Andersson L, Bodin MK, Sorensen S Progression of root resorption following replantation of human teeth after extended extra-oral storage. Endod Dent Traumatol. 1989; 5:38-47
Malmgren B, Cvek M, Lundberg M, Frykholm A Surgical treatment of ankylosed and infrapositioned reimplanted incisors in adolescents. Scand J Dent Res. 1994; 92:391-399
Malmgren B Decoronation: how, why, and when?. J Calif Dent Assoc. 2000; 28:846-854
Filippi A, Pohl Y, von Arx T Decoronation of an ankylosed tooth for preservation of alveolar bone prior to implant placement. Dent Traumatol. 2001; 17:93-95
Spontaneous alveolar bone growth in ankylosed, infraoccluded teeth in adolescents after elective decoronation – a clinical case series Muhammad Musaab Siddiqui Mital Patel Shakeel Shahdad Dental Update 2025 43:3, 206-210.
This article considers a possible solution to prevent or manage spontaneous alveolar bone growth in ankylosed, infraoccluded teeth in adolescents after elective decoronation, allowing replacement resorption to take place, preserving the surrounding alveolar bone and enabling vertical bone development coronal to the decoronated segment.
CPD/Clinical Relevance: To illustrate the advantages of decoronation allowing subsequent replacement of infraoccluded ankylosed teeth with implant-retained restorations and minimal aesthetic compromise.
Article
Intrusions and avulsions constitute 0.5–3% of all traumatic dental injuries.1 Ankylosis often occurs following late replantation or repositioning of avulsed or severely intruded teeth. This can hinder jaw growth and alveolus development resulting in:
One possible solution to prevent or manage these complications is to consider decoronation of the teeth and bury the root. This can allow replacement resorption to take place, preserving the surrounding alveolar bone and enabling vertical bone development coronal to the decoronated segment.3,4
Case description
Case 1
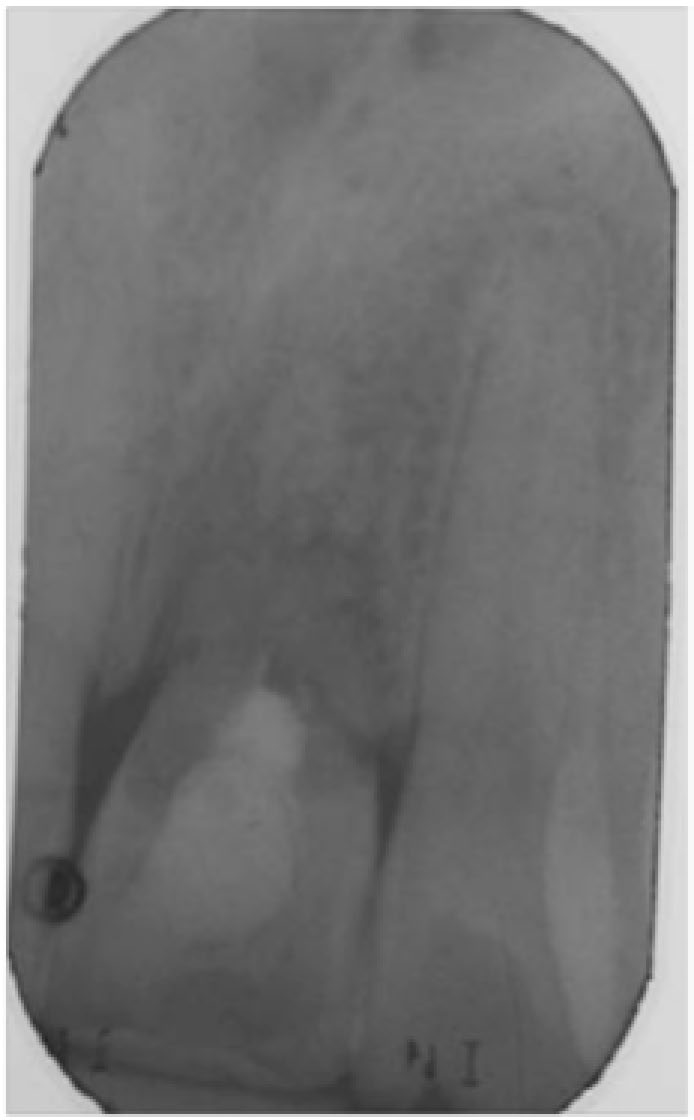
A 17-year-old male suffered avulsion of his UL1 at the age of 13. Following replantation, the tooth was discoloured and infraoccluded with compromised aesthetics (Figure 1a–k).
