Gunraj M Dental root resorption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 88:647-653
Del Fabbro M, Corbella S, Sequeira-Byron P Endodontic procedures for retreatment of peri-apical lesions. Cochrane Database Syst Rev. 2016; 10:(10) https://doi.org/10.1002/14651858.CD005511.pub3
Tandon J, Taneja S, Bhalla VK, Jain A Evaluation of bacterial reduction at various stages of endodontic retreatment after use of different disinfection regimens: an in vivo study. Eur Endod J. 2022; 7:210-216
Dotto L, Sarkis-Onofre R, Bacchi A, Pereira GKR The use of solvents for gutta percha dissolution/removal during endodontic retreatments: a scoping review. J Biomed Mater Res B Appl Biomater. 2021; 109:890-901 https://doi.org/10.1002/jbm.b.34753
Good ML, McCammon A An removal of gutta percha and root canal sealer: a literature review and an audit comparing current practice in dental schools. Dent Update. 2012; 39:703-708
Martos J, Gastal MT, Sommer L Dissolving efficacy of organic solvents on root canal sealers. Clin Oral Investig. 2006; 10:50-54
Oyama KO, Siqueira EL, Santos MD In vitro study of effect of solvent on root canal retreatment. Braz Dent J. 2002; 13:208-211
Ferreira I, Grenho L, Gomes P Efficacy and cytotoxicity of binary mixtures as root canal filling solvents. Materials. 2020; 13
Ribeiro DA, Matsumoto MA, Marques ME, Salvadori DM Biocompatibility of guttapercha solvents using in vitro mammalian test-system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:106-109
Wennberg A Biological evaluation of root canal sealers using in vitro and in vivo methods. J Endod. 1980; 6:784-787
Chang YC, Chou MY Cytotoxicity of halothane on human gingival fibroblast cultures in vitro. J Endod. 2001; 27:82-84
Vajrabhaya LO, Suwannawong SK, Kamolroongwarakul R, Pewklieng L Cytotoxicity evaluation of gutta percha solvents: chloroform and GP-Solvent (limonene). Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:756-759
Zaccaro Scelza MF, Lima Oliveira LR, Carvalho FB In vitro evaluation of macrophage viability after incubation in orange oil, eucalyptol, and chloroform. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:e24-27
Orange oil technique for gutta percha removal near open apices in root canal re-treatment M Ali M Tello Firas Elmsmari Abdul Rahman M Saleh Kelvin I Afrashtehfar Dental Update 2025 51:6, 443-446.
Authors
M Ali MTello
BDS, MFDS
Senior Resident in Endodontology, Postgraduate Studies, College of Dentistry, Ajman University, Ajman City, UAE
Division Lead and Assistant Professor in Endodontics, Department of Clinical Sciences, College of Dentistry, Ajman University, Ajman City, UAE; Visiting Faculty, Department of Endodontics, Faculty of Dentistry, Universitat Internacional de Catalunya, Barcelona, Spain
DDS, MDent, MSc, Dr med dent, PhD, FCGDent, FRCD(C), FDS RCS, ITI Fellow
Affiliate Clinical Faculty, College of Dentistry, Ajman University, Ajman City, UAE; Adjunct Research Professor, Department of Reconstructive Dentistry and Gerodontology, School of Dental Medicine, University of Bern, Bern, Switzerland
This clinical recommendation introduces a practical approach for the removal of gutta percha remnants near open apices in root canal retreatment using orange oil. This advice discusses the rationale for the technique, provides a step-by-step description, and outlines its advantages and limitations. This minimally invasive cost-effective approach offers dental practitioners greater effectiveness and safety in addressing the challenge of gutta percha removal near open apices.
CPD/Clinical Relevance: A minimally invasive cost-effective approach that offers effectiveness and safety when removing gutta percha near open apices is described.
Article
Apical lesions in root canal-treated mature teeth, especially in cases with suboptimal root canal treatment,1 are of concern as these lesions can progress into apical inflammatory root resorption, which in turn can lead to the formation of an open apex.2 When faced with such clinical scenarios, the choice of retreatment becomes crucial.3 This decision is driven by the need to prevent an unfavourable crown–root ratio and promote the healing process to preserve the integrity of the natural tooth and avoid an extraction.
