Moller AJ, Fabricius L, Dahlen G Influence on peri-apical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys. Scand J Dent Res. 1981; 89:475-484 https://doi.org/10.1111/j.1600-0722.1981.tb01711.x
Kakehashi S, Stanley HR, Fitzgerald RJ The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965; 20:340-9 https://doi.org/10.1016/0030-4220(65)90166-0
Haapasalo M, Udnæs T, Endal U Persistent, recurrent, and acquired infection of the root canal system post treatment Endod Topics. 2003; 6:29-56 https://doi.org/10.1111/j.1601-1546.2003.00041.x
Byström A, Sundqvist G Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981; 89:321-328 https://doi.org/10.1111/j.1600-0722.1981.tb01689.x
Byström A, Sundqvist G Bacteriologic evaluation of the effect of 0.5 percent sodium hypochlorite in endodontic therapy. Oral Surg Oral Med Oral Pathol. 1983; 55:307-312 https://doi.org/10.1016/0030-4220(83)90333-X
Nair PN, Sjögren U, Krey G Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant peri-apical lesions: a long-term light and electron microscopic follow-up study. J Endod. 1990; 16:580-588 https://doi.org/10.1016/S0099-2399(07)80201-9
Lin LM, Pascon EA, Skribner J Clinical, radiographic, and his-tologic study of endodontic treatment failures. Oral Surg Oral Med Oral Pathol. 1991; 71:603-611 https://doi.org/10.1016/0030-4220(91)90371-I
Sjögren U, Figdor D, Persson S, Sundqvist G Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997; 30:297-306 https://doi.org/10.1046/j.1365-2591.1997.00092.x
Shuping GB, Ørstavik D, Sigurdsson A, Trope M Reduction of intracanal bacteria using nickel-titanium rotary instrumentation and various medications. J Endod. 2000; 26:751-755 https://doi.org/10.1097/00004770-200012000-00022
Collin V, ÓSelmo E, Whitehead P Psychological distress and the perceived impact of the COVID-19 pandemic on UK dentists during a national lockdown. Br Dent J. 2021; 22:1-8 https://doi.org/10.1038/s41415-020-2592-5
Tait CM, Ricketts DN, Higgins AJ Restoration of the root-filled tooth: preoperative assessment. Br Dent J. 2005; 198:395-404 https://doi.org/10.1038/sj.bdj.4812187
Rotstein I, Simon JH Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontol 2000. 2004; 34:165-203 https://doi.org/10.1046/j.0906-6713.2003.003431.x
Gutmann JL Prevalence, location, and patency of accessory canals in the furcation region of permanent molars. J Periodontol. 1978; 49:21-26 https://doi.org/10.1902/jop.1978.49.1.21
Sjögren U, Figdor D, Spångberg L, Sundqvist G The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J. 1991; 24:119-125 https://doi.org/10.1111/j.1365-2591.1991.tb00117.x
Tronstad L, Andreasen JO, Hasselgren G pH changes in dental tissues after root canal filling with calcium hydroxide. J Endod. 1981; 7:17-21 https://doi.org/10.1016/S0099-2399(81)80262-2
Massarstrom LE, Blömlof LB, Feiglin B, Lindskog SF Effect of calcium hydroxide treatment on periodontal repair and root resorption. Endod Dent Traumatol. 1986; 2:184-189 https://doi.org/10.1111/j.1600-9657.1986.tb00142.x
Cvek M Treatment of non-vital permanent incisors with calcium hydroxide. VI. A clinical, microbiological and radiological evaluation of treatment in one sitting of teeth with mature or immature root. Odontol Revy. 1976; 27:93-108
McGurkin-Smith R, Trope M, Caplan D, Sigurdsson A Reduction of intracanal bacteria using GT rotary instrumentation, 5.25% NaOCl, EDTA, and Ca(OH)2. J Endod. 2005; 31:359-363 https://doi.org/10.1097/01.don.0000145035.85272.7c
Nerwich A, Figdor D, Messer HH pH changes in root dentin over a 4-week period following root canal dressing with calcium hydroxide. J Endod. 1993; 19:302-306 https://doi.org/10.1016/S0099-2399(06)80461-9
Card SJ, Sigurdsson A, Ørstavik D, Trope M The effectiveness of increased apical enlargement in reducing intracanal bacteria. J Endod. 2002; 28:779-783 https://doi.org/10.1097/00004770-200211000-00008
Sundqvist G, Figdor D, Persson S, Sjogren U Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative retreatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 85:86-93 https://doi.org/10.1016/S1079-2104(98)90404-8
Ray HA, Trope M Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995; 28:12-18 https://doi.org/10.1111/j.1365-2591.1995.tb00150.x
Tronstad L, Asbjornsen K, Doving L Influence of coronal restorations on the peri-apical health of endodontically treated teeth. Endod Dent Traumatol. 2000; 16:218-221 https://doi.org/10.1034/j.1600-9657.2000.016005218.x
Cvek M Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. Endod Dent Traumatol. 1992; 8:45-55 https://doi.org/10.1111/j.1600-9657.1992.tb00228.x
Andreasen JO, Farik B, Munksgaard EC Long-term calcium hydroxide as a root canal may increase the risk of root fracture. Dent Traumatol. 2002; 18:134-137 https://doi.org/10.1034/j.1600-9657.2002.00097.x
Kahler SL, Shetty S, Andreasen FM, Kahler B The effect of long-term dressing with calcium hydroxide on the fracture susceptibility of teeth. J Endod. 2018; 44:464-459 https://doi.org/10.1016/j.joen.2017.09.018
Healing of peri-apical lesions with calcium hydroxide medicament following apical enlargement: a case study Thai Yeng Dental Update 2025 50:2, 101-105.
