Van'T Spijker A, Rodriguez JM, Kreulen CM, Bronkhorst EM, Bartlett DW, Creugers NHJ. Prevalence of tooth wear in adults. Int J Prosthodont. 2009; 22:35-42
Kelly M, Steele J, Nuttal N Adult Dental Health Survey – Oral Health in the United Kingdom.London: The Stationery Office; 2000
White D, Pitts NB, Steele J, Sadler K, Chadwick B. Disease and related disorders – a report from the Adult Dental Health Survey 2009.London: The Health and Social Care Information Centre; 2011
Kreulen CM, Van'T Spijker A, Rodriguez JM, Bronkhorst EM, Creugers NHJ, Bartlett DW. Systematic review of the prevalence of tooth wear in children and adolescents. Caries Res. 2010; 44:151-159
The glossary of prosthodontic terms. J Prosthet Dent. 2005; 94:10-92
Ommerborn MA, Schneider C, Giraki M Effects of an occlusal splint compared with cognitive-behavioral treatment on sleep bruxism activity. Eur J Oral Sci. 2007; 115:7-14
Clarke DJH, Reynolds PJ. Suggestive hypnotherapy for nocturnal bruxism: a pilot study. Am J Clin Hypn. 1991; 33:248-253
Goldberg G. The psychological, physiological and hypnotic approach to bruxism in the treatment of periodontal disease. J Am Soc Psychosom Dent Med. 1973; 20
Moufti MA, Lilico JT, Wassell RW. How to make a well-fitting stabilization splint. Dent Update. 2007; 34:398-408
Nohl FSA, King PA, Harley KE, Ibbetson RJ. Retrospective survey of resin-retained cast-metal palatal veneers for the treatment of anterior palatal tooth wear. Quintessence Int. 1997; 28:7-14
Murray MC, Brunton PA, Osborne-Smith K, Wilson NH. Canine risers: indications and techniques for their use. Eur J Prosthodont Restor Dent. 2001; 9:137-140
Davis WB, Winter PJ. The effect of abrasion on enamel and dentine and exposure to dietary acid. Br Dent J. 1980; 148:253-256
Beyer M, Reichert J, Bossert J, Sigusch BW, Watts DC, Jandt KD. Acids with an equivalent taste lead to different erosion of human dental enamel. Dent Mater. 2011; 27:1017-1023
Bartlett DW, Fares J, Shirodaria S, Chiu K, Ahmad N, Sherriff M. The association of tooth wear, diet and dietary habits in adults aged 18–30 years old. J Dent. 2011; 39:811-816
Jarvinen VK, Rytomaa II, Heinonen OP. Risk factors in dental erosion. J Dent Res. 1991; 70:942-947
Chander S, Rees J. Strategies for the prevention of erosive tooth surface loss. Dent Update. 2010; 37:12-18
Ren YF, Liu X, Fadel N, Malmstrom H, Barnes V, Xu T. Preventive effects of dentifrice containing 5000ppm fluoride against dental erosion in situ. J Dent. 2011; 39:672-678
Austin RS, Rodriguez JM, Dunne S, Moazzez R, Bartlett DW. The effect of increasing sodium fluoride concentrations on erosion and attrition of enamel and dentine in vitro. J Dent. 2010; 38:782-787
Hooper SM, Newcombe RG, Faller R, Eversole S, Addy M, West NX. The protective effects of toothpaste against erosion by orange juice: studies in situ and in vitro. J Dent. 2007; 35:476-481
Rahiotis C, Vougiouklakis G. Effect of a CPP-ACP agent on the demineralization and remineralization of dentine in vitro. J Dent. 35:695-698
Rees J, Loyn T, Chadwick B. Pronamel and tooth mousse: an initial assessment of erosion prevention in vitro. J Dent. 2007; 35:355-357
Bartlett D, Sundaram G, Moazzez R. Trial of protective effect of fissure sealants, in vivo, on the palatal surfaces of anterior teeth, in patients suffering from erosion. J Dent. 2011; 39:26-29
Bartlett D. Regurgitated acid as an explanation for tooth wear. Br Dent J. 1998; 185
Gregg T, Mace S, West NX, Addy M. A study in vitro of the abrasive effect of the tongue on enamel and dentine softened by acid erosion. Caries Res. 2004; 38:557-560
Aidi HE, Bronkhorst EM, Huysmans MCDNJM, Truin GJ. Factors associated with the incidence of erosive wear in upper incisors and lower first molars: a multifactorial approach. J Dent. 2011; 39:558-563
Ashcroft AT, Joiner A. Tooth cleaning and tooth wear: a review. Proc Inst Mech Eng J. 2010; 224:539-549
Azzopardi A, Bartlett DW, Watson TF, Smith BG. A literature review of the techniques to measure tooth wear and erosion. Eur J Prosthodont Restor Dent. 2000; 8:93-97
Burke FJT, Kelleher MGD, Wilson N, Bishop K. Introducing the concept of pragmatic esthetics, with special reference to the treatment of tooth wear. J Esthet Restor Dent. 2011; 23:277-293
Hurst D. What is the best way to restore the worn dentition?. Evid-Based Dent. 2011; 12:55-56
Johansson A, Johansson AK, Omar R, Carlsson GE. Rehabilitation of the worn dentition. J Oral Rehabil. 2008; 35:548-566
Hussey DL, Irwin CR, Kime DL. Treatment of anterior tooth wear with gold palatal veneers. Br Dent J. 1994; 176:422-425
Berry DC, Poole DF. Attrition: possible mechanisms of compensation. J Oral Rehabil. 1976; 3:201-206
Milosevic A. Tooth wear and compensatory mechanisms. Br Dent J. 1998; 185:209-210
Poyser NJ, Porter RW, Briggs PF, Chana HS, Kelleher MG. The Dahl Concept: past, present and future. Br Dent J. 2005; 198:669-676
Briggs PF, Bishop K, Djemal S. The clinical evolution of the ‘Dahl Principle’. Br Dent J. 1997; 183:171-176
Mizrahi B. A technique for simple and aesthetic treatment of anterior toothwear. Dent Update. 2004; 31:109-114
Poyser NJ, Briggs PF, Chana HS, Kelleher MG, Porter RW, Patel MM. The evaluation of direct composite restorations for the worn mandibular anterior dentition – clinical performance and patient satisfaction. J Oral Rehabil. 2007; 34:361-376
Redman CDJ, Hemmings KW, Good JA. The survival and clinical performance of resin-based composite restorations used to treat localised anterior tooth wear. Br Dent J. 2003; 194:566-572
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211
Hemmings KW, Darbar UR, Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293
Smales RJ, Berekally TL. Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Restor Dent. 2007; 15:2-6
Bartlett D, Sundaram G. An up to 3-year randomized clinical study comparing indirect and direct resin composites used to restore worn posterior teeth. Int J Prosthodont. 2006; 19:613-617
Burke FJ. Fracture resistance of teeth restored with dentin-bonded crowns: the effect of increased tooth preparation. Quintessence Int. 1996; 27:115-112
Burke FJT. Four year performance of dentine-bonded all-ceramic crowns. Br Dent J. 2007; 202:269-273
Chana H, Kelleher M, Briggs P, Hooper R. Clinical evaluation of resin-bonded gold alloy veneers. J Prosthet Dent. 2000; 83:294-300
Satterthwaite JD. Indirect restorations on teeth with reduced crown height. Dent Update. 2006; 33:210-216
