Article
Chronic periodontitis is characterized with destruction of the periodontal apparatus. It is classified as localized or generalized.1 It is further classified as mild, moderate or severe, according to the degree of the destruction of the periodontium.1,2 Several clinical parameters, such as bleeding on probing, periodontal pocket depth and clinical attachment level, are used in diagnosis of the disease.1,2,3 Treatment of chronic periodontitis involves oral hygiene education, scale and polish and root debridement, as well as regular evaluation and maintenance.1,3 However, when the periodontal disease has reached an advanced stage, the involved teeth cannot be retained and should be extracted.
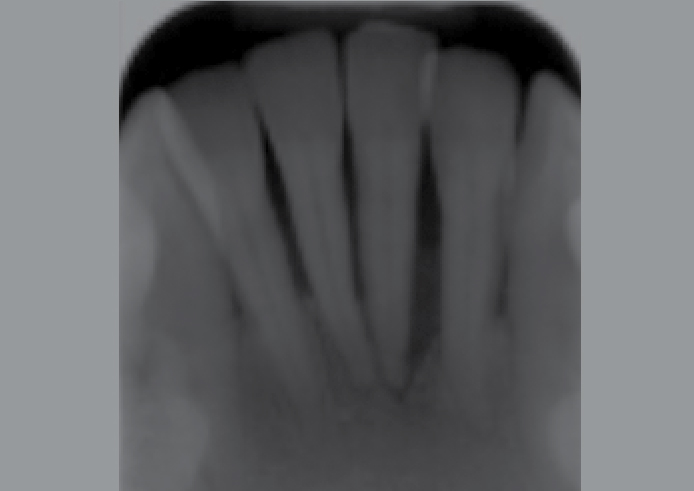
In this clinical tip, a 52-year-old female presented with a painful lower left central incisor. Clinical and radiographical examinations revealed the presence of moderate generalized chronic periodontitis, with a localized severe chronic periodontitis in the lower anterior region (Figures 1 and 2). The lower left central incisor was tender to percussion with grade III mobility. The patient was anxious to keep her teeth and to avoid wearing an immediate partial denture, replacing the lower left central incisor as proposed. One of the options, on which the patient agreed, was to extract the tooth and then re-fix it (as a pontic) to the neighbouring teeth using a composite resin restoration. The patient was made aware that the proposed treatment would be a provisional one and that a more permanent treatment may be required in the near future.

As part of the treatment, scale and polish and root debridement were carried out. A vinylpolysiloxane putty index was made to record the position of the lower anterior teeth in the dental arch and to aid in re-positioning the left central incisor into its right place during the fixation procedure. The lower left central incisor was then extracted and its root was amputated at about 2 mm apical to the cemento-enamel junction (Figure 3). The remnant of the neuro-vascular tissues were extirpated and filled with composite resin. The tooth was then shaped to resemble an ovate pontic. When the haemostasis was achieved, a rubber dam was placed across the six lower anterior teeth. The other five interior teeth were polished with pumice, etched and washed with copious water and then dried. The same procedure was completed for the extracted tooth. Using the putty index, the lower left central incisor was replaced in the arch and fixed to the two adjacent teeth, using composite resin on the facial surfaces of these teeth only at this stage (Figure 4). A bonding agent and composite resin filling were applied and light cured according to the manufacturer's instructions. The index was then removed and the position of the lower left central incisor and its neighbouring teeth in the arch was checked. Composite resin and Ribbond® (bondable reinforcement ribbon) (Ribbond Inc, Seattle, WA, USA) were placed on the lingual surface of the interior teeth4 (Figure 5). The composite resin was light cured and then finished and polished using composite finishing burs. The occlusion was checked and the use of inter-dental brushes and super-floss was demonstrated to the patient.


