Khan AA, Sandor GK, Dore E Canadian Consensus Practice Guidelines for Bisphosphonate Associated Osteonecrosis of the Jaw. J Rheumatol. 2008; 35:1391-1397
Khamaisi M, Regev E, Yarom N Possible association between diabetes and bisphosphonate associated osteonecrosis. J Clin Endocrinol Metab. 2007; 92
Wessel JH, Dobson TB, Zavras Al. Zolendronate, smoking and obesity are strong risk factors for osteonecrosis of the jaw: a case-control study. J Oral Maxillofac Surg. 2008; 66
Kanis JA, Johnell O, Oden A Smoking and fracture risk: a meta analysis. Osteoporosis Int. 2005; 16:155-162
Gralow JR, Biermann JS, Farooki A NCCN Task Force Report: Bone Health in Cancer Care. J Natl Compr Canc Netw. 2009; 7:S1-S32
Moghadam-Kia S, Werth VP. Prevention and treatment of systemic glucocorticosteroid side effects. Int J Dermatol. 2010; 49:239-248
McLeod NMH, Patel P, Kusanale A Bisphosphonate osteonecrosis of the jaw: a literature review of UK policies versus international policies on the management of bisphosphonate osteonecrosis of the jaw. Br J Oral Maxillofac Surg. 2011; 49:335-342
Filleul O, Crompot E, Saussez S. Bisphosphonate-induced osteonecrosis of the jaw: a review of 2,400 patient cases. J Cancer Res Clin Oncol. 2010; 136:1117-1124
Sambrook PN, Chen JS, Simpson JM Impact of adverse news media on prescriptions for osteoporosis: effect on fractures and mortality. Med J Aust. 2010; 193:154-156
Almubarak H, Jones A, Chaisuparat R Zolendronic Acid directly suppresses cell proliferation and induces apoptosis in highly tumorigenic prostate and breast cancers. J Carcinog. 2011; 10
Di Salvatore M, Orlandi A, Babala C Anti-tumour and anti-angiogenetic effects of zolendronic acid on human non-small cell lung cancer line. Cell Prolif. 2011; 44:139-146
Tepos E, Croucher Pl, Garcia-Sanz R The use of bisphosphonates in multiple myeloma: recommendations of an expert panel on behalf of the European Myeloma Network. Ann Oncol. 2009; 20:1303-1317
Arrain Y, Masud T. Recent recommendations on bisphosphonate-associated osteonecrosis of the jaw. Dent Update. 2008; 35:238-240
Sambrook P, Olver l, Goss A. Bisphosphonates and osteonecrosis of the jaw. Aus Fam Physician. 2006; 35:801-803
Almazrooa SA, Woo S. Bisphosphonate and non-bisphosphonate associated osteonecrosis of the jaw. J Am Dent Assoc. 2009; 140:864-875
Orhan K, Bayindir H, Aksoy S Numb chin syndrome as a manifestation of possible breast cancer metastasis around dental implants. J Craniofac Surg. 2011; 22:942-945
Marx RE.Chicago: Quintessence Publishing Co Inc; 2007
Kunchur R, Need A, Hughes T. Clinical investigation of C-terminal cross-linking telopeptide test in prevention and management of bisphosphonate-associated osteonecrosis of the jaws. J Oral Maxillofac Surg. 2009; 67:1167-1173
Kim RH, Lee RS, William D. Bisphosphonates induce senescence in normal human oral keratinocytes. J Dent Res. 2011; 90:810-816
Aguire Jl, Altman MK, Vanegas SM Effects of alendronate on bone healing after tooth extraction in rats. Oral Dis. 2010; 16:674-685
Wehrhan F, Stockman P, Nkenke E Differential impairment of vascularization and angiogenesis in bisphosphonate-associated osteonecrosis of the jaw-related mucoperiosteal tissue. Oral Surg Oral Med Oral Pathol Endodont. 2011; 112:216-221
Hokugo A, Christensen R, Chung EM Increased prevalence of bisphosphonate related osteonecrosis of the jaw with vitamin deficiency in rats. J Bone Miner Res. 2010; 25:1337-1349
Fedele S, Porter SR, D'Aiuto F Non-exposed variant of bisphosphonate associated osteonecrosis of the jaw: a case series. Am J Med. 2010; 123:1060-1064
Junquera L, Gallego L. Non exposed bisphosphonate-related osteonecrosis of the jaws: another clinical variant?. J Oral Maxillofac Surg. 2008; 66
Hutchinson M, O'Ryan F, Chavez V. Radiographic findings in bisphosphonate-treated patients with stage 0 disease in the absence of bone exposure. J Oral Maxillofac Surg. 2010; 68:2232-2240