Eder A, Wickens J. Surface treatment of gold alloys for resin adhesion. Quintessence Int. 1996; 27:35-40
Peachey A, Eder A, Ibbetson R, Pearson G. Surface treatment of alloys for resin adhesion: an in-vitro study. Clin Mater. 1994; 17:105-109
Rickman LJ, Satterthwaite JD. Considerations for the selection of a luting cement. Dent Update. 2010; 37:247-256
Rivera-Morales WC, Mohl ND. Restoration of the vertical dimension of occlusion in the severely worn dentition. Dent Clin North Am. 1992; 36:651-664
Setchell DJ. Conventional crown and bridgework. Br Dent J. 1999; 187:68-74
Stern N, Brayer L. Collapse of the occlusion – aetiology, symptomatology and treatment. J Oral Rehabil. 1975; 2:1-19
Hemmings KW, Howlett JA, Woodley NJ, Griffiths BM. Partial dentures for patients with advanced tooth wear. Dent Update. 1995; 22:52-59
Senior Lecturer/Hon Consultant in Restorative Dentistry, The University of Manchester, School of Dentistry, Higher Cambridge Street, Manchester M15 6FH
Tooth surface loss is becoming increasingly prevalent. Many cases can be managed with preventive measures, although there remain a number of patients for whom restorative intervention is indicated. Traditional treatment modalities have entailed extensive ‘full-mouth’ indirect restoration, although this approach has a number of disadvantages. Contemporary restorative techniques allow for a broader range of treatment options: this paper presents an overview of common issues and clinical techniques to overcome these.
Clinical Relevance: Treatment options and guidance for managing patients who present with tooth surface loss.
Article
Patterns of dental disease in populations are changing and the prevalence of toothwear/tooth surface loss (TSL) is increasing, both as a result of increased TSL seen in ageing populations,1 who have increased tooth retention rates compared to previous generations, and also an increase in the prevalence of TSL in younger populations.2–4 The latest UK Adult Dental Health Survey3 highlighted that 77% of dentate adults exhibited TSL extending into dentine.
The pathological loss of tooth structure may be caused by a single causative factor or, more commonly, by an interplay of factors, these being:5
Erosion: the progressive loss of tooth substance by chemical processes that do not involve bacterial action.
Abrasion: an abnormal wearing away of the tooth substance by causes other than mastication.
Attrition: the mechanical wear resulting from mastication or parafunction, limited to contacting surfaces of the teeth.
In addition to the above, abfraction (the pathologic loss of hard tooth substance caused by biomechanical loading forces due to flexure and chemical fatigue degradation of enamel and/or dentine at some location distant from the actual point of loading) may cause loss of tooth structure in cervical regions. A key step in the management of patients with TSL is to determine the primary causative factor and institute an appropriate preventive regime to check further deterioration of the dentition: any treatment without prevention is likely to fail.
It is axiomatic that a key element of prevention is that of removing the cause – in cases of abrasion, this is usually straightforward removal of the exogenous ‘agent’. For attrition, it is more difficult to stop parafunction (such as bruxism habit); in essence, the parafunction is often a centrally mediated response to life stressors and the use of cognitive behavioural therapy and alternative therapies (such as hypnosis) have shown some benefit.6–8 However, in many cases, the ‘next best’ approach is to provide a stabilization splint9 such that this, rather than opposing teeth, is being worn down (Figure 1). An alternative or additional step is to prevent wear of posterior teeth by increasing the posterior disclusion during excursive movements. This is easily done with canine risers, which can be made either indirectly10,11 or very simply from direct application of composite resin, to restore canine bulk palatally and height incisally with no preparation. The evidence base to support the use of such canine risers is limited, but the treatment is well tolerated and when direct composite is used it is easily reversible if there are any problems of adaptation.
Figure 1. Stabilization splint for maxillary arch.
The potential of dietary acids to lead to erosive TSL has long been recognized,12 with recent insights into dietary habits highlighting the relative effects of different food and drink, and habits such as swilling, and confirming the role of frequency of acidic challenge.13–15 Dietary analysis (using a diet ‘diary’) is helpful to identify such factors. Symptoms of gastric problems (eg gastric oesophageal reflux disorder) or the presence of eating disorders will require liaison with a patient's general medical practitioner to address the intrinsic acid. The prevention of erosive TSL has been covered in-depth elsewhere in this journal.16 The use of fluoride to reduce susceptibility to erosion and aid remineralization has a key role and commencement on a fluoride regime should be an integral part of prevention. Although some studies show a potential benefit of high fluoride concentrations,17 increased fluoride concentrations do not necessarily confer greater benefit, especially to exposed dentine.18 However, some newer agents (eg Pronamel, GSK, Weybridge; Tooth Mousse, GC Dental, Newport Pagnell; Pro-Expert, P&G, Weybridge) have been shown to provide enhanced resistance to acidic challenge.19–21 Additionally, the use of sealant resins on exposed dentine can confer some protection from further TSL.22
Although diagnosis is essential in each case, the multi-factorial nature of TSL can make a definitive diagnosis difficult – in many cases, where diagnosis is uncertain and when dietary analysis does not highlight an obvious extrinsic source of acid, the likelihood is that intrinsic erosion (due to undiagnosed GORD) is a factor.23 Similarly, the ‘classic’ appearance of TSL due to intrinsic acid (that of worn palatal surfaces of maxillary teeth) has been challenged24,25 and erosion may present as TSL on a variety of surfaces. Moreover, it has also been argued that enamel is only vulnerable to wear if it has been softened by exposure to acid.26 Therefore, even when erosion is not considered to be the primary causative factor, thought should still be given to recommending a fluoride regime.
