Lee IB, Son HH, Um CM. Rheologic properties of flowable, conventional hybrid, and condensable composite resins. Dent Mater. 2003; 19:298-307 https://doi.org/10.1016/s0109-5641(02)00058-1
Zimmerli B, Strub M, Jeger F Composite materials: composition, properties and clinical applications. A literature review. Schweiz Monatsschr Zahnmed. 2010; 120:972-986
Willems G, Lambrechts P, Braem M A classification of dental composites according to their morphological and mechanical characteristics. Dent Mater. 1992; 8:310-319 https://doi.org/10.1016/0109-5641(92)90106-m
Randolph LD, Palin WM, Leprince JG. Developing a more appropriate classification system for modern resin-based composite technologies. In: Miletic V (ed). Switzerland: Springer; 2018
Cramer NB, Stansbury JW, Bowman CN. Recent advances and developments in composite dental restorative materials. J Dent Res. 2011; 90:402-416
Baroudi K, Rodrigues JC. Flowable resin composites: a systematic review and clinical considerations. J Clin diagnostic Res. 2015; 9:ZE18-24
Firla MT. Seventeen years of using flowable resin restoratives. A dental practitioner's personal clinical review. Dent Update. 2015; 42:261-268
García AH, Lozano MAM, Vila JC Composite resins. A review of the materials and clinical indications. Med Oral Patol Oral Cir Bucal. 2006; 11:E215-220
Juloski J, Goracci C, Rengo C Enamel and dentin bond strength of new simplified adhesive materials with and without preliminary phosphoric acid-etching. Am J Dent. 2012; 25:239-243
Chesterman J, Jowett A, Gallacher A, Nixon P. Bulk-fill resin-based composite restorative materials: a review. Br Dent J. 2017; 222:337-344
Van Ende A, De Munck J, Lise DP, Van Meerbeek B. Bulk-Fill composites: a review of the current literature. J Adhes Dent. 2017; 19:95-109
Van Dijken JW, Pallesen U. Posterior bulk-filled resin composite restorations: A 5-year randomized controlled clinical study. J Dent. 2016; 51:29-35
Karaman E, Keskin B, Inan U. Three-year clinical evaluation of class II posterior composite restorations placed with different techniques and flowable composite linings in endodontically treated teeth. Clin Oral Investig. 2017; 21:709-716
Bayraktar Y, Ercan E, Hamidi MM, Çolak H. One-year clinical evaluation of different types of bulk-fill composites. J Investig Clin Dent. 2017; 8:1-9
Jain G, Narad A, Boruah L, Rajkumar B. Comparative evaluation of shear bond strength of three resin based dual-cure core build-up materials: an in-vitro study. J Conserv Dent. 2015; 18:337-341
Zankuli MA, Devlin H, Silikas N. Water sorption and solubility of core build-up materials. Dent Mater. 2014; 30:324-329
Zankuli MA, Silikas N, Devlin H. The effect of cyclic loading on the compressive strength of core build-up materials. J Prosthodont. 2015; 24:549-552
Tauböck TT, Oberlin H, Buchalla W Comparing the effectiveness of self-curing and light curing in polymerization of dual-cured core buildup materials. J Am Dent Assoc. 2013; 142:950-956
Muttlib NAA, Pungut N, Alawi R. The use of fiber reinforced composite post in restoring a wide and compromised canal: a case report. Der Pharm Lett. 2018; 10:66-72
Bansal R, Burgess J, Lawson NC. Wear of an enhanced resin-modified glass-ionomer restorative material. Am J Dent. 2016; 29:171-174
Gandolfi MG, Siboni F, Prati C. Chemical-physical properties of TheraCal, a novel light-curable MTA-like material for pulp capping. Int Endod J. 2012; 45:571-579
Camilleri J, Laurent P, About I. Hydration of Biodentine, Theracal LC, and a prototype tricalcium silicate-based dentin replacement material after pulp capping in entire tooth cultures. J Endod. 2014; 40:1846-1854
Dafar MO, Grol MW, Canham PB Reinforcement of flowable dental composites with titanium dioxide nanotubes. Dent Mater. 2016; 32:817-726
Tavassoli Hojati S, Alaghemand H, Hamze F Antibacterial, physical and mechanical properties of flowable resin composites containing zinc oxide nanoparticles. Dent Mater. 2013; 29:495-505
Kattan H, Chatzistavrou X, Boynton J Physical properties of an Ag-doped bioactive flowable composite resin. Materials. 2015; 8:4668-4678
Xu HHK, Weir MD, Sun L Strong nanocomposites with Ca, PO4, and F release for caries inhibition. J Dent Res. 2010; 89:19-28
Lassila L, Säilynoja E, Prinssi R Characterization of a new fiber-reinforced flowable composite. Odontology. 2019; 107:342-352
Yusoff NM, Johari Y, Ab Rahman I Physical and mechanical properties of flowable composite incorporated with nanohybrid silica synthesised from rice husk. J Mater Res Technol. 2019; 8:2777-2785
AL-Rawas M, Johari Y, Mohamad D Water sorption, solubility, degree of conversion, and surface hardness and topography of flowable composite utilizing nano silica from rice husk. J Mater Res Technol. 2021; 15:4173-4184 https://doi.org/10.1016/j.jmrt.2021.10.024
The versatility of flowable composites. Part 1: theory and new classification Matheel AL-Rawas Yanti Johari Nazrul M Yusoff Dasmawati Mohamad Adam Husein Dental Update 2025 49:7, 553-560.