Morgan G, Davies F, Gregory W Evaluating the effects of zolendronic acid (zol) on the overall survival (os) in patients (pts) with multiple myeloma (MM). Results of the Medical Research Council (MRC) Myeloma IX Study. J Clin Oncol. 2010; 28
Terpos E, Berenson J, Cook RJ Prognostic variables for survival and skeletal complications in patients with multiple myeloma osteolytic bone disease. Leukemia. 2010; 24:1043-1049
Gnant M, Harbeck N, Tomssen C. St Gallen 2011: Summary of the Consensus Discussion. Breast care. 2011; 6:136-141
Miksad RA, Lai KC, Dobson TB. Quality of life implications of bisphosphonate associated osteonecrosis of the jaw. Oncologist. 2011; 16:121-132
Black DM, Schwartz AV, Ensrud KE Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. J Am Med Assoc. 2006; 296:2927-2938
Phillips JM, Thibodeaux JD, Nathan CA Skull base osteomyelitis and bisphosphonate use in multiple myeloma: report of two cases and literature review. Laryngoscope. 2010; 120
Stopeck AT, Lipton A, Brody JJ. Denosumab compared with zolendronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol. 2010; 28:5132-5139
Fizazi K, Carducci M, Smith M. Treatment of bone metastases in men with castration-resistant prostate cancer: a randomised double-blind study. Lancet. 2011; 5:(9768)813-822
Professor of Musculoskeletal Gerontology, University of Derby and Consultant Physician, Nottingham University Hospitals NHS Trust, Hucknell Road, Nottingham, NG5 1PB, UK
Bisphosphonates are effective drugs used to treat important medical conditions affecting the skeleton, such as malignancy and osteoporosis. Bisphosphonate-associated osteonecrosis of the jaw (BONJ) is a rare but painful condition that can affect quality of life. Healthcare professionals need to be aware of this potential side-effect of bisphosphonates, as well as ways to minimize its occurrence.
Clinical Relevance: This review addresses the definitions of BONJ, differential diagnosis and staging, prevention and also discusses a recently recognized non-exposed variant of BONJ. The possibility that a recently introduced anti-resorptive agent, denosumab, which is not a bisphosphonate, may cause jaw osteonecrosis is also discussed.
Article
The bisphosphonate group of drugs are pyrophosphate analogues. They have a high affinity to bone and are taken up by osteoclasts during natural bone resorption. Bisphosphonates work by acting on osteoclast function to reduce bone resorption.1 They are important in treating many conditions such as osteoporosis, osteogenesis imperfecta, Paget's disease, skeletal events associated with metastatic cancer, hypercalcaemia, primary hyperparathyroidism and bone cancers such as Ewings Sarcoma (second most common bone cancer in young adolescents). As more research has been performed on bisphosphonates, their applications for use have increased. Consequently, general dental practitioners, dental hygienists and other healthcare workers may come across an increasing number of patients prescribed these drugs. Since bisphosphonates have been associated with osteonecrosis of the jaw (BONJ), it is essential that the management of patients on bisphosphonates is understood, the higher risk patient groups are identified and the risk of BONJ is minimized.
It is the purpose of this paper to provide an update on bisphosphonates and BONJ.
Risk factors for developing BONJ
Factors associated with an increased risk of BONJ are listed below:
Epidemiological studies on BONJ require appropriate adjustment for the fact that there is a link between osteoporosis, smoking and poor healing.6 Further work is required on the link between diabetes and BONJ; for example, whether poorer diabetic control increases the risk of developing BONJ and if there is a difference in occurrence between Type 1 and Type 2 diabetes.
