This paper outlines the features and presentation of body dysmorphic disorder (BDD), a psychological syndrome which results in patients seeking treatment for an imagined defect in appearance. The assessment of patients with suspected body dysmorphic disorder is outlined, as well as management strategies.
Clinical Relevance: Clinicians working in the field of aesthetic dentistry should be aware that some patients presenting for treatment may have body dysmorphic disorder. Aesthetic dental treatment for such patients is not beneficial and carries some risks. Advice for clinicians on assessment and management is outlined.
Article
Requests for aesthetic dental treatment and the availability of such treatment options are increasing as expectations of the appearance of teeth change. Clinicians are rightly concerned about the patient who appears to be overly preoccupied and distressed by minor (or non-existent) defects; such patients may be suffering from a psychological disorder called body dysmorphic disorder (previously termed dysmorphophobia). This paper outlines the features of body dysmorphic disorder (BDD), and describes techniques for assessment and management.
Body dysmorphic disorder: an overview
The diagnostic criteria for BDD are outlined in the Diagnostic and Statistical Manual of Diseases, version 4.0.1 The criteria are:
Preoccupation with an imagined defect in appearance. If a slight physical anomaly is present, the person's concern is markedly excessive in relation to the nature of the defect.
The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
The preoccupation is not better accounted for by another mental disorder (eg anorexia nervosa).
The primary symptom of BDD is preoccupation with perceived defects. Concerns may be specific to particular body parts or a more pervasive vague concern about something ‘not being right’. The feature is felt to be unbearably ugly, leading to high levels of shame and distress2 and low levels of self-esteem.3 Individuals with BDD are convinced of the severity of the defect, no matter how minor it may seem to others.4 Aspects of appearance most commonly the focus of this preoccupation are the skin (eg blemishes and moles), hair and nose, thus the face is frequently involved. There is some suggestion of differences according to gender, men being more likely to be preoccupied with their genitals, height, hair and body build, while for women the focus is likely to be their weight, hips, legs and breasts.5 However, the focus often shifts between body parts over the course of the disorder. Individuals with BDD have thoughts and concerns about the body part (eg everyone is staring at it; this body part is ‘disgusting’) which are experienced as uncontrollable and intrusive. These thoughts are likely to be worse in social situations. Up to 77% of people with BDD could be said to be delusional in their beliefs at some point in their disorder.5
The usual age of onset of symptoms is late adolescence (the average age reported in a large sample of patients was 16.4 years). However, people with BDD can go undiagnosed for many years and the typical age of presentation of psychiatric services is in the early 30s.5 The disorder is equally common amongst men and women.6 BDD is commonly misdiagnosed, and this may relate to the finding that people with BDD are often reluctant to disclose their symptoms and psychological distress.
The course of the illness is continuous, that is it is unusual for symptoms to show periods of remission. Complete remission is rare and its occurrence is related to the duration and severity of symptoms, such that people who have relatively mild BDD, which is not long established, are most likely to remit.7 Comorbidity is frequent in individuals with BDD: the condition is commonly associated with the presence of other psychiatric disorders, such as depression, anxiety, social phobia and obsessive compulsive disorder. For example, approximately 38% of people with BDD have previously experienced a social phobia. Alcohol dependence is also common, as individuals may attempt to manage their distress by using alcohol. Of great importance for clinicians who may treat individuals with BDD, suicidal ideation (considering suicide or making plans to commit suicide) is common, being reported in 78% of cases, and 17 to 33% of cases have attempted suicide.8 This is a critically important point in the assessment of individuals with BDD. BDD may be prodromal of schizophrenia in late adolescence and early adulthood.
The individual with BDD may engage in a variety of compulsive behaviours in relation to his/her body part.9 These behaviours are termed ‘compulsive’ because they occur at very high rates and are repetitive. Examples include:
Checking the body part in the mirror;
Comparing the self to others;
‘Skin picking’ (seeking to remove the blemish by plucking it or scratching it);
Applying make up; and
Camouflaging the body part with clothes.
These rituals, while reducing anxiety in the short term, are counter-productive in terms of reducing anxiety in the longer term, as they tend to lead to increased focusing of the perceived problem and anxiety rather than reassurance. The rituals may occupy a number of hours each day, leading to impairment in ability to function in work or relationships. For instance, 27% of people with BDD report having been housebound at some point in the disorder.6 This should be differentiated from a diagnosis of agoraphobia; individuals with BDD are housebound as a secondary consequence of their anxiety from their perception that people will stare at them, judge them and so on.