With public health orders restricting movement and changes to routine endodontic practice during the COVID-19 pandemic, many patients chose to wait, in the range of 12-18 months, before returning to complete their root canal treatment. This report describes several cases of non-vital and infected teeth that showed positive healing responses from having endodontic treatment using calcium hydroxide paste as an intracanal medicament and an apical enlargement technique to further reduce bacterial numbers. This indicates healing of peri-apical lesions may occur with a longer observation period.
CPD/Clinical Relevance: Endodontic treatment for peri-apical infection may allow a patient time to decide upon treatment options.
Article
Bacteria are essential for the development of apical periodontitis.1·2 Local factors, such as access to nutrients, positive and negative bacterial interactions, the redox potential and the host's defence system, influence the fate of bacteria that have entered the root canal space.3 In the management of apical periodontitis, the main antibacterial phase of endodontic treatment is attributed to chemomechanical instrumentation.4,5,6 Bacteria in areas such as isthmuses, ramifications, deltas, irregularities, and dentinal tubules may be unaffected by root canal treatment procedures.7,8
When root canal treatment is performed adequately, healing of the peri-apical lesion usually occurs, with gradual reduction and resolution of the radiolucency observed on subsequent examination.9,10 If an interappointment dressing is used, calcium hydroxide remains the best medicament available to inhibit the growth of intracanal bacteria before obturation.11 However, studies have shown that complete bacterial eradication is not achievable after chemomechanical debridement, even with the use of an intracanal medicament.11,12 Hence, further approaches need to be considered to maximize root canal disinfection.
With the emergence of COVID-19, a national human biosecurity emergency was declared across the country in March 2020, under Australia's Biosecurity Act 2015.13 Public health orders restricted gatherings and movement, and routine dental patient care practice changed, which generated significant challenges,14 and negatively affected patients’ willingness to seek dental treatment15 because of the fear of contracting COVID-19.
This study reports on the effectiveness of calcium hydroxide paste placement, following large apical size preparation, on the healing response of peri-apical lesions in permanent teeth in cases when a long period occurred before returning to the dentist to complete root canal therapy.
Case studies
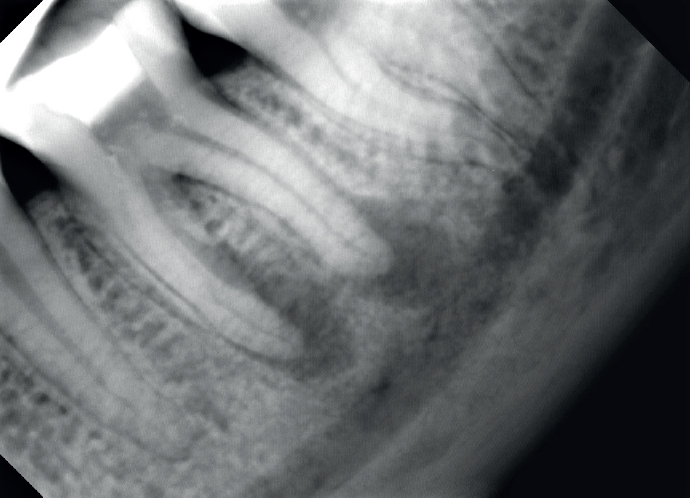
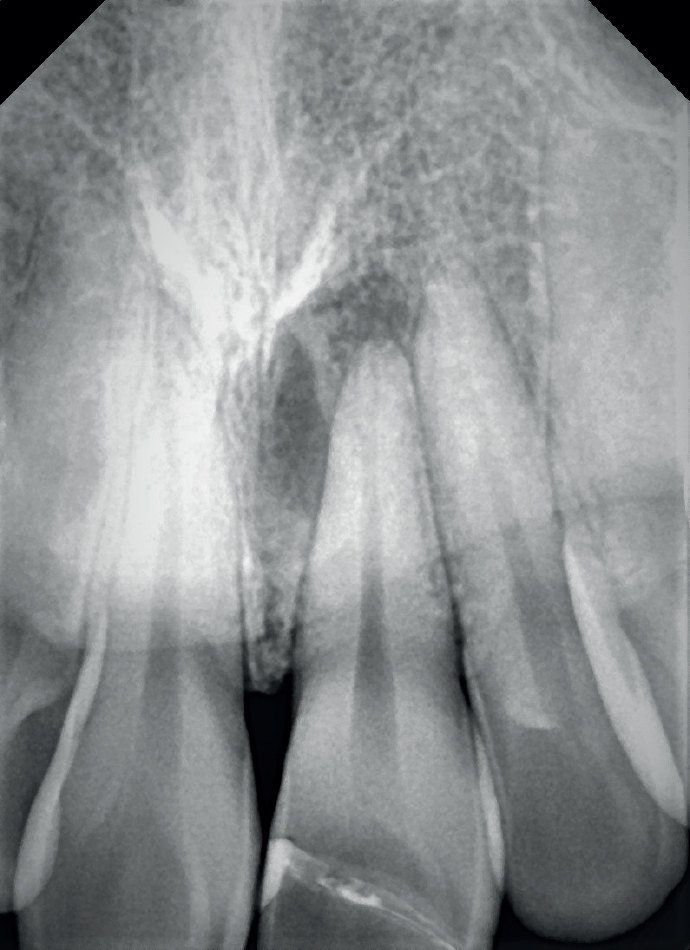
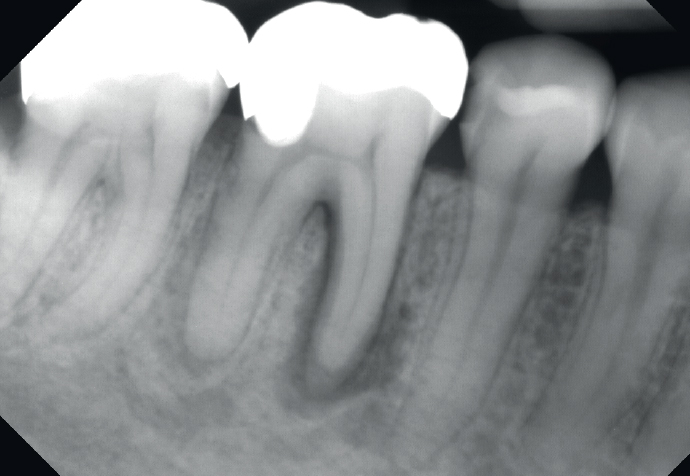
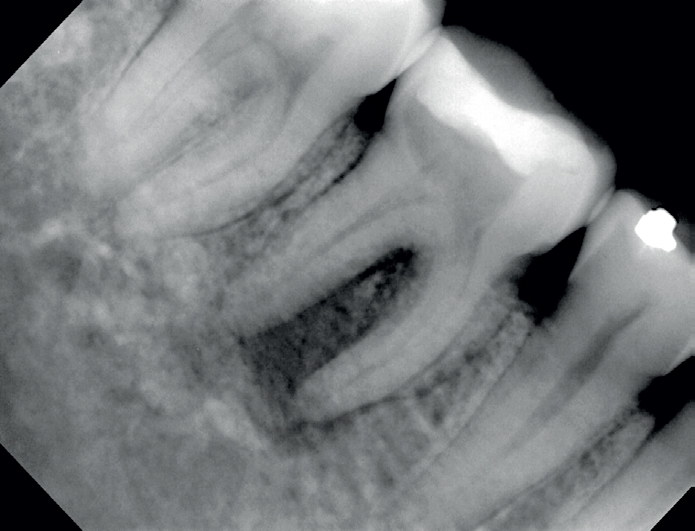
All five patients presented with a periapical radiolucency (Figures 1-5) and each was keen to have the tooth infection treated and avoid extraction.