Authors
MatheelAL-Rawas
BDS, MResDent (Prosthodontics), FRACDS
Specialist and Clinical Lecturer, Prosthodontic Unit, School of Dental Sciences, Universiti Sains Malaysia; Hospital Universiti Sains Malaysia
BDSc, Grad DipClinDent, DClinDent, FRACDS, Senior Lecturer, Prosthodontics Unit, School of Dental Sciences, Universiti Sains Malaysia, Kelantan, Malaysia.
The increase in consumer demand for restorative and aesthetic dental treatment has resulted in a gradual upsurge of dental professionals relying on flowable composites (FCs) to meet consumer needs. All main manufacturers in the worldwide dental market offer flowable products together with the packable type. Scientific and technological improvements of FCs properties and handling characteristics have not only seen FCs grow in popularity but resulted in the development of different generations and types of dental FCs suitable for wide range of clinical applications.
CPD/Clinical Relevance: It is useful for the dental practitioner to be aware of the classifications, composition and overview of FCs.
Article
Matheel AL-Rawas
Resin composites are classified as universal, packable or flowable according to their viscosity and consistency.1,2 This, along with other classifications,1,3–7 serves as a guide to practitioners, enabling them to identify and select the most suitable materials on a case-by-case basis (Figure 1).
Figure 1. Summary of all classifications related to resin composites.
The viscosity of resin composites can be reduced by decreasing the filler content, lowering the viscosity of the monomers, heating, and through ultrasonic vibration. All these methods produce less viscous composites that are easy to apply in cavities and possess excellent marginal sealability. Therefore, it is valuable to review the composition of each flowable composite (FC) to better understand the performance, capabilities and limitations of each type.
Composition
An FC typically consists of three primary substances: monomers; fillers; and a coupling agent.8 The physical and mechanical properties of an FC vary based on the type, size, shape, loading, porosity and geometry of its filler.8 A monomer, however, serves as a filler dispersion matrix that gives an FC its structure, while the type of monomer used affects the characteristics of the final FC. Therefore, the viscosity of the monomer mixture, as well as the choice of filler, must be carefully selected to produce a flow property that matches the intended usage. Additionally, a silane coupling agent is a chemical that bonds fillers to monomers. Table 1 summarizes FC compositions.
Formulation
Main components
Resin matrix
Methylacrylate monomers, such as Bis-GMA, UDMA, HEMA, TEGDMA, BisEMA and others
Inorganic filler
Filler particles, such as quartz, silica, silicate glass, strontium, alumina, zirconia, barium and glass and others
Coupling agent
Silane agents, such as MPTS, MPDMS or γ-MPS
Photo-initiator system
CQ, PPD, Lucirin TPO or benzyl peroxide
Acceleration system
DMAEM, EDMAB or CEMA
Stabilizer or inhibitor system
Hydroquinone monomethyl ether to optimize the product's storage life before curing and its chemical stability
Absorbers
2-hydroxy-4-methoxybenzophenone, to provide colour stability and eliminate the effects of UV light on the amine compounds in the initiator system
Flowable composite as a versatile material
The flowability of resin composites varies between brands and manufacturers. This can range from low, medium or high flowability as shown in Figure 2. Therefore, the choice of brand depends on the nature of the cavity and the clinician's preference.
Figure 2. Different flowability after 60 seconds of three different conventional FCs by using the drip method.