Intervention threshold
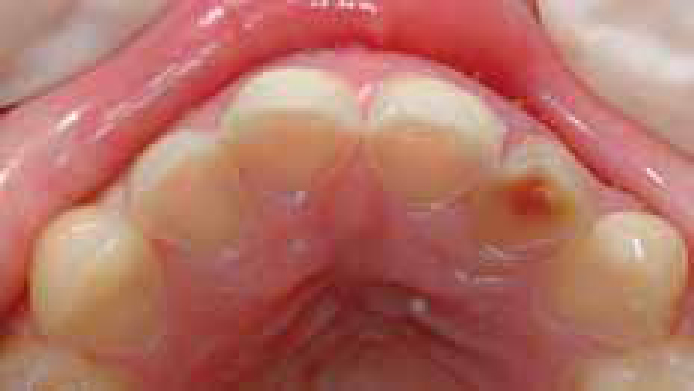
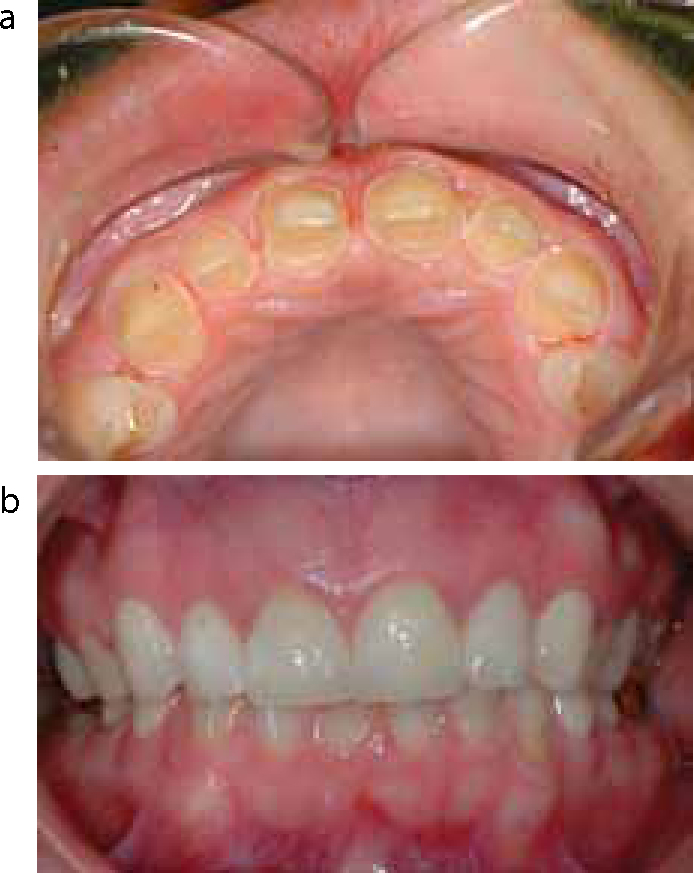
In many, if not most, patients with TSL the rate of deterioration is slow and a conservative approach with minimal, if any, restorative intervention is appropriate. In such cases it is paramount that a preventive regime (as above) is instituted and that monitoring of progression is undertaken. Such monitoring can take the form of serial study casts (eg six-monthly), clinical photographs, silicone indices or clinical indices.27 Where symptoms (typically sensitivity) exist that cannot be controlled through the use of fluoride/desensitizing agents, then restorative intervention may be warranted, but this may be able to be restricted simply to restoration of isolated defects of exposed dentine. Similarly, where ‘classic’ cupped erosive defects exist, it is sensible to restore these to prevent pooling during subsequent acid exposure and protect the dentine from further TSL (Figure 2). A further typical situation where minimal intervention is of benefit is where there is TSL affecting maxillary anterior teeth which have become ‘thinned’ to the extent that incisal enamel chipping occurs and is at risk of further fracture or is presenting sharp edges (Figure 3): in this situation application of a small amount of resin composite will prevent future fracture (flowable composite is convenient in many such cases).
Figure 2. Localized erosion with ‘cupped’ defects on molar occlusal surfaces.Figure 3. Mild TSL of anterior teeth but with thin incisal enamel liable to further fracture.
The requirement for more definitive restorative intervention is not always clear and is an interplay between the patient's needs/concerns, the perceived implications of progression and also the severity of TSL. With regards to patient needs, these may relate to functional or aesthetic concerns, although many patients only present when the latter issue becomes a problem (Figure 4). When there is concern that progression of TSL may lead to further complications, such as pulpal exposure (Figure 5), or may increase complexity of treatment (or even make treatment not possible) then more definitive treatment is indicated: this may be generalized as including those cases where significant amounts of dentine are exposed. In many cases, simple restoration with direct composite may be possible and a pragmatic approach with (relatively) limited treatment goals may also be appropriate;28 given that there is a lack of evidence to guide treatment choices in patients with TSL,29,30 pragmatic approaches with minimal intervention where possible are wise. Whatever the treatment goal, prior to restorative intervention consideration of typical challenges and potential solutions is required: a full guide to management of TSL is clearly beyond the scope of a single short article, although what follows is a brief outline of some common challenges and solutions that may prove helpful in the management of patients with TSL.
Figure 4. Patient with TSL complaining of poor aesthetics - note limited smile (compare to Figure 15).Figure 5. TSL of palatal aspect of anterior teeth: the proximity of the pulpal tissues is readily apparent on several of the incisors.
Consequences of toothwear and implications for restorative management
Typical problems may obviously vary depending on whether a patient presents with localized or generalized TSL, and also whether the patient is mostly/fully dentate or partially dentate (that is, multiple missing opposing units). There are, however, common ‘themes’ across these different presentations.