Removing gutta percha from irregular root canals of root canal-treated teeth (RCTT) can be challenging, particularly when conventional methods using retreatment files may prove to be less effective. The inefficiency of these methods can potentially lead to excessive dentine removal, resulting in root weakening, canal transportation, or strip perforation. Moreover, there is a risk of extruding gutta percha beyond the open apex, which can trigger a foreign body reaction, potentially delaying or impeding the healing process or causing a flare-up that may necessitate apical surgery or lead to post-operative discomfort.4
When these gutta percha remnants remain at the apex of the RCTT, they may risk compromising the apical seal, regardless of whether gutta percha or a hydraulic cement is chosen to fill the root canals. This can reduce the success rate and, in some cases, conceal underlying necrotic tissue or bacteria. As such, addressing the challenge of gutta percha removal in irregular canals with open apices is of particular importance in maintaining effective root canal treatment outcomes.5
The objective of this clinical advice is to provide a practical approach for the thorough removal of gutta percha remnants near open apices in re-treatment procedures, specifically after initial bulk removal.
Clinical technique rationale
To address this challenge, the proposed technique uses orange oil to dissolve these remnants effectively without causing harm to the peri-apical tissues.
Initial scenario
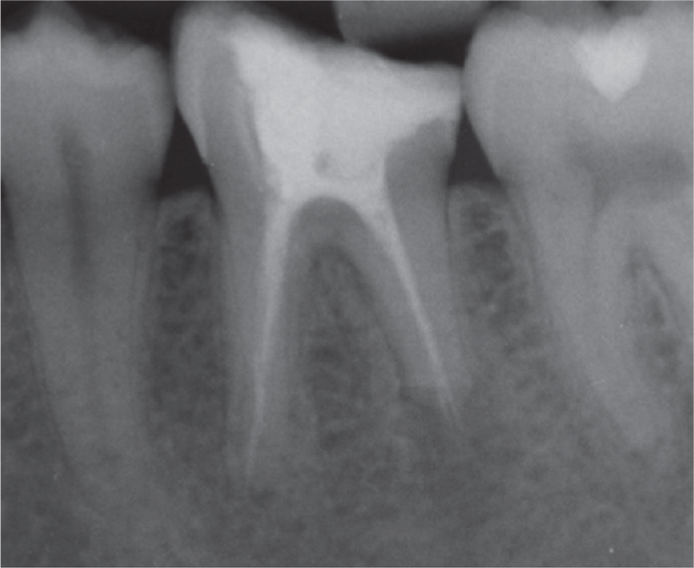
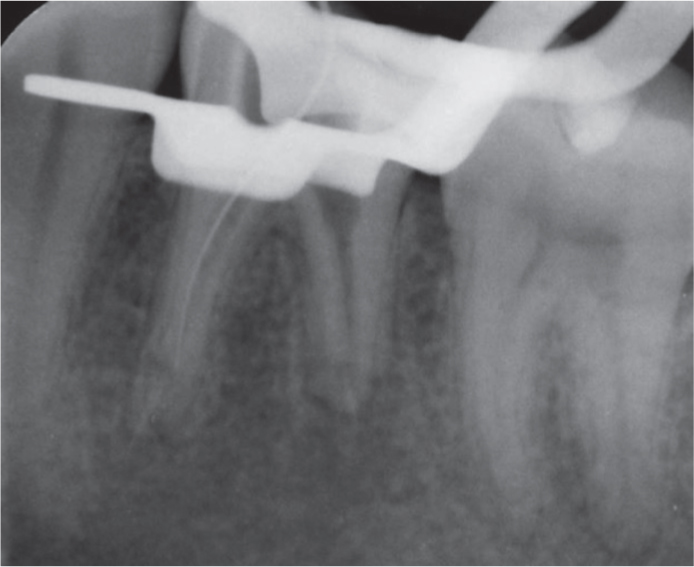
The pre-operative peri-apical radiograph reveals apical inflammatory root resorption, leading to an open apex with gutta percha extrusion (Figure 1). A residue of gutta percha remains in the apical region of the distal root, adjacent to the open apex, following the removal of the bulk of gutta percha material (Figure 2). This clinical scenario serves to describe the technique tip that can be adopted by general dental practitioners and specialists.