In patients with prostate and breast cancer that develop metastases, 68% and 73% affect the skeleton, respectively. Widespread bony involvement is also common in multiple myeloma patients. The spread of cancer to the bones can cause pain, nerve compression, hypercalcaemia and fracture. Some cancer treatments (eg hormonal treatments for prostate cancer; hormonal and aromatase inhibitors for breast cancer) can also cause bone loss and secondary osteoporosis. Anti-resorptive agents, such as bisphosphonates, are useful in maintaining bone health in patients undergoing several cancer treatments.7
Corticosteroids (glucocorticoids) are widely used in a number of conditions including respiratory, inflammatory, auto-immune disease and skin diseases.8 A major problem associated with the use of these drugs is corticosteroid-induced osteoporosis. In those people taking significant cumulative doses of corticosteroids, bisphosphonate therapy is recommended to prevent loss of bone mineral density (BMD). The measurement of bone mineral density (BMD) is currently the standard method of diagnosing osteoporosis. Osteoporosis is confirmed if the BMD T score (standard deviation below the mean for a young adult) is less than -2.5. Osteopenia is defined as a BMD T score between -1 and -2.5. Some guidelines advocate using bisphosphonates if the T score is worse than -1 in those patients taking corticosteroids. As both corticosteroids and bisphosphonates are risk factors for developing BONJ, the implication for dentists is that, when taking medical histories, special note of the ‘steroid-bisphosphonate duo’ be made as there may be a higher risk of BONJ after trauma such as a tooth extraction.
There are currently two types of bisphosphonate:
Non nitrogen-containing or first generation drugs – clodronate, etidronate and tiludronate; and
Nitrogen-containing or newer generation bisphosphonates – pamidronate, alendronate, ibandronate, risedronate and zoledronic acid.
The non nitrogen-containing are far less effective clinically in medical treatments than the nitrogen-containing bisphosphonates. Most cases of BONJ have been associated with the nitrogen-containing bisphosphonates.9
In terms of drug potency, zolendronic acid is considered to be a very potent intravenous bisphosphonate, being able to reach higher concentrations in bone rapidly (in months) relative to oral bisphosphonates such as alendronate, which can take much longer. Filleul et al found that, on reviewing 2,400 BONJ patients between 2003 and 2009, 88% of these were associated with zoledronic acid. Furthermore, 67% of cases were following tooth extraction. The vast majority (89%) of the BONJ cases were associated with malignancy.10 The doses of bisphosphonates used in cancer patients are generally much higher than the doses used for the treatment of osteoporosis and this may be one reason why the incidence of BONJ in osteoporosis patients is very low in comparison to cancer patients.
It is important to remember the benefits of bisphosphonates in preventing osteoporosis-related fracture and the resulting morbidity and mortality in osteoporosis patients. The issue of BONJ should be discussed in a balanced manner, particularly after ‘media scares’. Nine months after a television programme was screened in Australia on BONJ, prescription rates for bisphosphonates were down by over 29,000. This, in turn, may have resulted in 70 hip fractures (which are associated with significantly reduced quality of life and much cost in monetary terms to the health and social services), 60 other fractures and 14 deaths.11
Recent in vitro research has also found that bisphosphonates may have anti-tumour effects in breast cancer and prostate cancer,12 as well as in non-small cell lung cancers.13 It is well established that bisphosphonates reduce skeletal events in multiple myeloma.14In vitro research suggests that breast cancer cells are stopped from infiltrating bone by bisphosphonates via alteration of adhesion of the malignant cells to the extracellular bone matrix.7
The definition of bisphosphonate-associated osteonecrosis of the jaw
Currently, the definition of BONJ varies, depending on geographic location in the world. In Scotland, the Scottish Dental Clinical Effectiveness Programme (SDCEP) defines BONJ as ‘exposed necrotic bone in the maxilla or mandible that has persisted for more than eight weeks in patients taking bisphosphonates and where there is no radiation therapy to the jaw’.15 This is similar to the current British Dental Association guidelines and the American Society of Bone and Mineral Research (ASBMR) definition.16
The ASBMR defines a confirmed case of BONJ as ‘an area of exposed bone in the maxillofacial region that did not heal within eight weeks after identification by a healthcare worker, in a patient who was receiving, or had been exposed to, a bisphosphonate and had not received radiation therapy to the craniofacial region’. A suspected case of BONJ, however, is ‘an area of exposed bone in the maxillofacial region that had been identified by a healthcare worker and had been present for <8 weeks in a patient who was receiving or had been exposed to a bisphosphonate and had not had radiation therapy to the craniofacial region’.17 The Australian and New Zealand Bone and Mineral Society has a similar definition, that is the patient has to have had exposure to bisphosphonates but no radiation therapy, but they define BONJ as an exposed area of bone present for more than six weeks.18
Differential diagnosis is imperative when considering BONJ. We must exclude:
Metastasis (biopsy may be necessary if suspected);
Osteomyelitis arising from dental origin – osteomyelitis is a marrow space infection;
Dental abscess (with or without chronic draining sinus);
Periodontal infection;
Alveolar osteitis (dry socket);
Sinusitis;
Temporomandibular joint disorders;
Idiopathic benign sequestration of the lingual plate of the mandible.