Loss of tooth form and posterior stability
Notwithstanding the aesthetic effects of TSL, particularly when anterior teeth are affected, TSL of posterior teeth leads to loss of the natural tooth anatomy and cuspal form which, in turn, leads to a less stable intercuspal position (ICP). This reduced ‘posterior stability’, together with TSL of anterior teeth and reduced anterior guidance, may lead to a forward postural and functional position with adoption of an edge-edge incisal relationship (pseudo Class III) and subsequent anterior toothwear (Figure 6) owing to lack of posterior disclusion and simultaneous functioning on anterior and posterior teeth. Conceptually, this is distinct to a discrepancy between the retruded contact position (RCP) and ICP and is more related to the lack of stability of the existing ICP. This presentation may be seen even with relatively mild wear and may be managed with intervention only to anterior teeth to restore incisal guidance. However, anterior restorations will be more prone to failure without a concurrent increase in posterior stability. Retention of direct composite in situations where anterior teeth require mainly or only incisal build-up may prove problematic, particularly with a background of attritive TSL – in such cases restoration of incisal edges and subsequent placement of adhesive (gold) palatal veneers to ‘protect’ the composite may prove helpful31 (Figure 7). Opinions vary regarding the relative importance of providing posterior stability and also the most appropriate restorative material to achieve this, as aptly demonstrated during recent interactive treatment planning discussions at the British Society of Prosthodontics (BSSPD) sessions at the Second Pan Dental Society Conference. However, it is this author's view that, in many cases of TSL where there is a need to restore posterior teeth, the durable restoration of two pairs of occluding molars (typically all four first molars) through provision of adhesive gold onlays with minimal preparation (see below) has much to commend it, either in isolation or as part of a broader treatment plan.
Figure 6. Relatively mild TSL but with adoption of edge-edge functional position and anterior TSL.Figure 7. Adhesive palatal gold veneers placed with concurrent incisal build-up with composite.
Dento-alveolar compensation and short teeth
When teeth lose tooth structure, the ‘space’ of lost tooth tissue is rarely left owing to dento-alveolar compensation that typically occurs in conjunction with progressive TSL.32,33 Thus teeth may have short clinical crown heights and require restoration yet still be in functional contact with the opposing dentition; here problems present related to retention of any restoration and also related to maintaining pulpal health: the conventional method of obtaining space, ie removal of tooth structure with preparation, is likely to be injurious to the pulp or could even expose the pulp.
Methods to create space
Where TSL is localized to anterior teeth, space for restoration is typically required palatally and incisally. In such situations, it is often suggested that equilibration of the occlusion with RCP and ICP coincident will allow this space to be created. However, this approach entails removal of further tooth structure, which is difficult to justify in a patient whose presenting problem is that of loss of tooth structure. It is difficult to obtain stability in the newly established ICP, and the amount of space created is rarely sufficient to enable restoration: such an approach, therefore, seems hard to recommend. A more appropriate method for obtaining space is to undertake localized axial tooth movement utilizing the ‘Dahl concept’. The Dahl concept has been reviewed in depth elsewhere34,35 and has evolved from the use of a removable appliance (Figure 8) to the use of direct or indirect restorations.
Figure 8. Removable Dahl appliance to create space anteriorly.
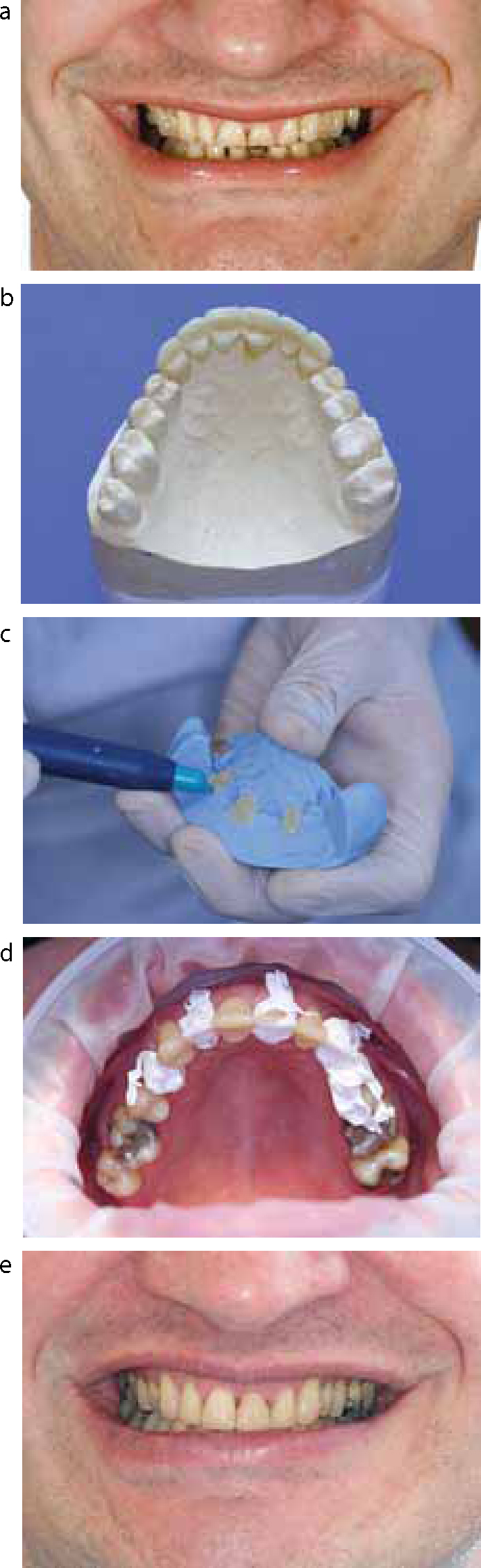
Use of direct composite to provide axial tooth movement is straightforward in most cases of anterior TSL. It is important that anterior teeth are built up not to recreate natural anatomy but with a more prominent cingulum to provide a flat ‘centric stop’ such that functional forces are directed axially. The use of a diagnostic wax-up and duplication of this to use as a matrix to ‘preview’ the intended outcome with a provisional material (Figure 9) and guide placement of composite is invaluable. A detailed guide of this technique using translucent stents and an ‘every other tooth’ technique has been previously published in this journal.36 Opaque silicone putty is readily and conveniently available and can also be used as a matrix, but in this case it is important to note that the resin-composite will need to be polymerized through the tooth structure with subsequent attenuation of the light intensity. If such a technique is adopted, a high power curing light is essential, as is further curing of the composite following removal of the matrix (Figure 10). An alternative to the ‘every other tooth’ technique is to use sections of metal matrix strip interproximally, embedded in the silicone (Figure 11): finishing and polishing is, however, more difficult in such cases.