Figure 1. Pre-operative radiograph of lower left first molar with open apex and extruded gutta percha owing to apical inflammatory root resorption.Figure 2. Remaining gutta percha near the open apex in the distal root after bulk removal.
Technique description
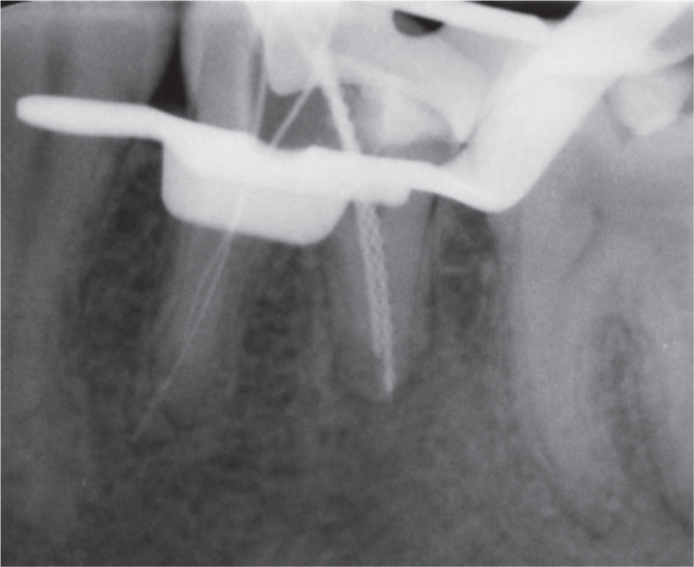
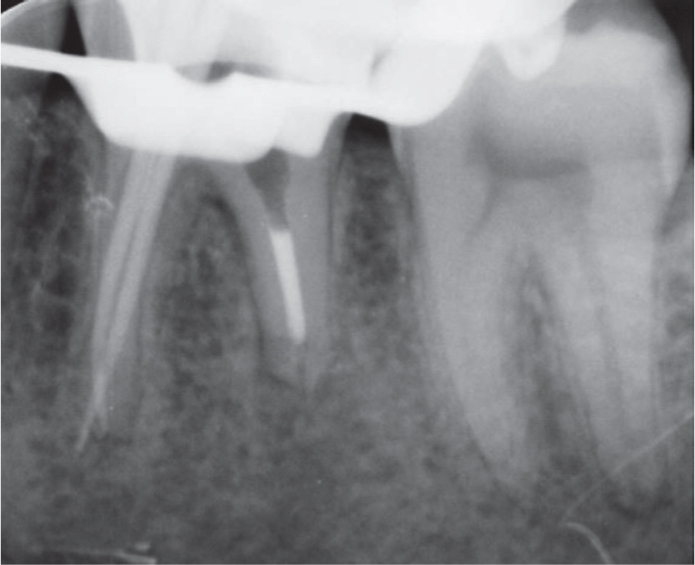
Start by estimating the distance on the radiograph from a reference point to the area where the gutta percha remnants are located (Figure 3).
Apply orange oil (orange guttane, 100% orange oil; Cerkamed, Poland) using a side-vented irrigation tip, positioning it approximately 2–3 mm from the open apex. Deliver approximately 1 ml, focusing on adequately filling the canal up to the orifice.
Improve the dissolution by using manual agitation or applying sonic activation. This procedure can be repeated as necessary, although typically once or twice is sufficient to clear the remnants.
Attach a flat-ended irrigation tip (EndoTech, Halifax, Canada) to a new 5-ml syringe. The use of a new syringe gives better visibility of the dissolved gutta percha within the orange oil.
Insert the tip of this needle to the same depth as the orange oil was delivered.