Individuals with BDD often believe cosmetic treatment is the only way to deal with the defect and, in turn, seek help from clinicians such as maxillofacial surgeons, dermatologists and plastic surgeons. A number of surveys of individuals with BDD have indicated that 71–76% had sought cosmetic treatment, and approximately 65% of all cases had received cosmetic treatment. The treatments most commonly undergone were rhinoplasty, liposuction, breast augmentation, though minimally invasive procedures were also common (collagen injections, tooth whitening). Refusal of treatments is less common than might be expected; only 35% of treatments requested by people with BDD were refused.10
Prevalence
In community samples, the estimated prevalence of individuals varies from 0.7–3%. Estimates amongst young student samples range from 2.2–28%. The reason for such large variation is probably the criteria used to define a ‘case’. Where strict psychiatric criteria are adopted, the estimated prevalence tends to be lower. It would be anticipated that, in populations seeking cosmetic or aesthetic dental care, the prevalence of BDD should be higher. Although, the research on BDD and dental treatment is relatively sparse, various published case reports document patients with BDD attending for treatment in general dentistry11,12 and maxillofacial surgery.13,14 Hepburn and Cunningham15 conducted a survey of 40 patients attending for adult orthodontic treatment and found an estimated prevalence of 7.5% for BDD, suggesting that individuals with BDD are likely to seek orthodontic treatment. This is supported by a recent investigation of patients presenting to two maxillofacial surgery outpatient clinics, where 10% of patients were found to demonstrate symptoms of BDD.16 De Jongh and co-workers17 surveyed a community sample about their intentions to receive cosmetic dental treatment and found that those who reported being preoccupied with a defect of appearance were nine times more likely to consider tooth whitening and six times more likely to consider orthodontic treatment, compared to those without such a preoccupation. It follows that clinicians working in the field of aesthetic dentistry are likely to be visited by patients with BDD and, as such, need to be aware of this condition and how to assess and manage patients suspected of having BDD.