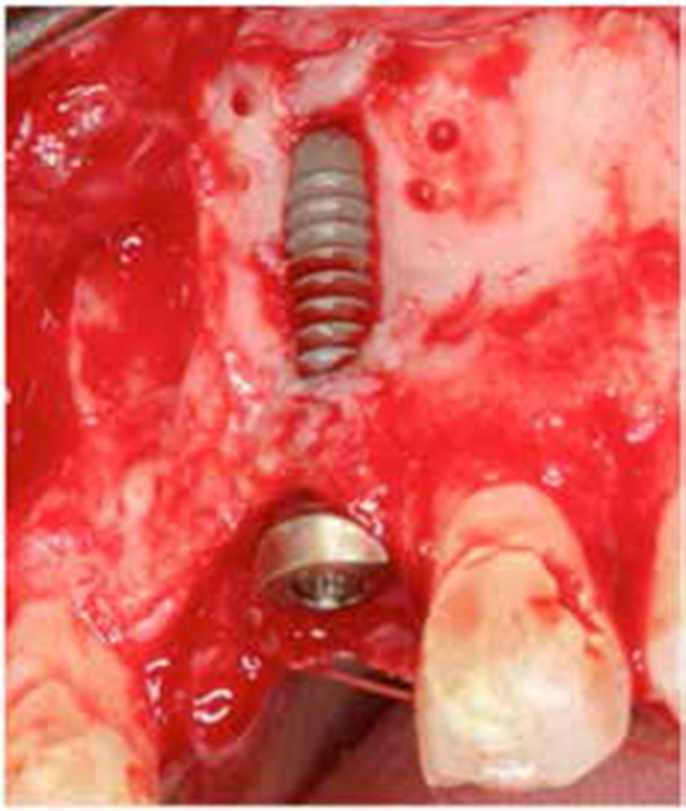
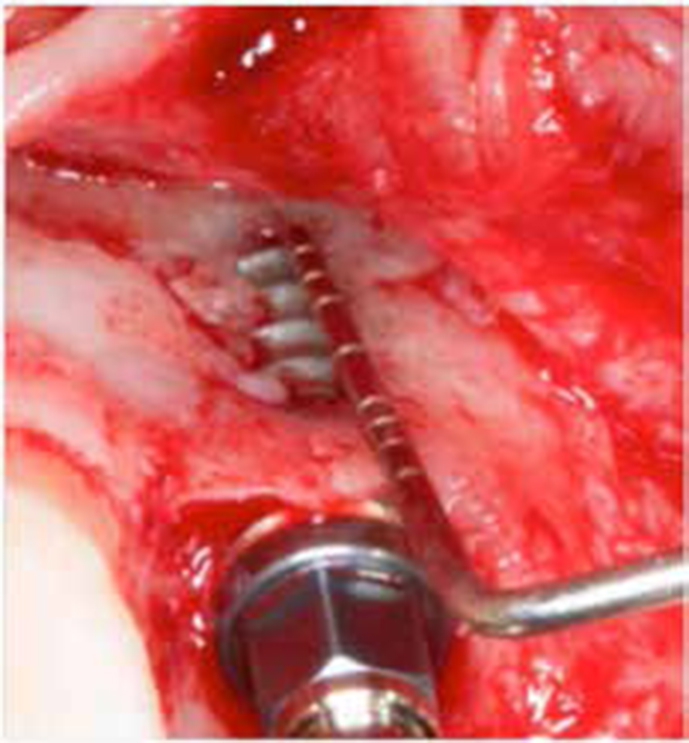
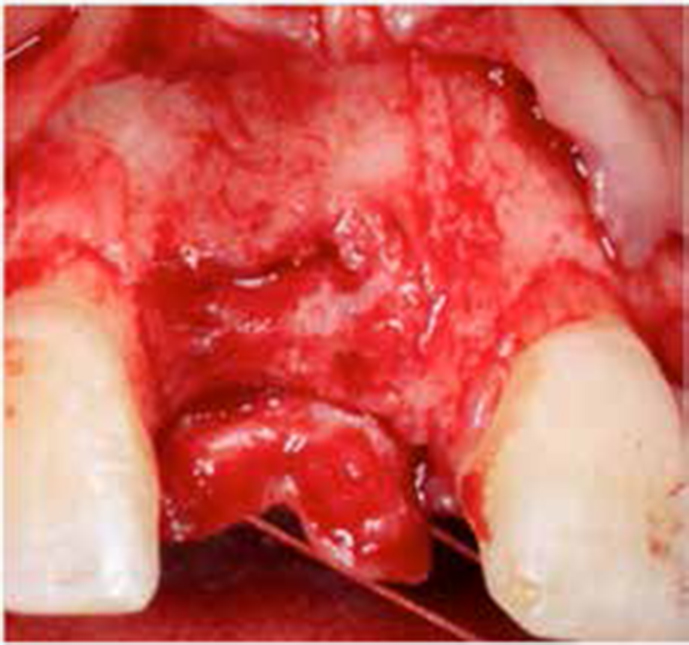
Figure 1.(a) Case 1: Infraocclusion after trauma; in occlusion.Figure 1.(b) Case 1: Discrepancy of 3 mm in gingival zenith between central incisors.Figure 1.(c) Case 1: Pre-op radiograph; external resorption visible.Figure 1.(d) Case 1: Gingival level 3 months after decoronation; labial view – no gingival discrepancy.Figure 1.(e) Case 1: Gingival level 3 months after decoronation; occlusal view.Figure 1.(f) Case 1: Post-decoronation radiograph.Figure 1.(g) Case 1: Site of decoronation, at the time of implant placement – remnant of root visible.Figure 1.(h) Case 1: Implant placement with the help of surgical guide.Figure 1.(i) Case 1: Simultaneous GBR for contour augmentation and correction of defect.Figure 1.(j) Case 1: Definitive screw-retained crown in place.Figure 1.(k) Case 1: Post-restoration radiograph.
Case 2
A 21-year-old male with traumatic luxation to UR1 which maintained a position labial and apical compared to the remaining anterior dentition. UL1 had avulsed and not replanted. Attempts at distraction using orthodontic forces to correct the vertical bone deficiency had failed. The aesthetics were challenging owing to missing centrals and space constraints (Figure 2a–k).