One might ask why flowability is significant. The handling of composite resin with a putty-like consistency for dental restoration may not be easy or successful, especially for small cavities, which can be 2 mm in diameter and depth, and with difficult access. By contrast, a flowable composite is adaptable, even for the tiniest defects in tooth structure, and does not result in voids, porosity, or gaps as typically found when a putty-like material is used.9
An FC should be an extrudable, flowable, steady and slumping slurry to achieve the optimal clinical results.10 Its advantages include wettability and penetration of a minimum thickness layer into all defects, resulting in no air inclusion or entrapment, a low flexural modulus of elasticity that reduces the likelihood of composite displacement from restored cavitated dentine lesions and cervical (wear) lesions, and its availability in different shades and radiopacities. Its clinical drawbacks, however, include higher shrinkage upon curing due to the low filler content of some conventional FCs, weak resistance to wear and poor mechanical properties.11 However, these drawbacks depend on which type of flowable composite material is used, and this should not deter clinicians from using FCs in suitable clinical procedures.
Types of flowable composites
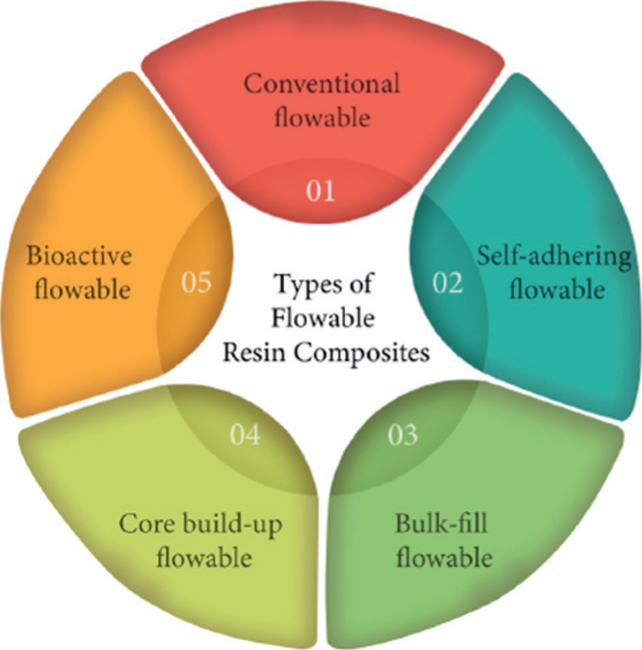
Within this review, a new classification of flowable composites is proposed based on their unique usages, such as conventional FCs, self-adhering FCs, bulk-fill FCs, core build-up FCs and bioactive (repair) flowable types. Figure 3 shows the new proposed FC classification.
Figure 3. New proposed FC classification.
Conventional FCs
Conventional FCs cannot be applied in bulk or be used as a core build-up material. Furthermore, they have no bioactive repairing properties or self-adhesive features. These FCs need to be applied with minimal thickness, using a conventional bonding technique. They are indicated for various situations, including as a fissure sealant or a liner under a restoration, and in the restoration of a class V cavity. These situations will be addressed in depth with evidence in Part 2 after discussing other types of flowable composites. Table 2 provides a list of the available commercial products as well as their composition.
A more recent development in the field is the introduction of self-adhering FCs that contain functional monomers to promote adhesion to tooth structures without etching, rinsing or drying.12
These products are generally indicated for use only as a liner, porcelain repair and pit-and-fissure sealant. However, incidents of microleakage are more prevalent with this type of FC in comparison to conventional FCs. While a self-adhering flowable would be a dentist's dream, more studies are needed to look at their long-term clinical success.