Idiopathic benign sequestration of the lingual plate of the mandible usually occurs in patients of the age range 32 to 57 years. It mostly involves the mylohyoid ridge, bony tori or mandibular exostosis. It has been suggested that these areas have poor blood supply, so minimal trauma can result in some ischaemia which, in turn, leads to spontaneous sequestration of mandibular bone in patients without underlying systemic disease.19
Radiographic signs of BONJ may include osteosclerosis of the lamina dura; a post-extraction radiograph may show moderate bony sclerosis or osteolysis or even inferior alveolar canal narrowing. Sometimes, differential diagnosis may be difficult but it is always important to consider the possibility of metastasis (Table 1).20
Condition
Radiographic finding
Metastasis eg breast cancer
Moth-eaten radiolucent and radio-opaque mixed appearance around teeth/implants. Clinically numb chin syndrome may occur.22
Osteomyelitis
Poorly defined radiolucent area with areas of radio-opaque sequestra.
Dental abscess with draining sinus
Radiolucency associated with the apex of the tooth-radiographically a gutta percha point placed into the chronic draining sinus will point to the abscessed tooth.
Periodontal infection
Moderate to advanced bone loss is present in periodontal disease. Bone loss around the teeth occurring at a similar rate gives an even crestal bone contour, ie horizontal bone loss. Vertical bone loss occurs when bone is lost at different rates around surfaces of tooth, resulting in angular bone loss.
There are differing opinions amongst the physicians and oral surgeons on the usefulness of blood test ‘C-Terminal Cross-Linking Telopeptide’ (CTX) in detecting early BONJ. CTX is a bone resorption and bone turnover marker and a measure of bone suppression. Marx advocates its use in predicting those at high risk of BONJ.21 Kunchur et al performed fasted morning CTX tests on 348 patients. Amongst the group there were 222 patients that were referred for extractions, as they were deemed at high risk of BONJ; 113 were controls and 15 had BONJ. They found the CTX did not predict which patients taking bisphosphonates will develop BONJ but did pick up those at higher risk.22 Different bisphosphonates suppress CTX to different degrees (with zoledronic acid showing the greatest suppression). More research is needed on improving the identification of those individuals taking bisphosphonates at high risk of BONJ. CTX or other bone turnover markers may have potential but at present there is not enough data to produce evidence-based guidelines. Further cellular and genetic research may also help to improve identification of high risk individuals.
