Mack F, Mundt T, Mojon P, Kocher T, Schwahn C, Bernhardt O. Parodontalstatus bei älteren Männern und Frauen. Dtsch Zahnärztl Z. 2005; 60:403-409
Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999; 4:1-6
Yoneyama T, Okamoto H, Lindhe J, Socransky SS, Haffajee AD. Probing depth, attachment loss and gingival recession. Findings from a clinical examination in Ushiku, Japan. J Clin Periodontol. 1988; 15:581-591
Toffenetti F, Vanini L, Tammaro S. Gingival recessions and noncarious cervical lesions: a soft and hard tissue challenge. J Esthet Dent. 1998; 10:208-220
Hand JS, Hunt RH, Reinhardt JW. The prevalence and treatment implications of cervical abrasion in the elderly. Gerodontics. 1986; 5:167-170
Lührs AK, Geurtsen W, Guhr S, Günay H. Gingiva-shaded compomers: clinical results after 24 months. Clin Oral Invest. 2009; 13:95-96
Zalkind M, Hochman N. Alternative method of conservative esthetic treatment for gingival recession. J Prosthet Dent. 1997; 77:561-563
Capa N. An alternative treatment approach to gingival recession: gingiva-colored partial porcelain veneers: a clinical report. J Prosthet Dent. 2007; 98:82-84
Greene PR. The flexible gingival mask: an aesthetic solution in periodontal practice. Br Dent J. 1998; 184:536-540
Miller PD. A classification of marginal tissue regeneration. Int J Periodontics Restor Dent. 1985; 5:9-13
Lührs AK, Guhr S, Schilke R, Borchers L, Geurtsen W, Günay H. Shear bond strength of self-etch adhesives to enamel with additional phosphoric acid etching. Oper Dent. 2008; 33:155-162
Frankenberger R, Lohbauer U, Roggendorf MJ, Naumann M, Taschner M. Selective enamel etching reconsidered: better than etch-and-rinse and self-etch?. J Adhes Dent. 2008; 10:339-344
Güler AU, Yilmaz F, Yenisey M, Güler E, Ural C. Effect of acid etching time and a self-etching adhesive on the shear bond strength of composite resin to porcelain. J Adhes Dent. 2006; 8:21-25
Durmusoglu Ö, Caliskan Yanikoglu F Sevikal Sert Doku Kayiplarinin CompNatur ile Restorasyonu. Dentalife. 2006; 4:26-28
Serino G, Wennstrom JL, Lindhe J, Eneroth L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J Clin Periodontol. 1994; 21:57-63
Shay K. Root caries in the older patient: significance, prevention, and treatment. Dent Clin North Am. 1997; 41:763-793
Schiffner U, Micheelis W, Reich E. Erosionen und keilförmige Zahnhalsdefekte bei deutschen Erwachsenen und Senioren. Dtsch Zahnärztl Z. 2002; 57:102-107
Günay H, Fricke R, Triadan H. Approximale Wurzeldentinkaries – eine zweite Karieswelle?. Dtsch Zahnärztl Z. 1987; 42:904-908
Lussi A, Maurer R, Zaugg D, Hotz P, Schaffner M. Prävalenz und Risikofaktoren der Wurzelkaries. Schweiz Monatsschr Zahnmed. 2001; 4:423-432
Schiffner U. Krankheits-und Versorgungsprävalenzen bei Erwachsenen (35–44 Jahre): Zahnkaries. In: Micheelis W, Schiffner U (eds). Köln: Deutscher Zahnärzte Verlag; 2006
Schiffner U. Krankheits-und Versorgungsprävalenzen bei Senioren (65–74 Jahre): Zahnkaries. In: Micheelis W, Schiffner U (eds). Köln: Deutscher Zahnärzte Verlag; 2006
Hahn P, Reinhardt D, Schaller HG, Hellwig E. Root lesions in a group of 50–60 year-old Germans related to clinical and social factors. Clin Oral Invest. 1999; 3:168-174
Kwong SM, Cheung GS, Kei LH Micro-tensile bond strengths to sclerotic dentin using a self-etching and a total-etching technique. Dent Mater. 2002; 18:359-369
Brackett WW, Brackett MG, Dib A, Franco G, Estudillo H. Eighteen-month clinical performance of a self-etching primer in unprepared class V resin restorations. Oper Dent. 2005; 30:424-429
Wiegand A, Schmid M, Schmidlin PR. Ästhetische Kronenrandkorrektur mit Komposit. Ein Fallbericht. Schweiz Monatsschr Zahnmed. 2008; 118:427-435
Kumbuloglu O, User A, Toksavul S, Vallittu PK. Intra-oral adhesive systems for ceramic repairs: a comparison. Acta Odontol Scand. 2003; 6:268-272
Frankenberger R, Krämer N, Sindel J. Repair strength of etched vs silica-coated metal-ceramic and all-ceramic restorations. Oper Dent. 2000; 25:209-215
Panah FG, Rezai SM, Ahmadian L. The influence of ceramic surface treatments on the micro-shear bond strength of composite resin to IPS Empress 2. J Prosthodont. 2008; 17:409-414
Conservative treatment of periodontal recessions with class v-defects using gingiva-shaded composite – a systematic treatment concept Hüsamettin Günay Werner Geurtsen Anne-Katrin Lührs Dental Update 2025 38:2, 124-132.