Figure 9. Mock trial of intended outcome using provisional material and silicone matrix (same patient as Figure 6).Figure 10. Direct composite build-up of maxillary anterior teeth to utilize Dahl concept: (a) teeth at presentation; (b) diagnostic wax-up - note overbuilt cingulum region; (c) silicone matrix providing palatal contour and incisal edge being filled with composite for every other tooth; (d) all six teeth now built up palatally with the three teeth restored in ‘first wave’ covered with PTFE tape; (e) result after placing labial composite.Figure 11. Alternative matrix with interproximal separating strips inserted.
During the phase of tooth movement, the restorations will be subjected to the entire occlusal functional load and some chipping or deterioration of the composite restorations is to be expected, however, following re-establishment of the posterior occlusion, the restorations typically remain serviceable as the definitive restoration, with only simple polishing or minimal refurbishment. It is for this reason that individual restorations rather than splinted restorations are essential. Concerns regarding splaying of anterior teeth are largely unwarranted provided the palatal form is appropriate. These restorations have been shown to have good medium term survival (median survival of ~5years) for both maxillary and mandibular teeth.37–40 When failure does occur, further direct repair is often possible. When a need for more robust restoration arises, ie a full coverage crown, the use of these ‘medium’ term restorations will have made this subsequent treatment easier and will also have enhanced the ‘life cycle’ of the tooth. Given the good survival, it is difficult to recommend full-coverage restorations as part of the initial treatment plan, and in many cases it is wiser to delay the final decision until after the posterior occlusion has re-established. However, in cases where there will be a clear need for subsequent crowns and thus separated restorations are not required, splinted composite restorations are much easier to provide and even more so if a combined indirect/direct technique is used, with the palatal contour formed indirectly and only the labial aspect left to be built up by hand (Figure 12).
Figure 12. Combined direct/indirect technique: (a) indirect splinted palatal composite veneer about to be cemented to teeth; (b) labial composite being placed following placement of indirect palatal composite; (c) result after placement of labial composite (note posterior separation).
Generalized TSL and direct composite
In cases of generalized TSL, where the majority of teeth would best be served by restoration, space is best obtained by increasing the occlusal vertical dimension (OVD) and providing full-arch or full-mouth restoration (see also decreased OVD below). This approach is often very extensive and technically demanding, not to mention potentially costly. The common approach when a full mouth restoration is contemplated is to assume automatically that teeth will require indirect restorations and that these will be full-coverage crowns. It is, however, uncommon for a patient with TSL to require the majority of teeth to be restored with full coverage crowns and, although published case reports of such treatments abound, the wholesale preparation of teeth and removal of further tooth structure in a patient who presents with TSL is unjustified: many such cases can be restored with direct composite alone or in conjunction with adhesive indirect restorations.
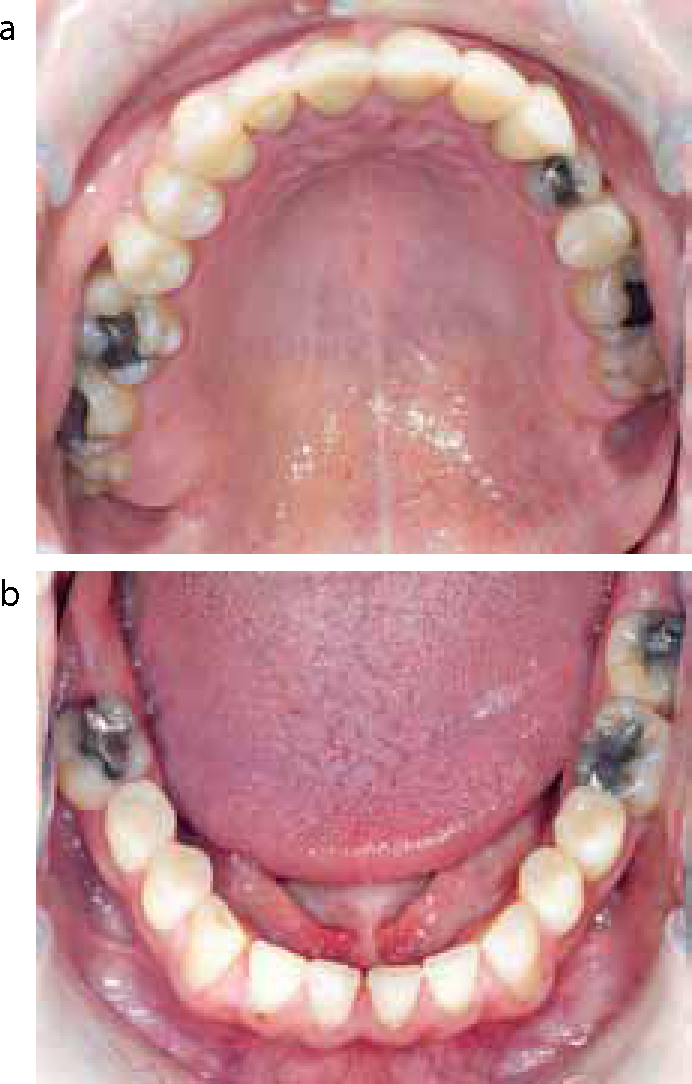
Survival of composite ‘reconstructions’ has been shown to be reasonable and, as argued above, for the use of composite anteriorly, future failure can be managed much more easily and the life-cycle of teeth extended:41 a matrix can prove very helpful to establish appropriate contour, particularly of the occlusal aspects of teeth (Figures 13 and 14) in a similar fashion to their use described above for build-up of anterior teeth. Whether considering anterior or posterior teeth, a ‘ring’ of enamel to which to bond gives more predictable bonding – this is often present in patients with TSL, perhaps owing to some protective effect of the gingival crevicular fluid. There is limited but conflicting evidence regarding the use of composite restorations, whether direct or indirect, to restore posterior teeth;41,42 however, a balance needs to be made between treatment options that have a low ‘cost’ to the tooth (in terms of loss of tooth structure and little iatrogenic harm to pulpal tissues) but high maintenance and those treatment options that may well have better survival, but at the cost of loss of tooth structure owing to the preparation required and potentially catastrophic failure.