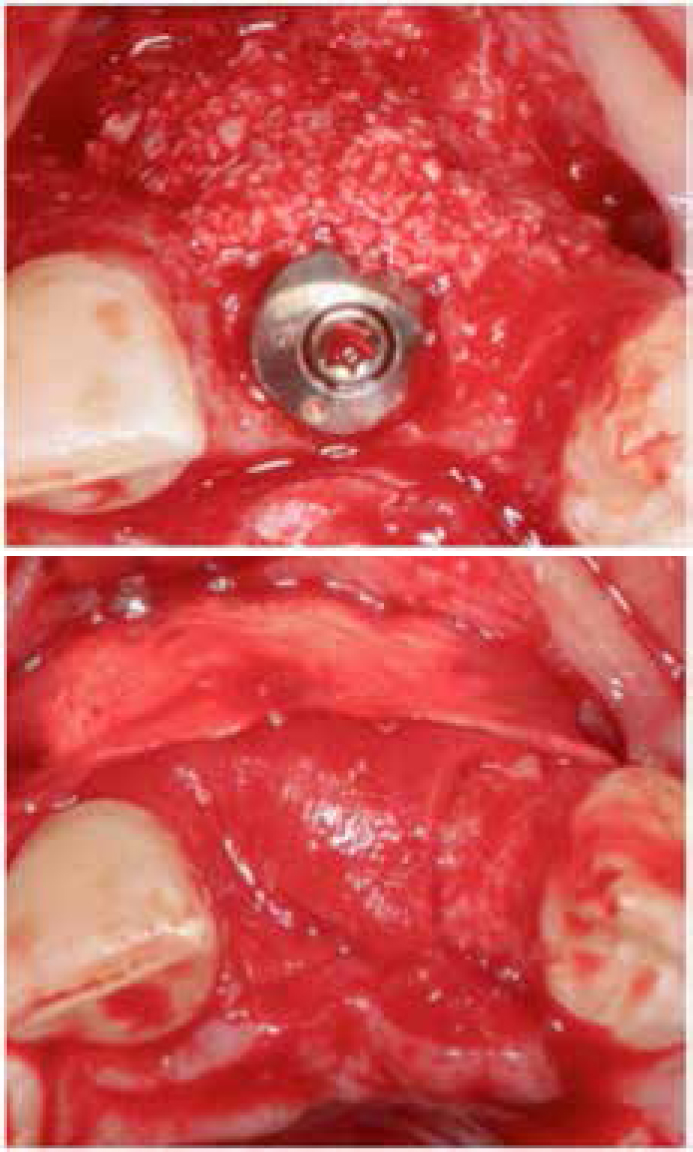
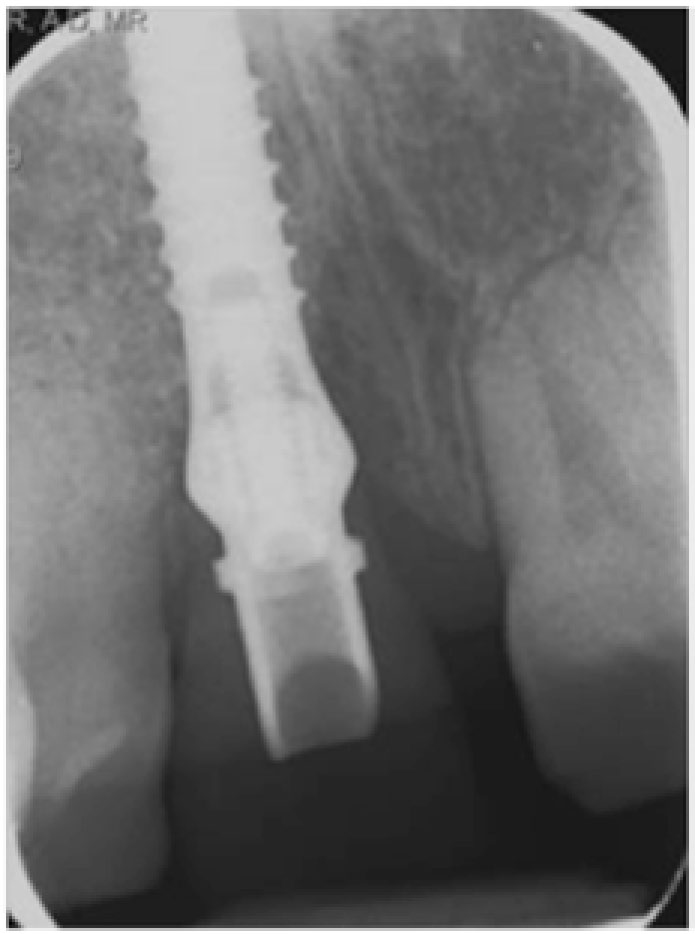
Figure 2.(a) Case 2: Discrepancy of 8 mm in gingival zenith between central incisor and adjacent lateral incisor.Figure 2.(b) Case 2: Infraocclusion after trauma, UL1 missing; in occlusion.Figure 2.(c) Case 2: Pre-decoronation radiograph.Figure 2.(d) Case 2: Post-decoronation; gingival level 2 years after decoronation: occlusal view.Figure 2.(e) Case 2: Post-decoronation: gingival discrepancy of 3 mm 2 years after decoronation – labial view.Figure 2.(f) Case 2: Post-decoronation radiograph after 2 years.Figure 2.(g) Case 2: Site of decoronation, at the time of implant placement – remnant of root visible.Figure 2.(h) Case 2: Osteotomy site preparation and implant placement with the help of surgical guide; corticotomy slots placed before GBR.Figure 2.(i) Case 2: Simultaneous GBR for contour augmentation and correction of defect. Crown lengthening performed on UL2 to reshape it as central incisor.Figure 2.(j) Case 2: Provisional crown in situ; no gingival discrepancy between central incisors.Figure 2.(k) Case 2: Post-restoration radiograph.