Authors
HüsamettinGünay
Professor (Dr med dent habil), Vice-Chairman, Department of Conservative Dentistry, Periodontology and Preventive Dentistry, Hannover Medical School, Carl-Neuberg-Straße 1, D-30625 Hannover Germany
Professor (Dr med dent habil), Chairman and Head of Department, Department of Conservative Dentistry, Periodontology and Preventive Dentistry, Hannover Medical School, Carl-Neuberg-Straße 1, D-30625 Hannover Germany, Affiliate Professor of Restorative Dentistry, University of Washington, Seattle, USA
Dr med dent, Senior Lecturer, Department of Conservative Dentistry, Periodontology and Preventive Dentistry, Hannover Medical School, Carl-Neuberg-Straße 1, D-30625 Hannover, Germany
Periodontal recessions can cause aesthetic and functional problems, especially in the anterior region or when combined with exposed crown margins. A combination of periodontal disease, recession with exposed root surface, hard-tissue defects and age emphasizes the need for treating these defects. If crown margins are exposed and surgical treatment is not possible, aesthetics and function can only be improved by replacement of the restoration. The restorative treatment option with a gingiva-shaded composite is especially valuable for dental fear patients or older patients with general or local risk factors, surgical contra-indications or Class III and IV recessions with questionable prognosis of surgery.
The step-by-step-approach described in this article is an alternative, minimal-invasive treatment concept for cervical lesions in combination with all kinds of periodontal recessions, that is especially suitable for wedge-shaped defects next to exposed crown margins.
Clinical Relevance: With this treatment concept, the reader should be able to use gingiva-shaded composite for different indications, such as exposed root surfaces or crown margins in combination with recessions.
Article
Periodontal recession often poses an aesthetic problem for patients. There are many causes for the formation of periodontal recession. It may appear without inflammation or formation of periodontal pockets, or can be understood either as symptoms or outcomes of untreated or treated periodontal diseases. The prevalence of periodontal diseases is high in ’senior’ patients and was determined to be up to 85% in a group of 60–69 year olds.1
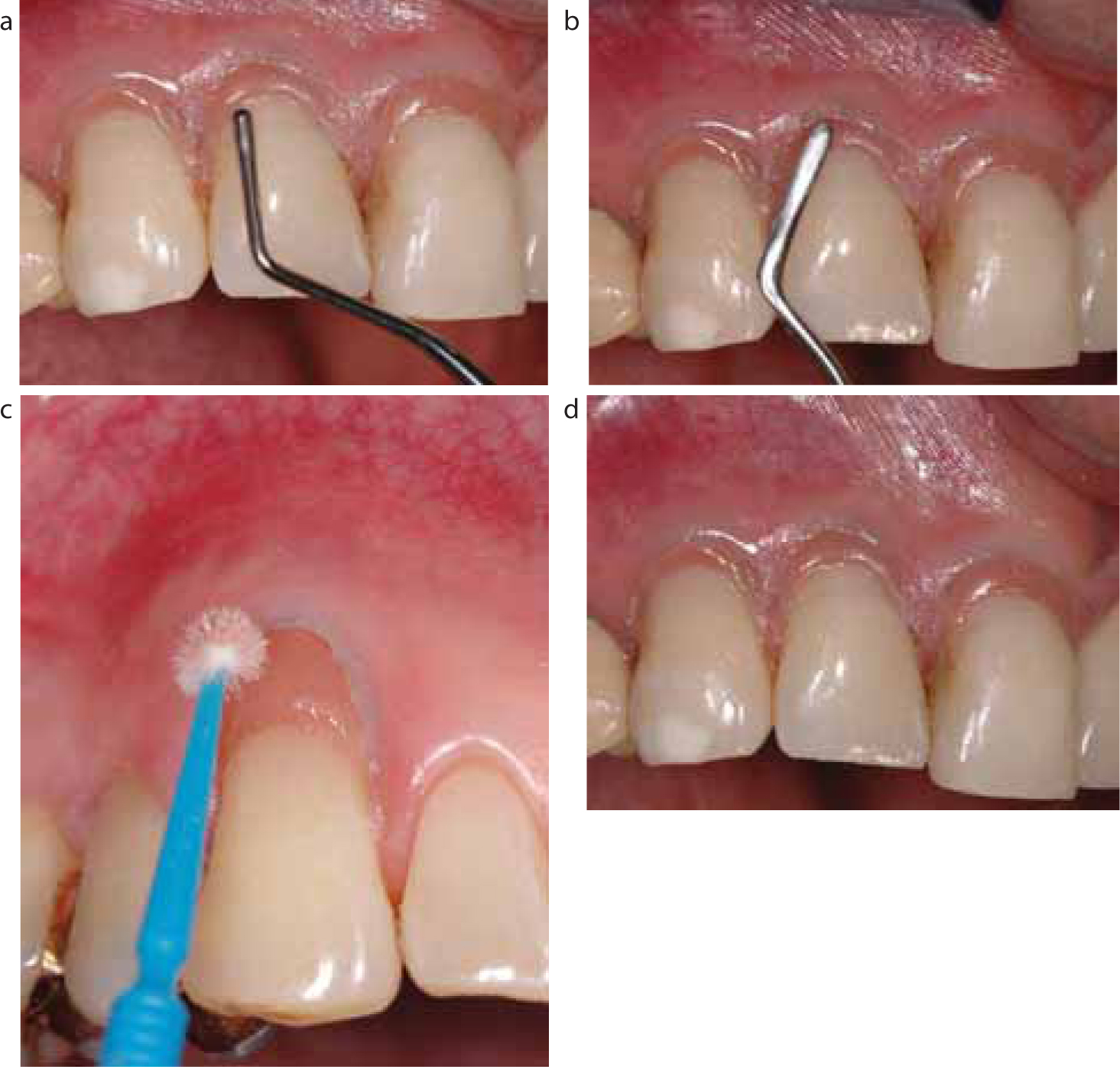
Regarding the location of gingival recession, facial/oral recession differs from proximal soft tissue lesions.2 Recession with traumatic origin is often located at the buccal area of canines and premolars. In contrast, circular recession regularly occurs in combination with general gingival inflammation.3 This leads to the conclusion of different aetiologies and pathogeneses for different types of gingival recession. As a consequence of recession, secondary damage to the exposed tooth and root surfaces often occurs. Cervical root areas are predisposed to secondary induced gingivitis or periodontitis and hypersensitivity due to difficult plaque control. The exposure of the root surface may lead to the formation of wedge-shaped defects and root caries by a combination of extrinsic, intrinsic and mechanical factors (Figure 1).4
Figure 1.
(a–c) Periodontitis and wedge-shaped defects as secondary damage of periodontal recessions in a 72-year-old patient: (a) before treatment; (b) 3 weeks after anti-infective therapy and (c) 5 years after periodontal and restorative therapy.
