Article


Conventional oral exploration (visual and palpation examination) constitutes the current gold standard for oral cancer screening, while biopsy and histopathological examination are indispensable for case detection. There are also a number of other techniques, that may contribute to the diagnosis of oral cancer, discussed below.
Biopsy and histopathology
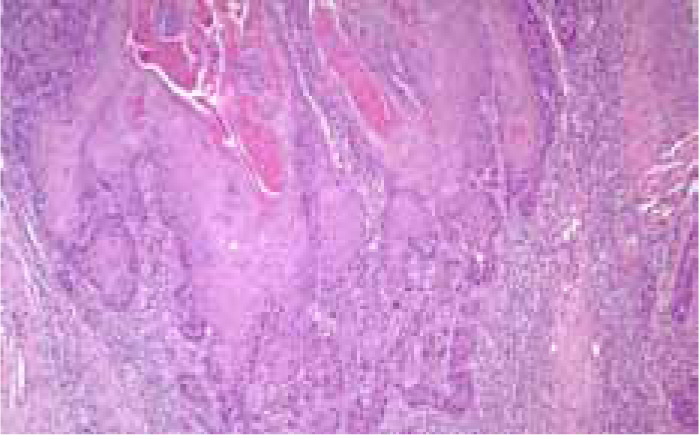
The accurate diagnosis of potentially malignant and malignant oral lesions depends on the quality of the biopsy, adequate clinical information, and correct interpretation of biopsy results (Figure 1).
Oral biopsy is discussed in Article 5. Specimens can be affected by crushing, fulguration, injection, or incorrect fixation and freezing. There is controversy regarding incisional versus excisional biopsy and surrounding the use of the most appropriate surgical instruments. Excisional biopsy is theoretically preferable because it allows histopathological examination of the entire lesion, but it risks incomplete treatment of malignant lesions and overtreatment of benign ones. It has been suggested that neck metastasis from OSCC may increase after incisional biopsy because tumour cells appear in the peripheral blood 15 minutes after incisional biopsies using a conventional scalpel. Other means of obtaining biopsy material might minimize seeding of cells. Electrocautery or CO2 laser, however, can produce thermal cytological artefacts.
Toluidine blue staining (see below) is best for selecting the site(s) for biopsy in large lesions and multiple biopsies and reducing the percentage of underdiagnoses.
Imaging techniques (DPT, CT, MRI) are also often used to supplement the clinical evaluation and tumour staging. CT is the technique of choice to evaluate bone invasion. Cone beam CT (CBCT) helps determine the invasion and extension of a lesion towards jaw bones, with the added advantages of lower cost and a lower radiation dose than conventional CT. MRI is more informative when evaluating soft tissue invasion, neurovascular infiltration, or cervical lymph node involvement.
Staging
Quality management of cancer requires universal, accurate TNM (Tumour; Node; Metastasis) staging, which must be documented in the clinical notes and on the database (Tables 1–3).
| TX | Primary tumour cannot be assessed. |
| T0 | No evidence of primary tumour. |
| Tis | Carcinoma in situ. |
| T1 | Tumour 2cm or less in greatest dimension. |
| T2 | Tumour more than 2cm but not more than 4cm in greatest dimension. |
| T3 | Tumour more than 4cm in greatest dimension. |
| T4 | Lip : Tumour invades adjacent structures, eg through cortical bone, inferior alveolar nerve, floor of mouth, skin of face. |
| NX | Regional lymph nodes cannot be assessed. |
| N0 | No regional lymph node metastasis. |
| N1 | Metastasis in a single ipsilateral lymph node, 3cm or less in greatest dimension. |
| N2 | N2a Metastasis in a single ipsilateral lymph node, more than 3cm but not more than 6cm in greatest dimension. |
| N3 | Metastasis in a lymph node more than 6cm in greatest dimension. |
| Nomenclature of anatomical site of lymph node | |
| Level I | Contains the submental and submandibular triangles bounded by the posterior belly of the digastric muscle, the hyoid bone inferiorly and the body of the mandible superiorly. |
| Level II | Contains the upper jugular lymph nodes and extends from the level of the hyoid bone inferiorly to the skull base superiorly. |
| Level III | Contains the middle jugular lymph nodes from the hyoid bone superiorly to the cricothyroid membrane inferiorly. |
| Level IV | Contains the lower jugular lymph nodes from the cricothyroid membrane superiorly to the clavicle inferiorly. |
| Level V | Contains the posterior triangle lymph nodes bounded by the anterior border of the trapezius posteriorly, the posterior border of the sternocleidomastoid muscle anteriorly and the clavicle inferiorly. |
| Level VI | Contains the anterior compartment lymph nodes from the hyoid bone superiorly to the suprasternal notch inferiorly. On each side the lateral border is formed by the medial border of the carotid sheath. |
| Level VII | Contains the lymph nodes inferior to the suprasternal notch in the upper mediastinum. |
| MX | Distant metastasis cannot be assessed. |
| M0 | No distant metastasis. |
| M1 | Distant metastases. |
Clinical palpation of the cervical lymph nodes is generally regarded as inaccurate (sensitivity and specificity 60–70%), and micrometastases may be present. CT has a higher sensitivity in detecting metastatic disease (69–93%) than physical examination. MRI is even better than CT but less readily available. Ultrasound Guided Fine Needle Aspiration Cytology (US-guided FNAC) requires particular expertise and experience, but can have a sensitivity of 76% and a specificity of 100%. PET/CT scanning is currently under evaluation.