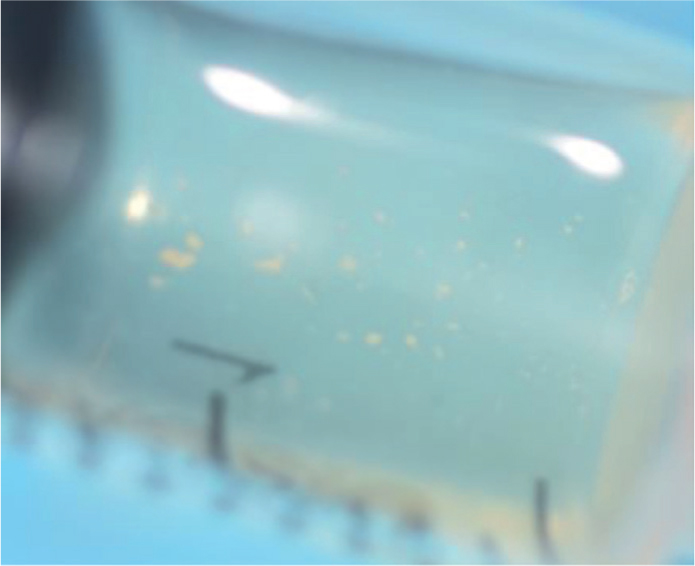
Apply negative pressure to withdraw the solution containing orange oil and dissolved gutta percha (Figure 4).
Take a radiograph to confirm the successful removal of these remnants. Following this confirmation, the re-treatment protocol can proceed in the usual manner (Figure 5).
Figure 3. Estimation of the distance from the reference point to the remnants using a large K-file.Figure 4. Aspirated orange oil with partially dissolved gutta percha remnants in a 5-ml syringe.Figure 5. Peri-apical radiograph displaying master cone gutta percha in the mesial canals and a distal MTA plug after successful removal of the previous gutta percha remnants.
Discussion
A recent scoping review highlighted a consistent presence of intracanal gutta percha remnants, with a higher frequency and increased abundance in the apical third of the root.6 To date, no technique has definitively outperformed conventional methods for the removal of gutta percha remnants in the apical third of the RCT roots.7,8,9 The proposed technique offers distinct advantages, ensuring a less invasive, more predictable, and cost-effective removal of these remnants. It requires only syringes, irrigation tips and a bottle of orange oil, along with the option for manual agitation or sonic activation.
Conversely, traditional solvents like chloroform, xylene, and halothane, while effective in dissolving gutta percha, can carry a risk to the peri-apical tissues, particularly in cases with an open apex.7 The proposed technique mitigates such risks, leading to more predictable outcomes with fewer complications or catastrophic events such as tooth loss.
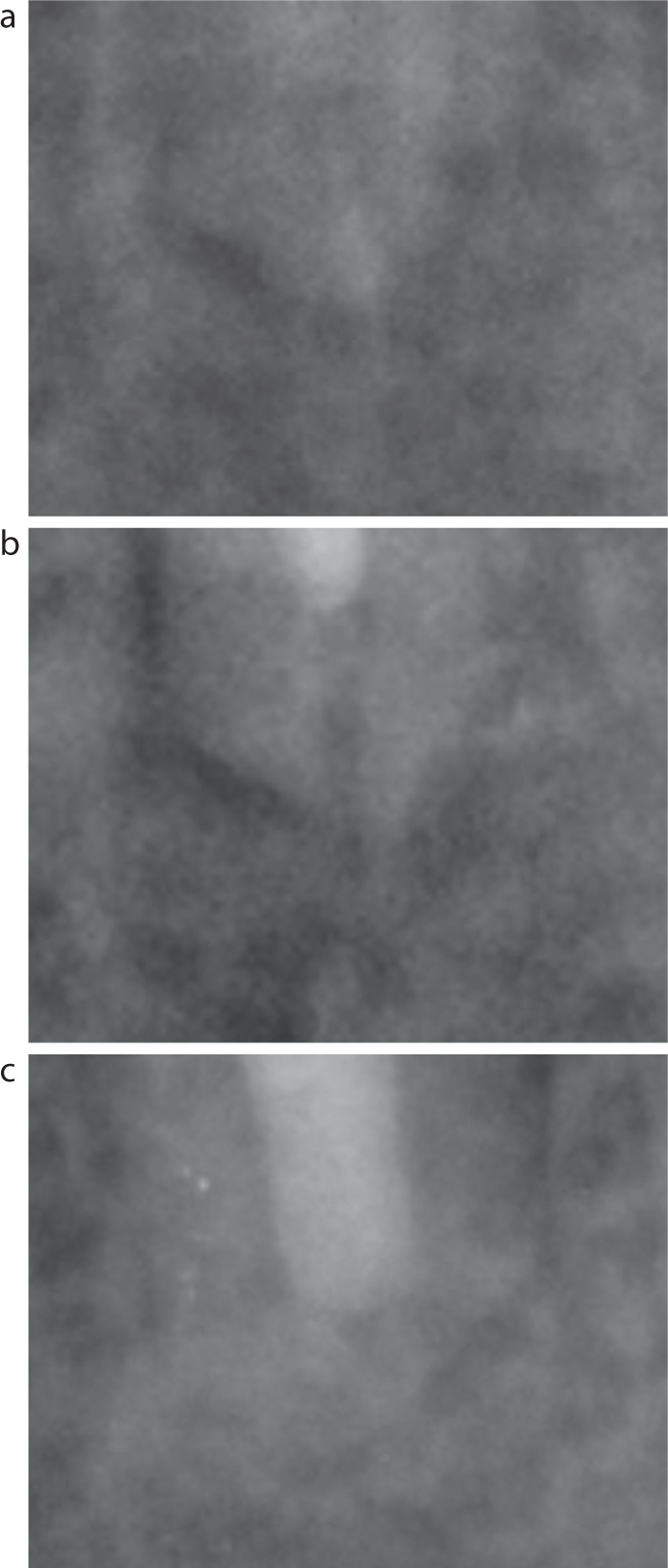
The cytotoxicity of chemical solvents, such as chloroform, has been extensively established through various in vitro and in vivo studies, while organic solvents, such as orange oil are recognized for their lower cytotoxicity and reduced potential harm to peri-apical tissues.8,9,10,11,12,13,14,15 Overall, this approach provides a valuable alternative for dental practitioners performing root canal re-treatment procedures, combining efficacy with safety, making it a compelling option in addressing the challenge of gutta percha removal near open apices (Figures 6 and 7).