Aetiology of BONJ
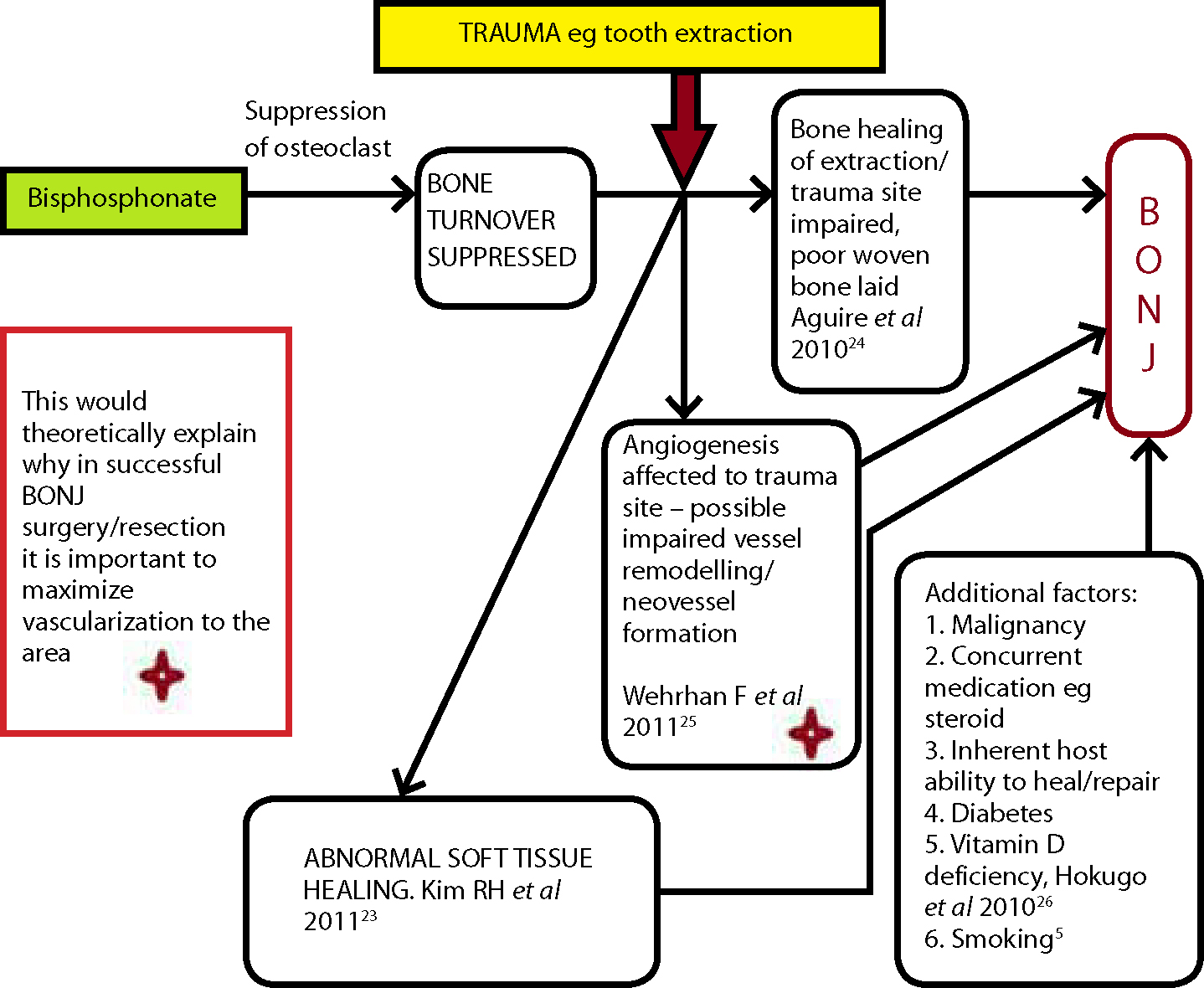
There have been various theories put forward to explain why BONJ occurs. Recent in vitro studies suggest that bisphosphonates can cause ageing of keratocytes and result in defective re-epithelialization inside the mouth.23 This could contribute to poor healing associated with BONJ. The bone turnover suppressing effects of bisphosphonates are likely to be relevant in the pathogenesis of BONJ. In this situation, trauma such as a tooth extraction could result in poorer healing due to the fact that the resulting laid bone is of poor quality.24 Furthermore, as bisphosphonates are known to affect angiogenesis, poorer blood supply and ischaemic conditions may contribute to the development of necrosis (Figure 1).
Figure 1. Hypothesis for pathogenesis of BONJ.
Non-exposed variant of BONJ
There have been recent reports of BONJ not showing the classical definition of BONJ (6 to 8 week time frame of bone exposure). Indeed, there have been cases where the bony exposure has taken over 4 months to occur from the time of trauma. Fedele et al used data from five European centres accepting referrals associated with jaw abnormalities in patients taking, or having had exposure to, bisphosphonates. They found that, of 332 patients, 96 presented with a non-exposed variant of BONJ.27 Junquera and Gallego also documented occurrence of the non-exposed variant of BONJ.28
The American Association of Oral and Maxillofacial Surgeons have refined their staging of BONJ to include the non-exposed variant of BONJ – Stage 02 (Table 2).