Because these defects are often found in combination with extensive gingival recession, loss of interdental bone and soft tissue, the prognosis for a surgical therapy is rather limited. Taking this into account, a need for creating a conservative treatment concept with the aim of tooth preservation exists. Deeper cervical lesions have to be treated with composite restorations because their proximity to pulpal tissues could trigger pulpal inflammation. To protect the tooth from further loss of hard tissues and hypersensitivity, cervical lesions with a depth of 0.5 mm and more should be treated restoratively in order to protect the marginal periodontal tissues, reduce hypersensitivity and improve aesthetics.5 The restorative treatment ensures the preservation of a healthy periodontal environment by means of caries prevention, inhibition of plaque accumulation and ’toothbrush trauma’.
The restoration of cervical defects associated with severe recession could lead to dissatisfying results, if tooth-coloured materials are used, because of the appearance of a disproportional elongation of the visible crown. Gingiva-shaded composites are therefore an alternative for a minimal-invasive and adhesive restorative treatment, especially if they are used in combination with tooth-coloured materials. A recent study on gingiva-shaded compomers showed a high patient satisfaction with the treatment outcome after two years and an aesthetic improvement compared to the initial situation.6
If a lesion (caries, erosion or wedge-shaped defect) is located adjacent to crown margins, questions arise regarding a conservative treatment concept without removal of the crown. If the restoration can be preserved, there are different options regarding the treatment of the cervical lesion:
Application of tooth- or gingiva-coloured materials;7,8
If a cervical lesion at a crown margin is combined with periodontal recession, the use of gingiva-shaded materials may improve the aesthetics while preserving the restoration, which is also a financial advantage for the patient combined with a reduced treatment time, in so far as the final restoration can be done in only one session.
This case report describes a systematic treatment concept for the restoration of cervical defects combined with gingival recession, particularly Miller Class III and IV,11 using gingiva-coloured composites.
Materials
The composite used for this step-by-step approach is Amaris® Gingiva which is part of the Amaris® system (Voco, Cuxhaven, Germany), a methacrylate-based composite with BIS-GMA, UDMA, TEGDMA used as matrix monomers and a filler content of 80 wt%. Amaris® Gingiva consists of the gingiva-shaded composite and three different-coloured flowables (‘opaquers’). The Amaris® system can be used with every methacrylate-based light curable adhesive system.
Step-by-step approach
Decision-making/’mock-up’
Before starting the restorative therapy, the aetiology of the gingival recession and the cervical defects should be determined through an accurate periodontal and diagnostic screening. An intra-oral pretherapeutic ’mock-up’ helps to visualize treatment results and helps the patient to select the restorative therapy (Figure 2). The ’mock-up’ can also be used before surgical recession treatment as decision guidance during the pre-therapeutic information.
Figure 2.