Bulk-fill FCs
Manufacturers have developed a variety of resin-based composites to simplify the application protocol for posterior restorations deeper and wider than 4 mm to a single step. Known as bulk-fill materials, they can be classified as light or dual-cured, high- or low-viscosity resin composites.13Table 3 provides a list of some of the commercial products available at present, as well as their specific requirements and features.13,14
Product name (manufacturer)
Maximum layer thickness (mm)
Filler content by weight (%)
Available shades
Length of cure in seconds (s) according to manufacturer's instructions
Lowest intensity (550 mW/cm2)
1000 mW/cm2 or greater intensity
X-tra base (Voco)
4
75
Universal
10
10
A2
40
20
Surefil SDR Flow (Dentsply)
4
68
Universal
20
No additional recommendation
A1
A2
A3
Venus bulk-fill (Heraeus Kulzer)
4
65
Universal
20s
No additional recommendation
Filtek bulk-fill flowable (3M ESPE)
4
65
Universal
20s
10
A1, A2, A3
40s
20
Tetric EvoFlow bulk-fill (Ivoclar Vivadent)
4
68.2
Universal shades: IVA, IVB, IVW
20s
10
With regard to clinical performance, in vitro and in vivo studies have shown that bulk-fill FCs are appropriate for use in restorative dentistry alongside other restorative materials.15–17
In a randomized clinical trial, a bulk-fill (SureFil SDR flow, Dentsply Sirona) was capped with a nanocomposite and compared to a conventional FC applied using the incremental technique. The authors found comparable success over 5 years. The annual failure rate (AFR) was 1.4% and 2.1%, respectively, for the SDR and conventional FC in Class II restorations and zero AFR in Class I restorations.15 Another randomized clinical trial compared 3M Filtek Bulk Fill Flowable Restorative capped with Filtek P60 Posterior Restorative, Tetric EvoCeram Bulk Fill, SonicFill 3 SingleFill Composite System and a nanohybrid composite. These products were used on 172 Class II restorations in 43 patients. At 1-year follow up, all restorations were found to be in acceptable condition with no observable differences between the products.17 Karaman et al conducted a randomized clinical trial of Class II restorations in non-vital teeth using VOCO x-tra base bulk-fill FC capped with nano-hybrid VOCO Grandio and compared with restorations made from BISCO Dental AELITEFLO conventional FC capped with nano-hybrid VOCO Grandio applied using the incremental technique. Both methods of restoration were found to be acceptable and comparable in their clinical performance throughout the 3-year evaluation period.16
Bulk-fill FCs offer efficient, less time-consuming and less technique sensitive tooth-coloured restorations compared to conventional flowable and packable composites. These materials can be especially beneficial for restoring cavities when procedural time is particularly critical, for example in children and nervous patients. Although these results were encouraging, further clinical studies, with evaluation periods of longer than 5 years, are required to establish long-term clinical performance and longevity, as well as possible flowability improvements to withstand occlusal forces without a cap.
Core build-up low and medium viscosity FCs
These materials can be applied to badly broken vital or non-vital teeth, as well as to restore and fortify weak spots. The core material can be a cast or plastic core acting as a foundation for the tooth. This allows the practitioner to establish a favourable form to enhance the resistance and retention of the overlying prosthesis. Resin composite is considered one of the plastic core materials.
Core build-up composite materials come in different viscosities: low, medium and high. Table 4 highlights some core build-up materials with different flow properties.
Material name
Company
Curing mode
Viscosity
Filler loading (weight %)
Luxacore Z Automix Dual
DMG
Dual
Low
70
Paracore Automix
Coltene/Whaledent
Dual
Medium
74
Rebilda DC Automix
Voco GMBH
Dual
Low
70
Grandio core Automix
Voco GMBH
Dual
Low
77
Compcore AF Automix
Premier
Dual
Low
Not available
Core.X flow
Dentsply/caulk
Dual
Low
69
Core paste/XP syringe Automix
Den-mat
Dual or self
Low
Not available
Clearfil DC core plus\ Automix
Kuraray America
Dual
Medium
74
Clearfil core new bond
Kuraray America
Self
Medium
78
Multicore Flow
Ivoclar Vivadent
Self with light-cured option
Low
70
Three studies have tested and compared the properties of these materials. One study investigated the shear bond strength (SBS) of three different build-up materials. One of the materials, MultiCore dual-cure resin (Ivoclar Vivadent, Liechenstein) had the best mean SBS relative to the other tested materials.18 Another two studies concluded that all build-up composites were found to have acceptable water sorption and solubility, and could last 1 year in service without compromising on compressive strength.19,20
Tauböck et al detailed that exposing dual-cured materials to light imparted no additional microhardness benefits over self-cured materials. Self-curing materials allow them to be placed in areas with little to no light exposure.21 Significant differences were found in the physical and mechanical properties of various core composite materials. Flowable or injectable core build-up materials are considered crucial for endodontically treated, badly broken teeth because they can be used to fill the prepared canal as a luting material, followed by build up of the coronal part of the tooth. These materials help to ensure an adequate seal and flow into all irregularities of the preparation and reduce the chairside time. An example of this situation is when a clinician has a widened canal that cannot be fitted with any of the prefabricated posts available. In one report, instead of prescribing the indirect cast post core, a fibre-reinforced composite post (everStick, Stick Tech Ltd, Turku, Finland) was cemented with core build-up material.22 This is made possible due to the flowability and injectability of the material to ease the adaptability to the tooth structure. Once again, flowable composite in the form of core build-up proved to be an essential material to the restorative dentist.