Case 3
A 22-year-old male suffered avulsion of UR1 at the age of 11. Following replantation, the tooth became infraoccluded due to ankylosis. Again, attempts at distraction using orthodontic forces to correct the vertical bone deficiency had failed (Figure 3a–j).
Figure 3.(a) Case 3: Orthodontic treatment before decoronation to manage space distribution.Figure 3.(b) Case 3: Discrepancy of 5 mm in gingival zenith between central incisors.Figure 3.(c) Case 3: Pre-decoronation radio-graphs – external resorption visible.Figure 3.(d) Case 3: Post-decoronation; gingival discrepancy of 1 mm 6 months after decoronation – labial view.Figure 3.(e) Case 3: Post-decoronation; gingival level 6 months after decoronation – occlusal view.Figure 3.(f) Case 3: Osteotomy site preparation and implant placement with the help of a surgical guide.Figure 3.(g) Case 3: Site of decoronation; horizontal bone loss noted.Figure 3.(h) Case 3: Simultaneous GBR for contour augmentation and correction of defect.Figure 3.(i) Case 3: Definitive screw-retained crown in situ – no discrepancy in gingival margin.Figure 3.(j) Case 3: Post-restoration radiograph.
Treatment
In all the three cases the crown was sectioned past the level of cemento-enamel junction, ensuring complete enamel removal.
In Cases 2 and 3, the pulp was extirpated and allowed to fill with blood coagulum to stimulate replacement resorption. In Case 1, most of the root had already been resorbed so endodontic intervention was not required.
Primary closure was achieved after periosteal relief in all cases.
All cases were monitored radiographically and clinically over 6–18 months.
Once there was evidence of sufficient alveolar growth and replacement resorption, implants were planned and placed.
Any remaining root fragments were removed at the time of surgery.
Simultaneous labial guided bone regeneration (GBR) was performed for horizontal width and contour augmentation.
No vertical augmentation was required.
Discussion
Ankylosis or replacement resorption leads to loss of the affected teeth but also interferes with alveolar bone growth.
Extraction in pre-adolescent period will lead to extensive bone loss, both in vertical and horizontal dimensions.
Extraction of ankylosed teeth can cause significant alveolar trauma.
Decoronation may be one of the optimal treatments for ankylosed teeth.4,5
Complete resorption of ankylosed teeth is predictable if enamel and the pulp were completely removed.3
Conclusions
Decoronation seems to maintain alveolar ridge and promote vertical alveolar growth in intruded, infraoccluded teeth.
These case reports illustrate improvement in soft and hard tissue profile after decoronation to facilitate ideal implant positioning.
Coronal bone apposition demonstrated in these cases enables optimal aesthetic outcome with implant restorations.
None of the cases required vertical bone augmentation to correct the vertical ridge deficiency.
Decoronation seems to be a clinically and cost-effective procedure in managing infraoccluded teeth when replacing with dental implants.
The success of decoronation supports replantation of avulsed teeth in children even if ankylosis is expected.