BONJ stage
Treatment
Stage 0: (non-exposed variant of BONJ)No exposed necrotic bone but non-specific clinical findings and symptoms currently include:Definitely no bone exposure, possible bone enlargement, possible gingival swelling, possible tooth mobility, sometimes a sinus tract, possible dull jaw pain (may radiate to temporomandibular joint area); usually but not always radiographic signs of BONJ: eg osteosclerosis of the lamina dura; moderate bony sclerosis or osteolysis on a post extraction radiograph, inferior alveolar canal narrowing; possible altered neurosensory functions; sometimes maxillary sinus pain with possible thickening and inflammation of sinus wall.
Conservative management, symptomatic treatment, eg medication for chronic pain and Abs to control infection if indicated Pt education.
Stage 1: Exposed and necrotic bone where Pt is asymptomatic and has no evidence of infection.
0.12% chlorhexidine gluconate MW, no surgical treatment needed other than removal of any necrotic bone/sequestrum without exposure of uninvolved bone. Any symptomatic teeth within exposed necrotic bone should be extracted - it is unlikely that this will increase risk of further necrosis.Review with physician/oncologist regarding continued use/regime alteration of bisphosphonate if Pt's physical condition allows.
Stage 2: Exposed and necrotic bone in Pts with pain and clinical evidence of infection (shown by erythema around the necrotic bone +/- pus discharge).
0.12% chlorhexidine gluconate MW and Abs (microbial cultures should be analysed, eg where Actinomyces appropriate Abs given), pain control, debridement superficially to help reduce soft tissue irritation. Remove as needed any necrotic bone/sequestrum without exposure of uninvolved bone. Any symptomatic teeth within exposed necrotic bone should be extracted - it is unlikely that this will increase risk of further necrosis.Review with physician/oncologist regarding continued use/regime alteration of bisphosphonate if Pt's physical condition allows.
Stage 3: Exposed and necrotic bone in patients showing pain, infection as well as one of the following: necrotic exposed bone extending beyond the area of alveolar bone (that is the maxillary sinus and zygoma in the maxilla and the inferior border and the ramus in the mandible) resulting in pathological fracture, oro-antral fistula, oro-nasal communication, extra-oral fistula or osteolysis extending to the inferior border of the mandible or the sinus floor.
0.12% chlorhexidine gluconate MW and Abs pain control, debridement/resection, offer long-term palliative care, aim to deal with acute infection and pain. Any symptomatic teeth within exposed necrotic bone should be extracted - it is unlikely that this will increase risk of further necrosis.Review with physician/oncologist regarding continued use/regime alteration of bisphosphonate if Pt's physical condition allows.
Hutchinson et al studied 8,572 patients taking oral bisphosphonates; 1,005 had dental symptoms or complications. Those without BONJ but clinical symptoms without exposure of necrotic bone numbered 30. These patients were examined and panoramic radiography or computed tomography performed. Osteosclerosis was found in a third of those with stage 0 (ie clinical signs and symptoms but no exposed bone).29 Further larger scale collaborated research is needed in this area to find out if osteosclerosis is a significant factor in non-exposed variant cases of BONJ, or even an indicator of progression of BONJ.
The signs and symptoms of the non-exposed variant of BONJ (Stage 0) are listed in Table 2.
Where there is purulent discharge, culture of pus can be carried out and appropriate antimicrobial agents given.