(a) Wedge-shaped defects on teeth UL3 and UL4 and recession (Miller Class I); (b, c) intra-oral ‘mock-up’ for demonstrating treatment results; (d) stable condition 8 years after surgical treatment.
Once a decision has been made for the restorative treatment, the tooth is cleaned with an adequate cleaning paste to remove organic and inorganic debris. In order to get good clinical results, a non-inflamed gingiva is mandatory prior to the restorative treatment, since bleeding caused by inflammation could impair the marginal seal and the aesthetics of the restoration (Figure 3).
Figure 3. Sound gingiva UR1–UR3 with no signs of inflammation before treatment in a 53-year-old patient.
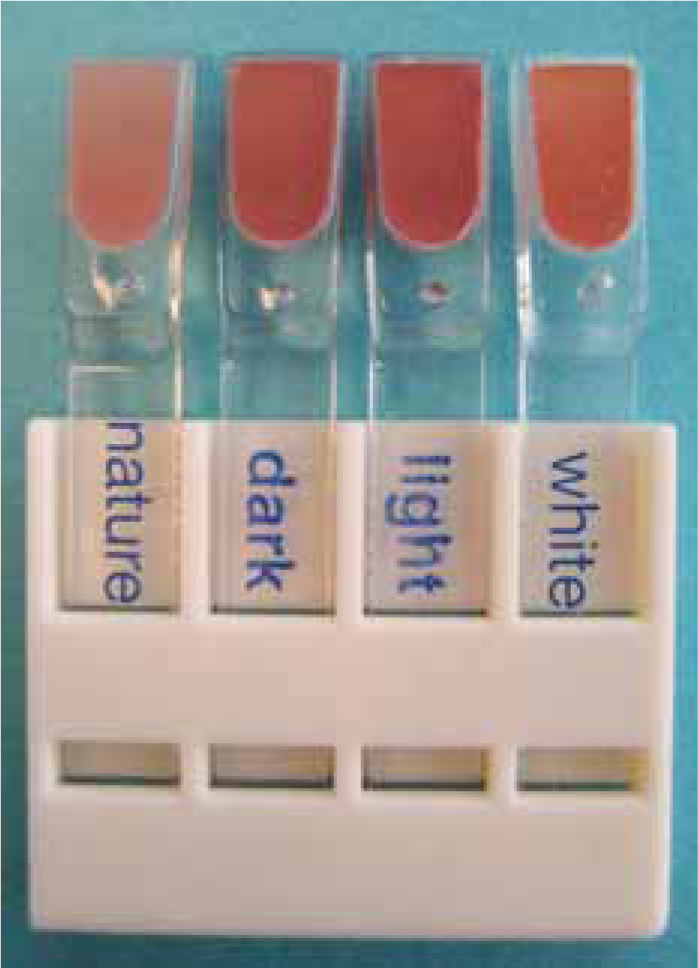
Selection of shade
The shade selection regarding the gingiva-coloured material should be done with the appropriate shade guide (Figure 4). The final shade will be achieved by the combination of different flowable opaquers with the viscous restorative material. The shade guide with the colour samples ’light’, ‘dark’, ‘white’ and ’nature’ (viscous material without opaquer) gives only a rough idea of the possible shade variations. Mixing of different opaquers and their combination with the restorative material allows an individual shade adaptation. If the incisal part of the cavity has to be restored with a tooth-coloured material, the shade has to be chosen with a second shade guide at the cervical third of the tooth. In case of large defects, adjacent teeth can help to decide about a certain shade.
Figure 4. Shade guide with the colour samples ‘light’, ‘dark’, ‘white’ and ‘nature’.
Preparation/pre-treatment of dental hard tissues
Any remnants of old restorations and caries have to be removed. If no caries is present and sclerotic dentine is exposed to the oral cavity, the surface should be roughened with burs in a minimally invasive way to expose sound dentine with a regular structure,4 which is also recommended by certain manufacturers, depending on the adhesive system used. A small chamfer is prepared at the gingival margin (mesial, cervical, distal) with small bud burs (size 08 or 10). This so-called ‘adhesive preparation’ helps to create well-defined restoration margins and to secure a better colour effect (Figures 5, 6). In deeper cavities, the application of a calcium hydoxide liner and/or a lining as pulp protection may be necessary. The area covered by the liner should be limited. Only the dentine close to the pulp should be covered in order to use the remaining dentine as bonding substrate for the adhesion of the restoration. In shallow cavities the bonding agent can be applied without any lining. If enamel is available, it is bevelled for approximately 1 mm using a fine-grit diamond with water spray. The bevel is of great advantage because it enlarges the enamel surface and allows the shaping of invisible restoration margins and improves the adhesion of the restoration.
Figure 5. Cross-sectional schematic view of the cavity – a slight approximal chamfer preparation leads to a precise cavity and a better colour adaption.Figure 6. Clinical view of the cervical and approximal chamfer preparation.