Figure 13. Restoration of incisors, canines and premolars with direct composite: (a) maxilla; (b) mandible.Figure 14. Restoration of premolars and molars with direct composite: (a) at presentation; (b) after restoration.
If composite restorations are restricted primarily for restoration of axial contours of teeth and for restoration of functional surfaces of premolar teeth (generally not functional surfaces of molars) and are placed as part of a planned treatment, with the occlusal scheme providing good posterior stability (perhaps with indirect onlays – see below) and posterior disclusion on excursive movements (discussed above), then a positive treatment outcome is likely.
Even when there is a need for indirect restoration, the use of direct composite can be invaluable during the provisionalization phase and this ‘stepping-stone’ phase may be extended for the convenience of the patient or dentist to break up what is otherwise extensive treatment (Figure 15). In cases where direct composite will not achieve the treatment aims, extensive preparation of teeth should still be avoided where possible and minimal preparation and adhesive techniques employed.
Figure 15. Result immediately after placing ‘full-mouth’ direct composite as long-term provisional restoration (same patient as Figure 4 - note difference in smile line).
Minimal preparation and adhesive indirect restoration
In many patients with TSL the use of adhesive restorations can overcome a number of issues including:
The increased impact of preparation of teeth and further loss of tooth structure where residual tooth structure is already at a premium.
The desire to avoid conventional preparation and thus reduce the biological impact on teeth.
The limited height of teeth that, after preparation, would yield insufficient retention or resistance form.
In situations where it is simply too difficult to achieve full correct contour with direct composite restoration of posterior teeth, provision of an indirect composite can overcome these problems, although often minimal preparation is helpful to aid accurate seating of the restoration and/or achieve a margin that is amenable to finishing. Similarly, ceramic restorations may be etched with hydrofluoric acid, silane-treated and bonded with resin-based luting cement and used as an alternative aesthetic adhesive onlay (Figure 16). Both these techniques are particularly suited to restoration of premolars, although the improved aesthetics and durability of porcelain is somewhat offset by the slightly greater bulk of material required and greater difficulties in repair and maintenance when failure does occur. Similarly, the use of ceramic in thin sections with minimal preparation may be appropriate for anterior teeth requiring full-coverage crowns as an alternative to ‘traditional’ crowns (Figure 17). Such resin-bonded crowns (RBCs) have good survival and excellent aesthetics.43,44 In cases where there is concern regarding the amount of force that these restorations may be subjected to, for example TSL due to attrition/bruxism, then a reasonable compromise is to use stronger more durable crowns, for example porcelain fused to metal crowns with metal guiding surfaces, but to restrict these to canines and use RBCs for incisors, ensuring shared guidance on protrusion. There is scant evidence regarding their suitability for use on posterior teeth and thus they should be used posteriorly with caution, although the author has used RBCs successfully on premolars with good results in patients where posterior stability is good and attrition/bruxism is not a factor.