Metastases may be further specified according to site (Table 4).
| Pulmonary | PUL | Bone marrow | MAR |
| Osseous | OSS | Pleura | PLE |
| Hepatic | HEP | Peritoneum | PER |
| Brain | BRA | Adrenals | ADR |
| Lymph nodes | LYM | Skin | SKI |
| Others | OTH |
Careful examination of the upper aerodigestive tract is mandatory and can identify primary tumours in 40–50% of patients presenting with a metastatic cervical lymph node but no other symptoms. Panendoscopy should include the oral cavity, pharynx, larynx, and upper oesophagus. Chest radiology should be performed to look for metastases and any second primary tumours (SPTs). CT or MRI scan of the chest should be carried out in suspected metastases.
The absence or presence of residual tumour after treatment may be described by the symbol ‘R’ (Table 5).
| RX | Presence of residual tumour cannot be assessed. |
| R0 | No residual tumour. |
| R1 | Microscopic residual tumour. |
| R2 | Macroscopic residual tumour. |
Additional diagnostic aids
A number of possible diagnostic aids have appeared on the market but as yet none has been accompanied by scientific studies that has convinced the clinical community of their usefulness over and above clinical examination (Table 6).
|
|
Toluidine blue (TB)
Toluidine blue (tolonium chloride) (Figure 2) has been evaluated as a diagnostic aid in many studies over many decades. A meta-analysis based on data available up to 1989, assessing the effectiveness of TB, revealed a sensitivity for identifying oral squamous cell carcinomas between 93% and 97% and a specificity between 73% and 92%. However, many of these studies had serious methodological flaws.

Light-based detection systems
Light-based detection systems were introduced on the assumption that the mucosal structural and metabolic changes during carcinogenesis give rise to distinct profiles of absorption and refraction when exposed to different types of light or energy (Table 6). Sadly, few reliable studies have appeared before their release for clinical use.
Chemiluminescence
ViziLite® (Zila Pharmaceuticals, Phoenix, Arizona, USA) is the best known system. It appears to have a high sensitivity (100%), but its specificity (0%–14.2%) and positive predictive value are low. ViziLite® does not help overall in the identification of malignant and premalignant oral lesions and therefore the combination with TB (ViziLite Plus®) was proposed to reduce the number of false positives. Although the specificity and positive predictive value of this combination have improved, there is little supporting scientific evidence.
Microlux/DL® consists of a battery-powered, light-emitting diode (LED) transilluminator with an autoclavable light guide that produces diffused light (Microlux/DL®, AdDent Inc, Danbury, Connecticut, USA). In a prospective study, the sensitivity and specificity for the detection of oral cancerous and precancerous lesions were 77% and 70%, respectively.
Tissue fluorescence imaging
VELscope® (Visually Enhanced Lesion Scope; LED Dental Inc, White Rock, British Columbia, Canada) detects the loss of fluorescence in visible and non-visible high-risk oral lesions, such as cancers and precancers, by applying direct fluorescence. Reported sensitivity values of 97% to 100% and specificities of 94% to 100% are encouraging but there are no studies that have demonstrated the utility as a diagnostic aid in lesions in low-risk patients or when used by general dentists.
Tissue fluorescence spectroscopy
Autofluorescence spectroscopy consists of a small optical fibre that produces various excitation wavelengths and a spectrograph that receives the data and records it on a computer. This eliminates the subjective interpretation of the changes in tissue fluorescence resulting in a high sensitivity and specificity in differentiating healthy mucosa from malignant oral lesions.
Exfoliative cytology
OralCDx® brush biopsy (OralCDx® Laboratories Inc, Suffern, New York, USA) is a transepithelial ‘biopsy’ system. The sensitivity of this system for the detection of abnormal cells has been of 52–100% and specificity of 29–100%.
Most clinicians, faced with a doubtful mucosal lesion, will elect to undertake a biopsy with scalpel or punch, rather than undertake a procedure which is costly and is not as reliable at excluding neoplasia.