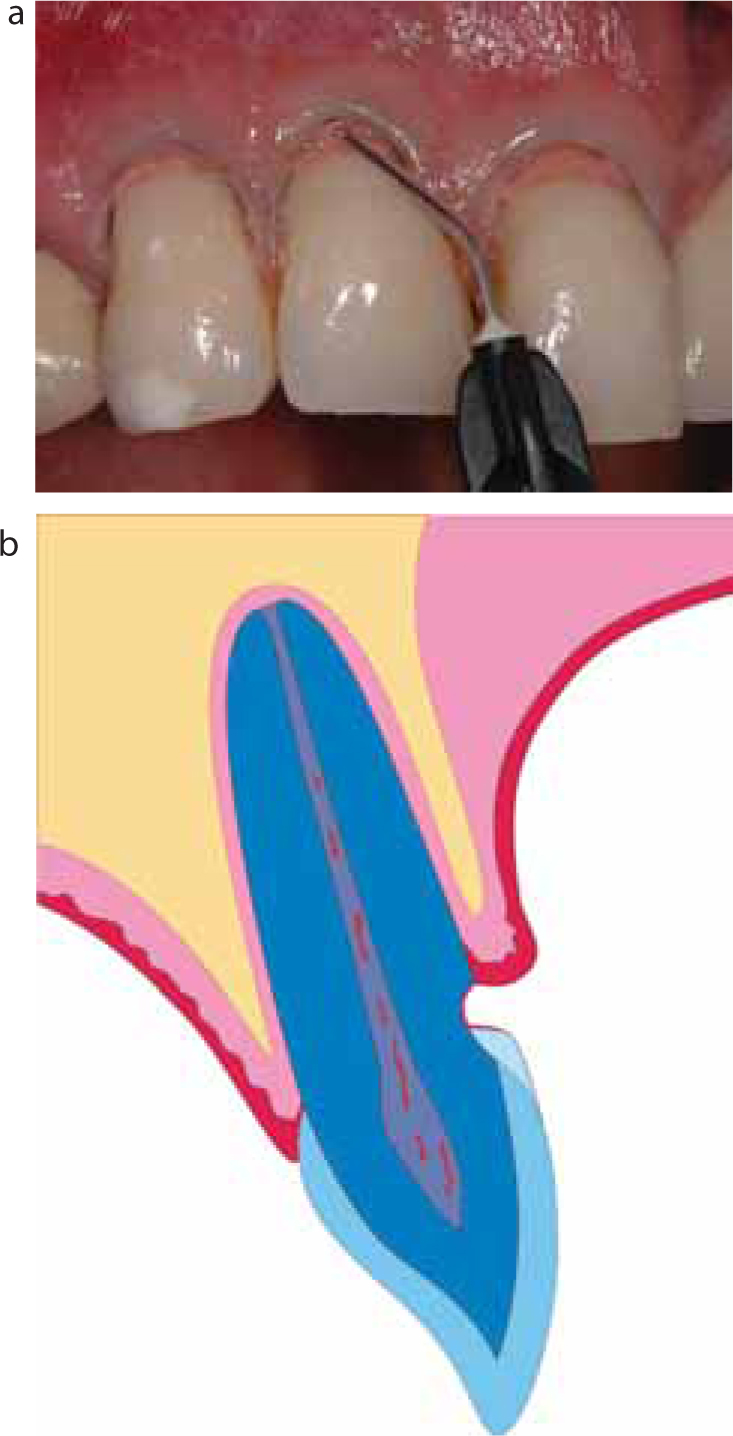
A retraction cord that helps to expose the cervical preparation margin is applied if the cavity extends into the sulcus or subgingival areas (Figure 7), in order to avoid trauma of adjacent soft tissues (eg Ultrapak, Ultradent, USA). After the application of the retraction cord, the cervical dentine margins should be finished.
Figure 7. Placement of the retraction cord with a special instrument (Packer® Ultradent, USA); cavity after the cervical preparation margin has been finished.