Figure 16. Porcelain onlays used to restore maxillary premolars as part of an integrated treatment plan.Figure 17. RBCs used to restore maxillary anterior teeth: (a) preparation (palatal tooth structure had minimal alteration from condition at presentation); (b) restorations at 3 years (same patient as Figure 16).
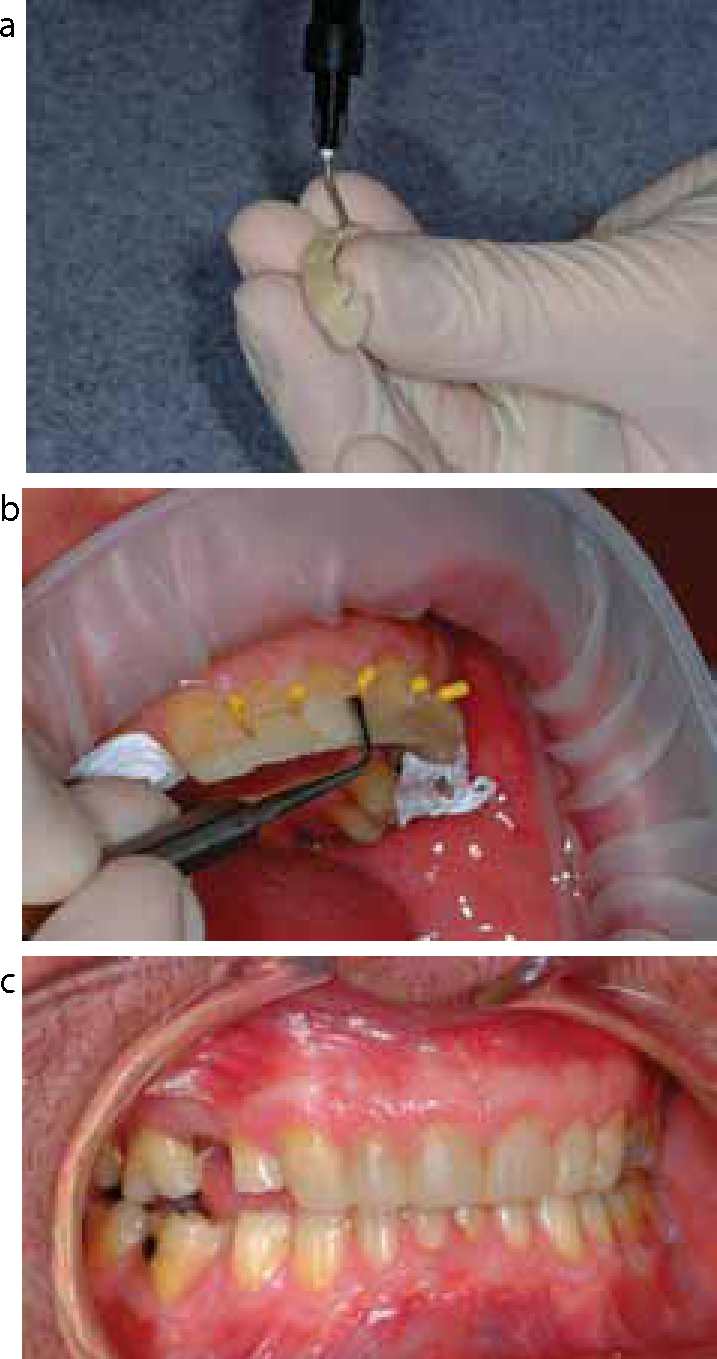
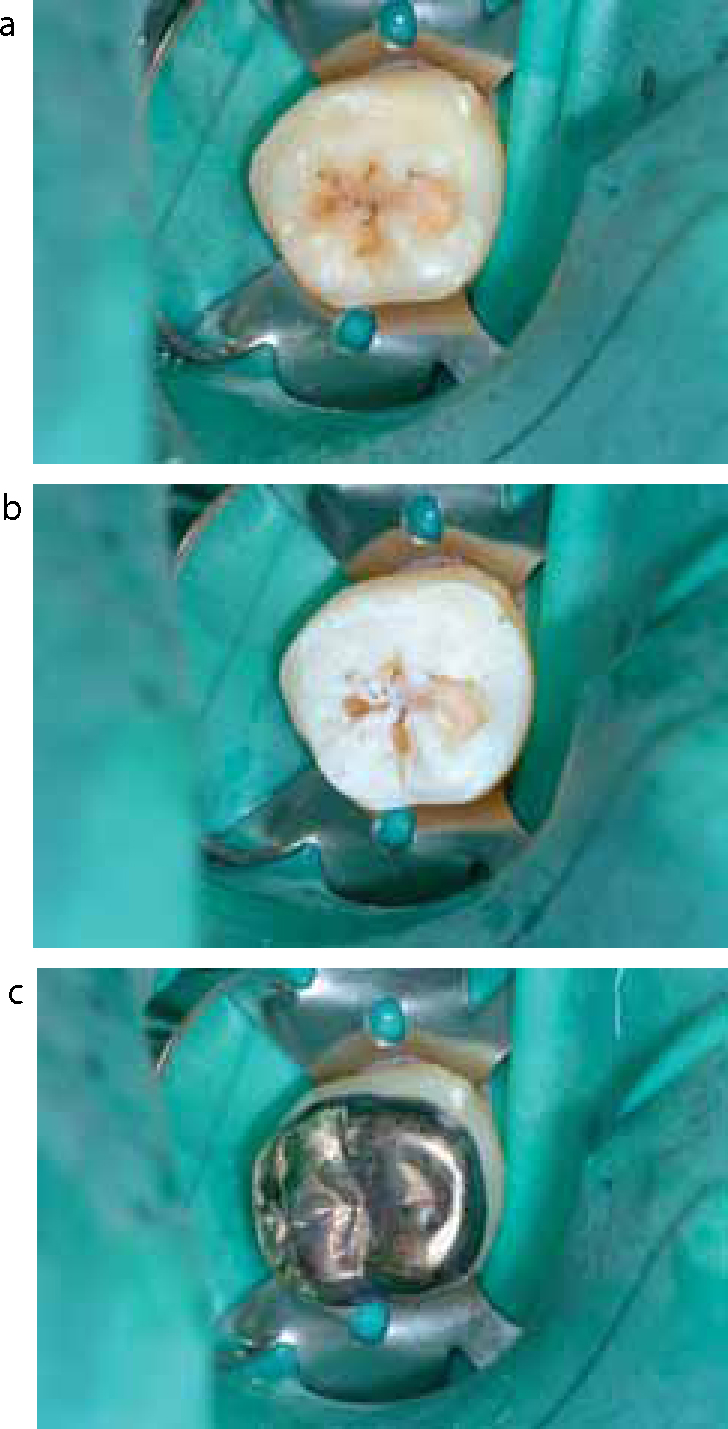
A convenient and conservative means by which to provide durable posterior stability is through the use of adhesive gold onlays to restore molars with minimal preparation45,46(Figure 18). A variety of methods have been employed to bond gold alloys to tooth structure, whether for molars or for anterior palatal veneers, as described above: the simplest of these is alumina-blasting, however, heat-treatment to produce an oxide layer provides a more effective solution.47,48 Whichever technique is employed, it is important that a bi-functional resin is used (for example Panavia F, Kuraray, Osaka, Japan).49
Figure 18. Adhesive gold onlay for a molar tooth: (a) minimal preparation; (b) etched tooth showing minimal extension into dentine; (c) cemented heat-treated gold onlay.
Decreased OVD and gross wear
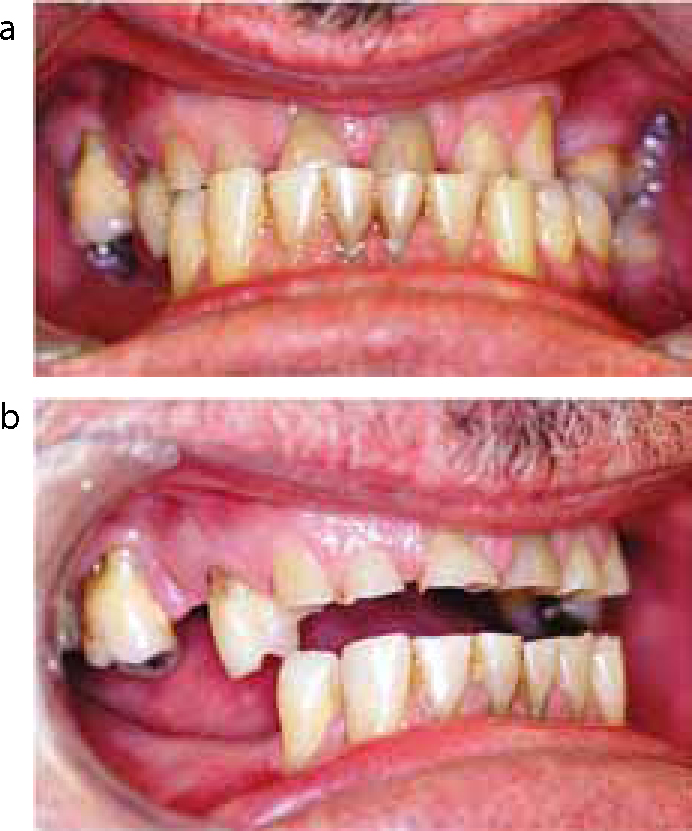
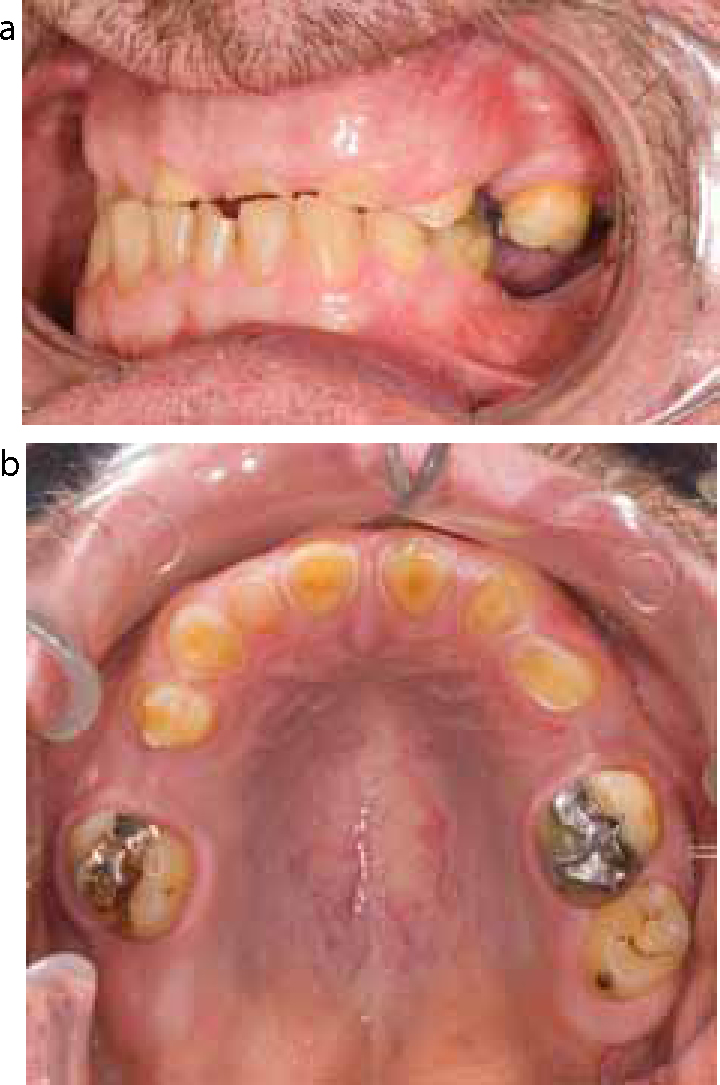
If the rate of TSL is such that it progresses quicker than dento-alveolar compensation occurs, then a decrease in the OVD may be seen. The relevance of this in dentate patients is debatable; such a presentation may lead to a more extensive treatment plan entailing full-mouth or full-arch reconstruction at an increased OVD, but traditional arguments relating to tolerance (or otherwise) of such an increase are likely to be of little relevance in mostly/fully dentate patients where any restoration is all tooth supported.50,51 However, the situation in partially dentate patients who will require mucosal supported tooth replacement is frequently very different. In many cases, a lack of opposing units with TSL on those few teeth that do occlude leads to a lack of stable posterior support, which may in turn give the appearance of a decreased OVD, usually with a more cranial and forward habitual/functional position and consequent anterior TSL, sometimes termed a ‘collapsed’ occlusion.52 In many of these cases, the RCP is at an appropriate OVD but is simply unstable, and what appears to be a problem relating to lack of space to restore anterior teeth is, in fact, a problem of a lack of posterior support with space available anteriorly (Figure 19). Where RCP contacts do not exist to guide determination of OVD, and where TSL is gross and uncompensated (Figure 20), basic principles for provision of removable prostheses should be followed. In a few cases, patients may present with multiple retained teeth, but with these not being suitable for restoration, even with remedial treatment, in such cases an overdenture is often the only treatment option, even if this entails further reduction of the clinical crowns (Figure 21): where such reduction of clinical crowns would be excessive, then an overlay/onlay denture may be more appropriate.53 Such options may also be the modality of choice where economics or time constraints do not allow consideration of complex and extensive treatment plans.