Assessment of patients who are suspected of having BDD
Cunningham and Feinman18 outline the importance of systematic and detailed assessment of individuals who are suspected to have BDD attending for dental treatment. The first consideration is to ensure that the setting is conducive to disclosure and discussion of the underlying problem; this includes allowing sufficient time to discuss the individual case, minimizing the number of people present (while ensuring that a chaperone is present) and ensuring privacy from interruptions. The patient will also need to be reassured that the information they give will remain confidential within their healthcare team.
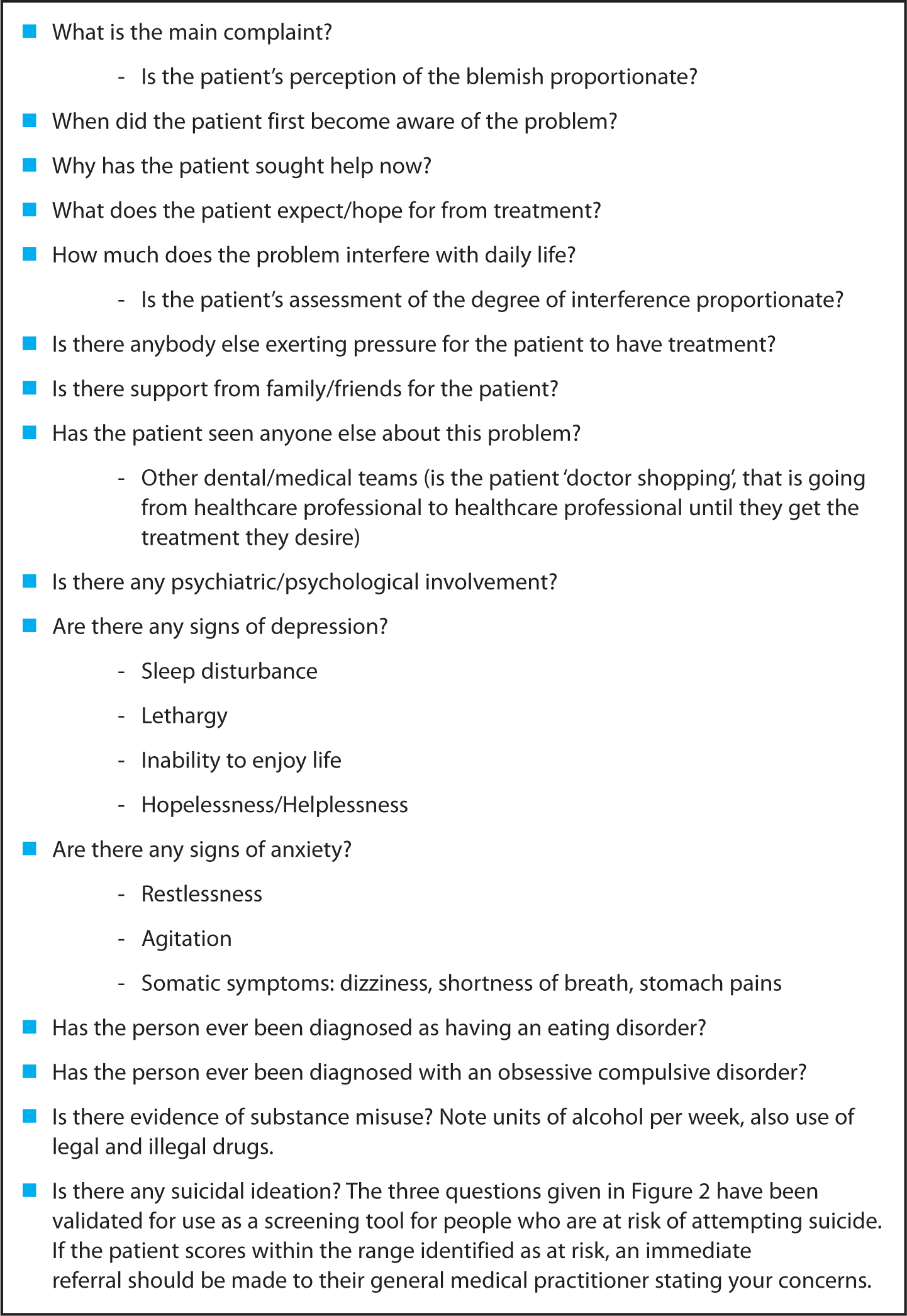
Having established a ‘safe’ environment for the patient to talk with the dentist, and sufficient rapport to ensure open communication, there are a number of areas which the discussion should cover (Figure 1). Central to this is an assessment of whether the patient's response is proportionate. Is it reasonable to hold such strong beliefs about the defect, be it imagined or real? Are the consequences of having such a defect proportional to the reported interference of the defect? For example, being unable to maintain employment because of crooked teeth is unlikely to be a realistic consequence.
Figure 1. Areas to cover in an interview with a patient who is suspected to have BDD.18
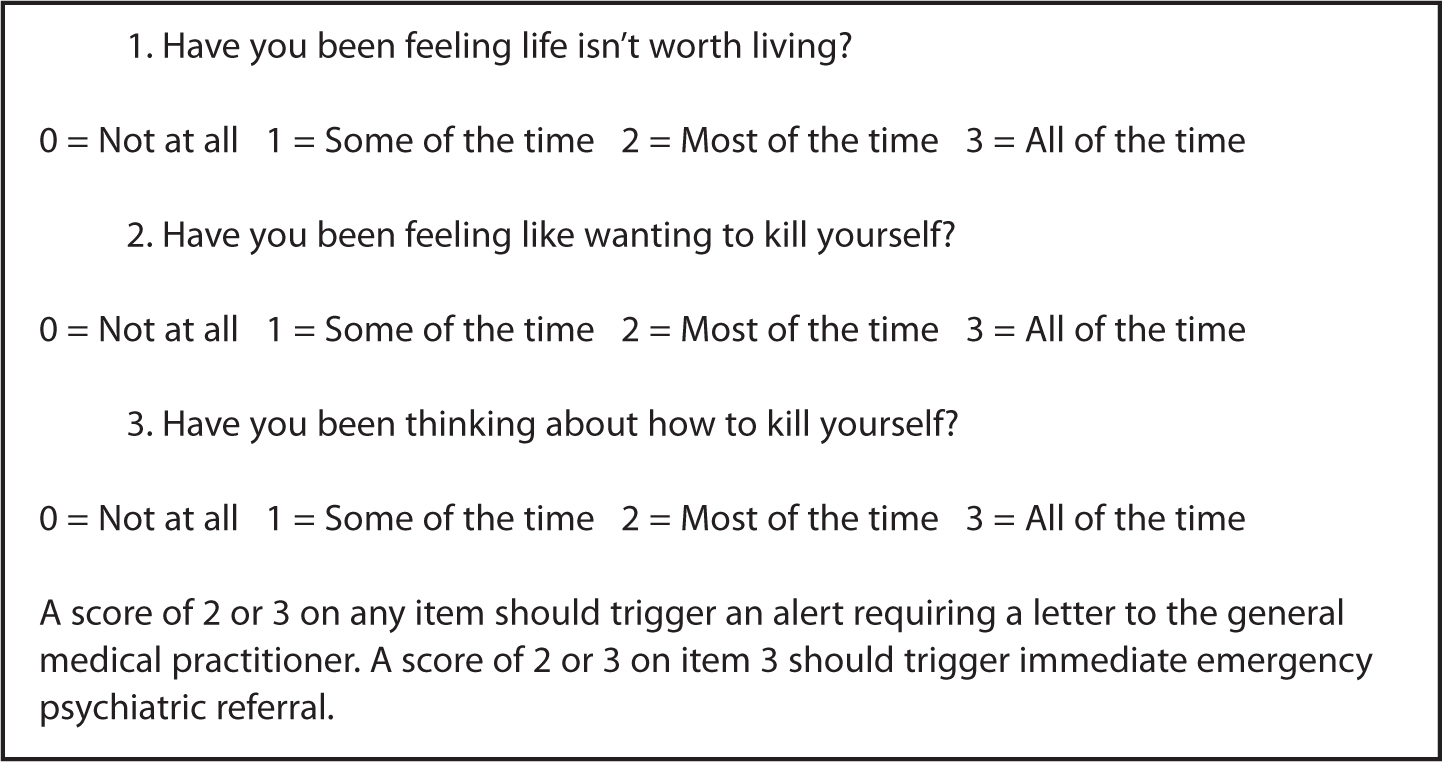
If the clinician has strong suspicions of a diagnosis of BDD, or where there is clear suicidal ideation, the patient should be referred for formal assessment by psychological or psychiatric services. Any referral letter should contain reference to the information gained from the interview in Figures 1 and 2.