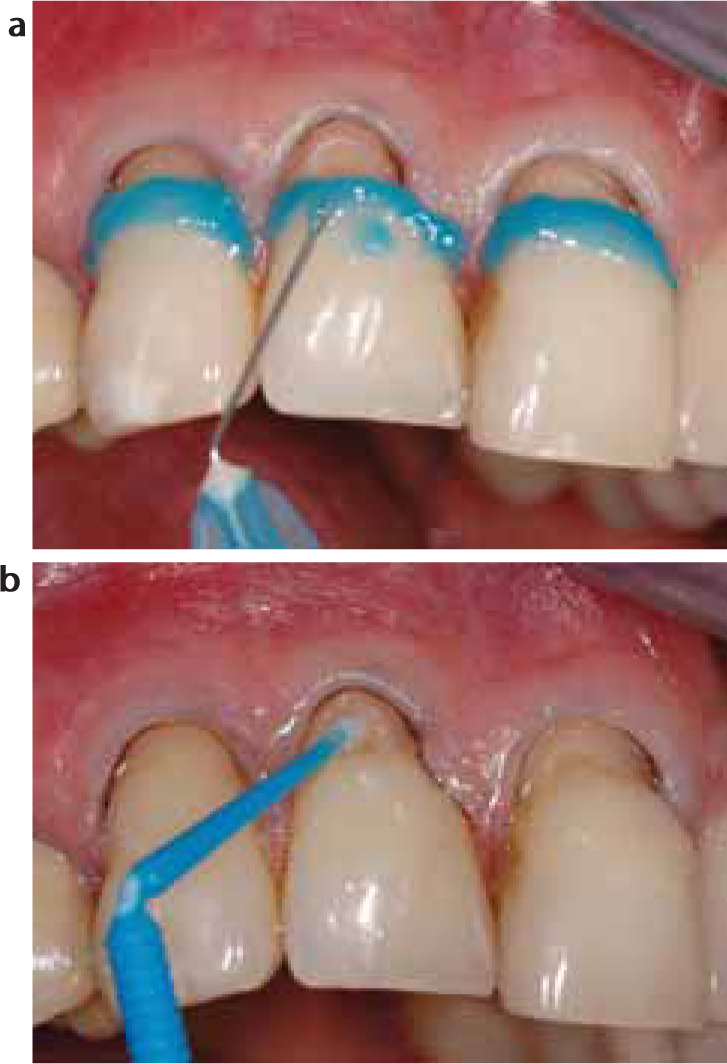
Dependent on the adhesive system, the enamel is etched with phosphoric acid (37%) for 30 seconds, rinsed and air-dried until the enamel reveals the typical frosty appearance of acid etching. Although an additional phosphoric etching is not mandatory for self-etch adhesives, recent studies showed that the enamel shear bond strength and the marginal integrity of these adhesives can be improved by a selective phosphoric acid etching.12,13 The adhesive is applied with a small brush, air-dried and light-cured for 20 seconds (Figure 8).
Figure 8.
(a) Etching of the enamel margins with phosphoric acid; (b) application of the adhesive system.
Restoration of the defect
The restoration is performed based on the systematic treatment concept as described by Günay and Lührs.7
If the incisal part of the cavity has to be restored with a tooth-coloured material, the placement of the increments is easier with specific shaping instruments that allow the adjustment of the material to the convex tooth profile. For shaping of the cervical cavity part, pear-shaped instruments are recommended (Figure 9).
Figure 9. Clinical view of the cavity – restoration of the incisal part of the cavity with a tooth-coloured composite and shaping of the composite with special carving instruments.
The flowable opaquer of the Amaris® system is then applied to cover the tooth surface, and light-cured for 40 seconds. The opaquer, which serves as an undercoat, leads to a natural appearance of the restoration and helps to maintain colour stability (Figure 10).
Figure 10.
(a) Clinical view of the flowable ‘opaquer’ which has to be applied after the restoration of the incisal part of the cavity in order to preserve the colour effect; (b) schematic view of the ‘opaquer’ layer.
Subsequently, the gingiva-shaded composite is applied (thickness maximum 2 mm per increment) and light-cured for 40 seconds per increment. The layers should not exceed the size of 2 mm in order to ensure the best possible polymerization. A gingival sulcus can be formed at the transition of the gingiva-shaded material to the incisal enamel or the tooth-coloured restoration. To avoid irritation of the gingiva and to facilitate oral hygiene, the cervical margin must not overlap the adjacent soft tissues (Figure 11a, b). The restoration should be polished and finished with fine-grit diamonds or carbide burs, flexible disks, the EVA-System® in combination with diamond-coated files or polishing cups and paste. Care should be taken regarding the restoration's morphology: the surface of the gingiva-shaded part should simulate the colour and texture of the gingiva (‘stippled’), which ensures the natural and aesthetic appearance of the restoration (Figure 11c). To ensure the long-term stability of the restoration, checkups after 1 to 3 weeks, 6 and 12 months have to be carried out (Figure 12).
Figure 11.
(a–d) Clinical view of the cavity – restoration of the cervical part of the cavity with a gingiva-shaded composite; shaping with the same instruments as in Figure 9; imitation of the ‘stippled’ gingiva by shaping the surface with a brush (c); clinical view immediately after restorative therapy (d).Figure 12.
(a–c) Clinical view of the restoration 1 week, 6 and 12 months after restorative therapy, no signs of gingival inflammation or recession, excellent aesthetic appearance.
Restorative therapy adjacent to exposed crown margins
The first steps during the treatment are the same as described above. The restorative therapy is then carried out as follows:
Crown margins have to be roughened: if a ceramic surface is present, the superficial glazed layer should be removed.
Afterwards, the tooth is isolated using rubber dam or a gingival matrix.
Ceramic or exposed metal surfaces are sandblasted for 10 sec with CoJet-Sand (CoJet™-System, 3M ESPE, Seefeld, Germany) perpendicular to the surface at a distance of 2–10 mm (pressure: 2–3 bar).
After sandblasting, remnants of the silica-coating process are removed with dry air.
Sandblasting is followed by the application of a silane (ESPE Sil, 3M ESPE, Seefeld, Germany) which should be dried for 30 sec. Any contamination with oral fluids, for example saliva, should be avoided.