Bioactive repair flowable products
Some active materials have both a flowable consistency and chemical effects on pulpal tissues. Such products include Pulpdent Corporation's (USA) ACTIVA BioACTIVE – RESTORATIVE and ACTIVA BioACTIVE – BASE/LINER that combine the benefits of composites with glass ionomers.23 These materials can chemically bond to teeth, release and recharge with ions, have a good seal against microleakage and are strong and resistant to wear and fracture.24 One short-term study of two cases reported no complaints of post-operative tooth sensitivity. While the authors of the study lauded the materials as a significant development in the field of adhesive restorative dentistry, they recommended that longer-duration studies should be conducted in the future.24
Bioactive FCs, such as Beautifil Flow Plus and Plus X (Shofu, Japan), which contain Giomer, a proprietary filler particle, can release fluoride ions and reduce the rate of secondary caries. One clinical evaluation of Class I and II restorations with a 13-year recall, showed good retention rates and few secondary caries. Table 5 displays the available bioactive Giomer products.25
Material name
Matrix
Filler type
Beautifil Flow F02 and F10 (Giomer)
Bis-GMA, TEGDMA
S-PRG filler based on fluoroboroaluminosilicate glass
Beautifil Flow Plus F00 and F03 (Giomer)
Bis-GMA, TEGDMA
S-PRG filler based on fluoroboroaluminosilicate glass
Beautifil Flow Plus X F00 and F03 (Giomer)
Bis-GMA, TEGDMA
S-PRG filler based on fluoroboroaluminosilicate glass
FIT SA F03 and F10 (self-adhesive Giomer)
UDMA, HEMA, phosphonic acid monomer
S-PRG filler based on fluoroboroaluminosilicate glass
Beautifil-Bulk Flowable (Giomer)
Bis-GMA, UDMA, Bis-MPEPP, TEGDMA
S-PRG filler based on fluoroboroaluminosilicate glass
BISCO Dental TheraCal LC26 is a light-cured resin-modified calcium silicate product indicated for use in direct and indirect pulp capping procedures that has favourable effects in comparison to calcium hydroxide. It also has acceptable sealing capabilities and tolerated immortalized odontoblast cells well.26 Although Gandolfi et al mentioned that TheraCal can release calcium and hydroxyl ions and alkalinize the surrounding fluids to increase the pH,26 Camilleri et al showed that the calcium-releasing ability is limited, and less than that of Biodentine, which may affect calcium hydroxide formation and limit the reparative properties of TheraCal.27 However, the same author claimed the possibility that the released calcium ions were not in hydroxide form.27 Compared to calcium hydroxide-based products, the ability of TheraCal to be light cured is a potential advantage to dental practitioners to avoid setting failure and potential microleakage.
However, despite the unique features of these products and their encouraging studies, additional in vitro and in vivo studies of both materials are required to further evaluate long-term clinical outcomes.
Progress in flowable composite products
The past 6 years have seen researchers incorporate small amounts of additional fillers to FCs to improve their properties. Some researchers have added titanium oxide nanotubes, which showed that the addition of an optimal concentration of filler substantially improved the physical and mechanical properties of commercial FCs.28 Other studies incorporated silver-doped bioactive glass and zinc oxide fillers to integrate antibacterial properties into commercial FCs. Although the addition of these fillers enhanced bacterial inhibition, some properties were adversely affected.29,30 Another group has tried to include antibacterial agents, such as fluoride,31 to kill bacteria or inhibit biofilm formation.
Another study explored the use of smart-release composites that depend on the acidic challenge of the oral environment to slowly release calcium and phosphate in order to enhance the remineralization process.31 A recent study embedded experimental glass microfibre in an FC and compared it with various commercial FCs. The properties of the formulated FC were considerably superior to those of its commercial counterparts.32 Yusoff et al and AL-Rawas et al fabricated an FC with a unique rice husk-derived silica filler and concluded that the rice husk-based silica filler FC possessed acceptable physical and mechanical properties, and could potentially be used in dentistry.33,34
Conclusion
Flowable composites are versatile materials and can offer easy application and distinctive qualities. Based on current clinical and laboratory experiments, further research and clinical trials are needed to improve the various properties of the different FC products, such as self-adhering FCs and bulk-fill FCs. More studies are needed on the self-repairing and antimicrobial properties of FCs, as well as on resin composites for hard dental tissue regeneration. Studies that aim to develop environmentally friendly and sustainable flowable products through recycling waste materials to reduce carbon emissions from the manufacturing procedure and its effects on the environment should be encouraged. The production of such FCs would not only improve oral health, but also the quality of life.