It must be remembered that any alteration of bisphosphonate regime must be discussed with, and co-ordinated with, the patient's physician and medical team. The half-life of bisphosphonates is long and entombed bisphosphonate within bone may be gradually released over many years (half-life of different bisphosphonates varies). Any drug holidays should only be carried out if the patient's physical condition allows. In cases of multiple myeloma/breast cancer patients, the use of IV bisphosphonates reduces skeletal related events, ie they not only help reduce otherwise extreme pain due to spinal cord compression, hypercalcaemia or pathological fracture, they also reduce the need for bone surgery or bone radiation therapy. Bisphosphonates have shown, as discussed earlier, anti-tumour properties and helped in clinical trials involving multiple myeloma patients with bone involvement.30,31 Whilst bisphosphonates are used in advanced breast cancer with spinal metastasis, they are not currently recommended for early breast cancer.32 It has been suggested that, if the patient's systemic condition allows, discontinuation of IV bisphosphonates may help stabilize established BONJ sites and reduce the appearance of new BONJ sites;2 where the patient's quality of life is affected, in consultation with the patient and oncologist, this may be of benefit. Quality of life is significantly affected by patients suffering with BONJ, including:
The issue of drug holidays is one where the evidence base is lacking and further research is needed. Discontinuation of oral bisphosphonates for 6 to 12 months may result in spontaneous sequestration or resolution after debridement. It is important to liaise with the treating physician. It is essential to consider the patient's systemic condition when altering the regime or discontinuation of bisphosphonates in cases of BONJ.2
Prevention of BONJ
Patients taking oral bisphosphonates
Patients taking oral bisphosphonates for more than three years (cumulative dose) may be at risk of BONJ, especially those patients also taking long-term steroids. However, stopping oral bisphosphonates after many years of continual use may be associated with a higher risk of fracture and bone loss.34
The AAOMS2 suggest, after consultation with the patient's physician, stopping the oral bisphosphonate three months prior to any invasive, elective dental surgery (eg implants) and three months after. This advice, however, is not evidence-based but a pragmatic attempt at expert opinion.
Patients taking IV bisphosphonates
It is important in these patients to reduce the risks of developing BONJ occurring. This is especially the case in patients being treated for malignancy. If the patient's physical condition allows, we should try and get the patient dentally fit. This would include:
Removing teeth of hopeless prognosis;
Restoring decayed teeth;
Carrying out any needed root treatment;
Dealing with any acute periodontal disease;
Scaling to remove plaque-retaining calculus;
Ensuring dentures fit adequately and are not causing mucosal trauma (advise patients to leave dentures out at night to reduce trauma risks);
Check flange extensions, especially lingually where the mucosa is thin at the floor of the mouth.
Homecare is important and patients should be advised to return if they notice any swelling or anything abnormal in the oro-facial region.2 Recently, there have been reported cases of patients (in remission and not immune compromised) with multiple myeloma using IV bisphosphonates, where there have been bone masses in the temporal and maxillary area associated with skull base osteomyelitis. Pathological analysis revealed no metastasis but instead Actinomyces associated with osteonecrosis. In such cases, early consideration of the differential diagnosis and appropriate treatment is mandatory in order to stop intracranial complications.35
Other bone anti-resorptive agents
Bisphosphonates are classed as bone modifiers as they alter bone structure. There are now other bone modifiers, eg denosumab. This is a monoclonal antibody which acts on the RANK ligand system, inhibiting osteoclastic resorption of bone. A randomized double blind study found that, when denosumab was compared to zolendronic acid in the treatment of breast cancer metastases, it was better in reducing skeletal-related events.36 The patient survival, disease progression and adverse events (including osteonecrosis of the jaw) were similar in both groups of patients. Osteonecrosis of the jaw was a rare event (2% with denosumab and 1.4% with zolendronic acid; P = 0.39). In another recent study, which examined advanced prostate cancer,37 denosumab showed better results compared to zoledronic acid in reducing skeletal related events. Osteonecrosis of the jaw in this study of 1904 patients occurred infrequently (2% in denosumab group and 1% in zoledronic acid group – a non-significant difference). The incidence of osteonecrosis of the jaw in osteoporosis patients taking denosumab is not known, but as with bisphosphonate-taking osteoporosis patients, is likely to be much lower than with the cancer patients.
Conclusion
Bone-modifying agents are constantly being developed and their umbrella of use increasingly expanding. One type of these agents, the bisphosphonates, are essential to prevent fractures and the morbidity and potentially crippling effects of osteoporosis, as well as to help those patients suffering with pain due to skeletal-related events in malignancy. BONJ is a rare but important complication of bisphosphonates and potentially of other newer anti-resorptive agents, which reduces quality of life. Knowledge on risk factors and aetiology of BONJ is rapidly expanding and guidelines for prevention and treatment of this condition are developing as more studies are published.