If a metal surface is exposed, it should be covered by a thin layer of opaquer (Synfony, 3M ESPE, Seefeld, Germany) which has to be polymerized for 10 sec. If no metal surface is exposed, this step is not necessary.
The last step is the application and polymerization of the adhesive system. The pre-treatment of the dentine surface should be carried out with a ‘conventional’ total etch-adhesive.
When using a system that requires multiple steps after etching with phosphoric acid, only the system's bonding agent has to be applied to the pretreated veneering material and the opaquer-covered metal. The use of self-etch adhesive systems results in a decreased bond strength of composite on ceramic.14 In order to obtain a satisfactory colour with the ceramic surface, the gingiva-shaded material can be combined with a tooth-coloured material (Figure 13).
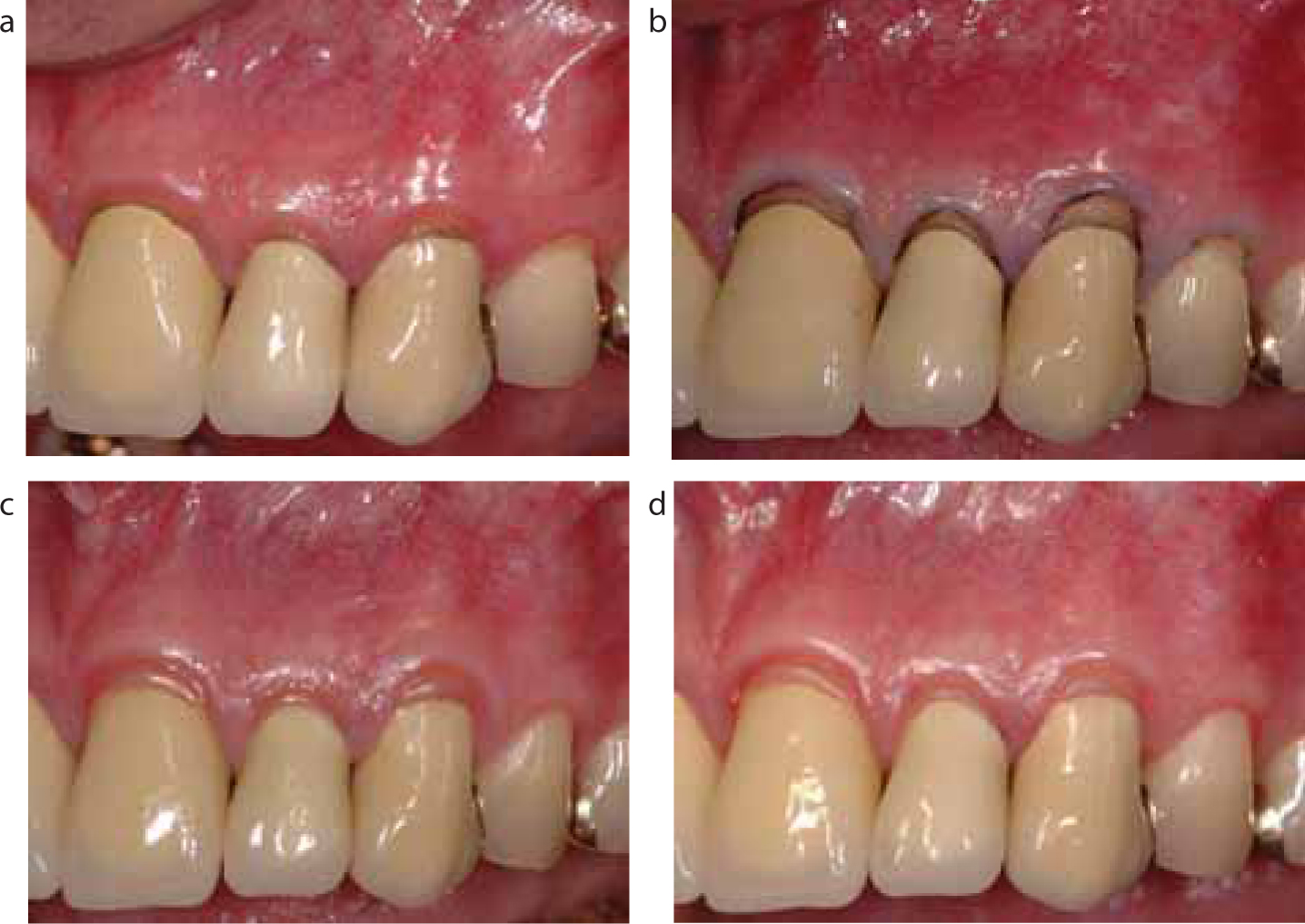
Figure 13.
(a–d) Restoration of wedge-shaped defects adjacent to visible crown margins as treatment alternative in order to preserve the fixed crowns: (a) before treatment; (b) cavity after preparation and finishing with placed retraction cord; (c, d) 6 and 12 months after restorative therapy with a gingiva-shaded composite in a 58-year-old patient.