Figure 19. Anterior TSL: (a) apparent lack of space for restoration of anterior teeth; (b) restoration at RCP will provide space anteriorly. (Images courtesy of Mr S Brindley.)Figure 20. Gross TSL: (a) at presentation; (b) restored with direct composite and removable partial dentures. (Images courtesy of Mr S Brindley.)Figure 21. Gross TSL with minimal coronal tooth structure: (a) functional relationship at presentation; (b) occlusal view.
Adjunctive treatments
Surgical crown lengthening may be required where conventional full-coverage indirect restorations are planned but insufficient tooth structure is present to retain a crown, but can be obtained through moving the entire attachment apparatus apically (which requires bone removal in conjunction with gingivectomy or an apically repositioned flap). Similarly, such procedures may be helpful to improve aesthetics and increase the length of incisors in an apical rather than incisal direction.54 Another technique to allow restoration of teeth with insufficient coronal tooth structure to retain a crown is to place a post-retained core. This obviously will entail elective endodontic treatment and this decision should not be made lightly, nor without thought to the subsequent functional forces that will be placed on the then-compromised tooth. It is important to note that elective endodontic treatment itself (with subsequent post-retained core crown) will not create space, but is simply to manage the problem of insufficient coronal tooth structure. In many cases where TSL is extensive to the degree that this is a considered treatment option, other methods of gaining space will also be required.
Conclusion
Where restorative treatment is needed, a pragmatic approach should be considered first and thought also be given to keeping treatment as minimal as possible and preserving tooth structure (with minimal or no tooth preparation where possible). In many cases, this may entail a need for regular maintenance/repair but with a reward of increasing the life-cycle of teeth. This idea of balancing options is also apparent in the decision as to whether or not to provide treatment at all. In some cases, early intervention may be minimal and may actually help to prevent further problems (for example canine risers as discussed above). In any event, thorough planning is key and a full clinical examination supplemented by study models is essential in each case, with a diagnostic wax-up being invaluable to guide and assist treatment. It should also be remembered that, in the vast majority of cases, particularly where TSL is advanced, no one treatment modality alone will suffice and a multi-technique approach is required.
A number of restorative methodologies have been presented but, as discussed above, in the majority of cases TSL is slowly progressing and, unless symptoms dictate immediate intervention, then many cases can be treated simply through preventive advice to stabilize the dentition and subsequent monitoring.55 In those cases where restorative intervention is required, prevention is equally important, and it is paramount that no treatment should be undertaken unless steps to stabilize the dentition are made. This should not be restricted to the pre-treatment phase but should continue throughout treatment and form part of a planned maintenance programme, for example provision of a stabilization splint post treatment.