Figure 2. Assessing suicide risk.19
Management strategies for people with BDD
Provision of the requested cosmetic treatment
Once a formal diagnosis of BDD has been made, it is not advisable to commence with cosmetic treatment. Provision of the requested cosmetic treatment appears to be of little benefit to the patient and there is some possible harm. Crerand et al found that 91% of procedures administered to people with BDD resulted in no change in BDD symptoms.10 Further, there is strong suggestion that people with BDD express high levels of dissatisfaction with treatment.20 This often leads to further treatment (usually with different clinicians) or the shifting of the preoccupation to another part of the body.2
Additionally, there are numerous possible adverse effects for the treating clinician if he/she provides cosmetic treatments for people with BDD. As patients tend to be dissatisfied with the results of cosmetic treatment, there is the possibility that the patient may sue the clinician for his/her perceived poor outcome (29% of members of the American Society for Aesthetic Plastic Surgery have been sued at some point in their medical career, though it is not possible to determine how many of these cases involved a person with BDD).21 In a court case of an individual who sued their clinician for treating them without their consent (Lynn G vs Hugo), the patient argued that, since they had been diagnosed with BDD they were unable to consent for treatment properly. Although the case was not upheld (on the grounds that there was no evidence that the patient had BDD at the time that they gave consent for the treatment – they were only diagnosed after the treatment had taken place), there is an interesting precedent here that treating an individual who is known to have BDD may mean that any consent given by the patient is not valid. Furthermore, serious risks include physical assault (2% of physicians who are members of the American Society for Aesthetic Plastic Surgery have been attacked by patients; 10% have been threatened).21 There are two known cases where a clinician has been murdered by an individual with BDD who they had treated.22
Thus, given the potential risks to both the patient and the professional, it is recommended that patients diagnosed with BDD should not undergo the cosmetic treatment requested. Instead, in a sensitive yet straightforward manner, clinicians should discuss with the patient that the cosmetic treatment is not in the patient's best interest4 and recommend referral to psychological or psychiatric services for pharmacological or psychological treatment.
Pharmacological and psychological therapy
A recent Cochrane review23 suggested that both pharmacotherapy and psychotherapy may be effective in the treatment of BDD.
Psychological management of BDD, specifically cognitive behavioural therapy (CBT) is recommended as the first line of management by the National Institute for Health and Clinical Excellence (NICE, http://www.nice.org.uk/Guidance/CG31). CBT is based on the premise that the emotions, such as anxiety and distress, are affected by thoughts (or ‘cognitions’) and beliefs, and by behaviour. CBT works by encouraging the reassessment of thoughts and actions. CBT often includes exposure to the feared stimulus (eg social setting) and response prevention whereby the patient is encouraged to face his/her anxiety without engaging in repetitive ritual. This process is repeated until the patient no longer feels anxious. CBT can also involve changing beliefs connected to patients' dissatisfaction with their body, teaching stress management techniques and provision of information about the condition.23 Randomized controlled trials have indicated that, for example, reports that 55% of patients in a CBT group improve, in comparison, none of the no treatment control group improved and 14% were symptomatically worse.24
There is good evidence for the effectiveness of anti-depressive drugs in people with BDD. Randomized controlled trials of selective serotonin reuptake inhibitors (eg fluoxetine. clomipramine) indicate that, on average, 53% of individuals with BDD improved compared to 18% in the placebo control group.25 Given the prevalence of delusions amongst people with BDD, it has been suggested that anti-psychotic agents might be prescribed. However, there is no evidence for the effectiveness of anti-psychotic agents in patients with BDD, even when delusions are present.
Conclusions
Patients with BDD are likely to present for aesthetic or cosmetic dental treatment. This is potentially problematic since aesthetic dental treatment has little benefit for people with BDD and has potentially negative consequences for patient and the treating clinician. Clinicians should be aware of this possibility and be familiar with specific strategies to recognize and assess people with suspected BDD and appropriately manage them by referral to specialist services.