Discussion
The step-by-step approach presented in this paper introduces a systematic treatment concept for periodontal recessions in combination with Class V-defects using gingiva-shaded composites. It is a conservative alternative to a surgical treatment, especially for seniors or anxious patients with systemic or oral risk factors, or in cases when a surgical treatment is contra-indicated. The presented restorative concept allows aesthetically and functionally satisfying results to generate with minimal intervention. Today's literature provides only little information concerning gingiva-shaded materials owing to the scarce number of case reports; a systematic treatment concept has not yet been described.8,15
Treatment concepts that are only minimally invasive become increasingly important. The age pattern of our society is changing, leading to an increased proportion of patients with periodontal diseases. Of patients who are older than 41 years, 91% suffer from at least one buccal recession.16 In current studies, 48% of the remaining teeth in the age-group of 60 to 69-year-olds revealed recessions.1
Owing to the exposure of the root surface to oral fluids, bacterial colonization and mechanical irritation, the probability of the formation of carious lesions or non-carious defects is elevated.17 Compared to enamel, a root that is exposed by gingival recession shows a rougher surface, and therefore a higher risk of plaque accumulation and formation of root caries. It was demonstrated by Schiffner et al that 42.1% of 35 to 44-year-old adults show erosions or wedge-shaped defects. In the group of 65 to 74-year-olds the percentage was 46.3%.18 The prevalence of root caries is 42% in patients with an average age of 42.19 Senior patients older than 70 years who live in senior residences showed root caries in 48% of all cases.20 The DMS IV-Study revealed a decline of caries in adults, except for root caries the incidence of which increased from about 10.7% to 21.5% for adults and from about 30.5% to 45% for senior patients in the years 1997 to 2005.21,22
The ’German DMS IV-Study’ also showed that 45% of all root surfaces within the age cohort of senior patients were affected by caries or treated with restorations. Even in the group of 35 to 45-year-old patients, 16.9% of the adults suffered from erosive or wedge-shaped defects; this percentage increased with age (age 65 to 74 years) to 29.3%.21,22 Modern dental prevention allows the preservation of teeth up to a greater age. Patients 50 to 60 years old revealed an average number of 22 teeth.23 The preservation of natural teeth with an associated increase in risk for root caries entails an elevated number of cervical carious lesions and wedge-shaped defects, which corresponds with the patient's age.18 Of non-edentulous senior patients, 46.3% suffer from such lesions, with an average number of 2 to 3 teeth showing erosive or wedge-shaped defects.
Cervical lesions often appear after periodontal recession at the cervical margin of prosthodontic restorations: the concept presented in this report allows for successful treatment of these defects with minimally invasive intervention while preserving the prosthodontic piece.
It is recommended to roughen sclerotic dentine surfaces prior to the adhesive procedure. For self-etching systems, the microtensile bond strength to sclerotic dentine was lower than to sound dentine, independent of a previous acid etching.24 But it should be emphasized that the manufacturers' instructions for adhesive systems are inconsistent regarding the surface pre-treatment. In some cases, roughening of the exposed dentine is required, for other systems, a cleaning of the surface with pumice is sufficient to remove organic and inorganic debris. Wedge-shaped defects that were exposed to the oral cavity over a longer period of time show a hypermineralized surface. The removal of this layer is discussed controversially in today's literature. A clinical long-term study revealed a low longevity for composites used in non-carious Class V-lesions, especially when ‘all-in-one’ adhesive systems were used.25
Apart from case reports, no scientific research has been published regarding the long-term stability of composite restorations placed adjacent to crown margins so far.8,26 For the intra-oral repair of fractured veneering ceramic, research on possible treatment concepts has been published.27–29 The ceramic surface could be pre-treated with either hydrofluoric acid, air abrasion or silica-coating followed by silane application. Regarding ceramic repair with composite, the shear bond strength obtained by silica-coating compared to etching with hydrofluoric acid was equal or higher for the silica-coating method.28 Therefore, the authors prefer the use of silica-coating combined with a silane coupling agent for the use of gingiva-shaded composites adjacent to crown margins. With this system, different substrates, eg ceramic and exposed metal surfaces, can be pre-treated by using only one technique.
Conclusions
Owing to our society's changed age pattern, treatment concepts that are minimally invasive become more important. This process leads to a growing proportion of ‘senior’ patients who are able to preserve an increased number of teeth owing to dental prevention. As a consequence, the growing number of exposed root surfaces with caries, erosions and wedge-shaped defects requires alternative treatment concepts. The methods described in this report can be used to treat recessions of all classes and is especially of advantage for dental fear patients or older patients with general or local risk factors, surgical contra-indications or Class III and IV-recessions with questionable prognosis of surgery. Another important indication is the restoration of cervical defects adjacent to exposed crown margins. Also, fixed dentures can be preserved, which is of financial benefit for the patients. This restorative treatment option results in aesthetic, functional and long-lasting results. Moreover, the gingiva-shaded composite can be used as an intra-oral ’mock-up’ prior to surgical intervention to visualize post-operative treatment results.