Figure 6. Close-up peri-apical digital radiograph highlighting the area of interest within the peri-apical complex. (a) Residual gutta percha after bulk removal. (b) Apical region with MTA plug being gently condensed into the space where the gutta percha remnants were located before their removal. (c) 6-month follow-up demonstrating progressive bone formation, indicative of an ongoing healing process. For more information, see Figure 7.Figure 7. Additional information on the specific area of interest within the peri-apical complex discussed in Figure 6. (a) Distal root resorption is evident in an oblique pattern, with the buccal aspect being shorter than the lingual. (b) Residual gutta percha observed at the apical region on the wall. (c) Removal of gutta percha and placement of MTA plug (about to be pushed more apically). (d) MTA pushed up to the apex to the working length determined by the resorption pattern detected by CBCT and aided with an apex locator (Morita Root ZX2). (e) A 7-month follow-up reveals bone formation distally. (Follow-up CBCT can be justified after 1 year, based on AAE/AAOMR CBCT recommendations from 2017.
The practical limitations of the proposed technique should be acknowledged, however. First, achieving complete clearance of gutta percha remnants may sometimes necessitate multiple attempts. While the technique offers minimally invasive removal and predictability advantages, dental practitioners should be mindful that certain remnants may prove more resilient and require additional applications. Also, while an effective solvent for gutta percha, orange oil requires careful application because it can potentially damage or dissolve rubber dam used for tooth isolation.
Despite these limitations, the proposed approach presents a promising alternative for addressing the challenge of gutta percha removal near open apices. It balances efficacy and safety, making it a valuable option for general dental practitioners to address root canal re-treatment cases.
Conclusion
To sum up, the use of orange oil for gutta percha removal near open apices in root canal re-treatment is a cost-effective and practical technique. However, multiple attempts may be needed, and caution is advised to protect the rubber dam during application. This technique offers a promising balance between effectiveness and safety, improving predictability in complex endodontic cases.