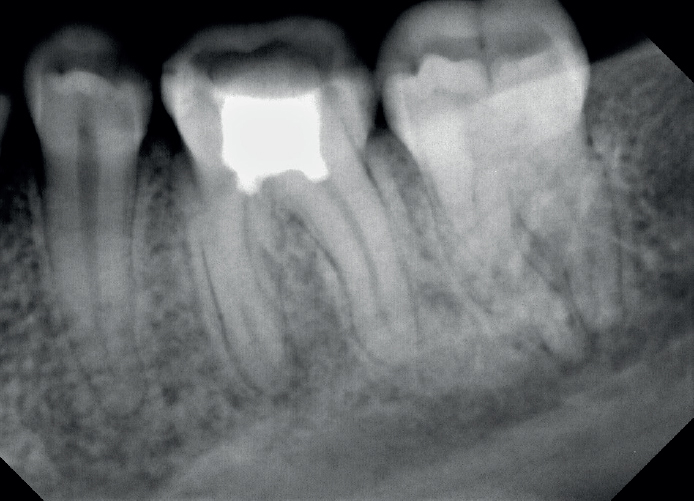
Figure 1.
Case 1. The lower left first mandibular molar (LL6) with a peri-apical lesion around the mesial and distal roots.Figure 2.
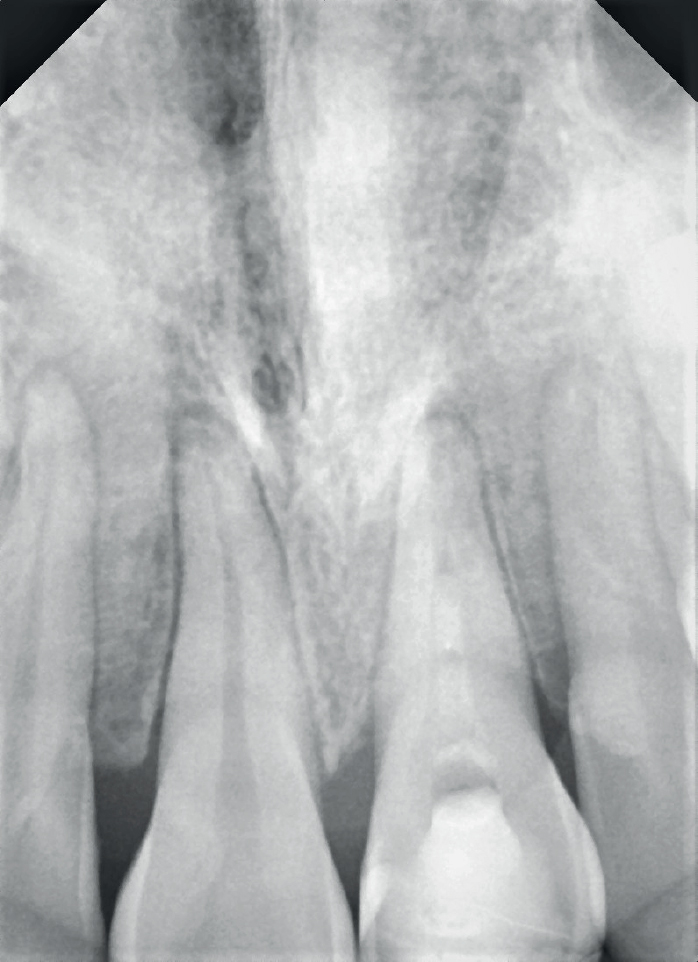
Case 2. A peri-apical lesion in the upper left central incisor (UL1).Figure 3.
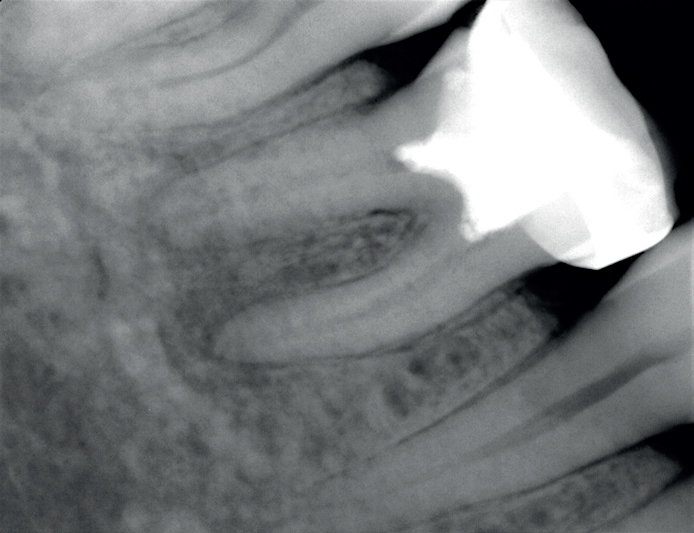
Case 3. The lower right first mandibular molar (LR6) with a peri-apical lesion seen around the mesial root.Figure 4.
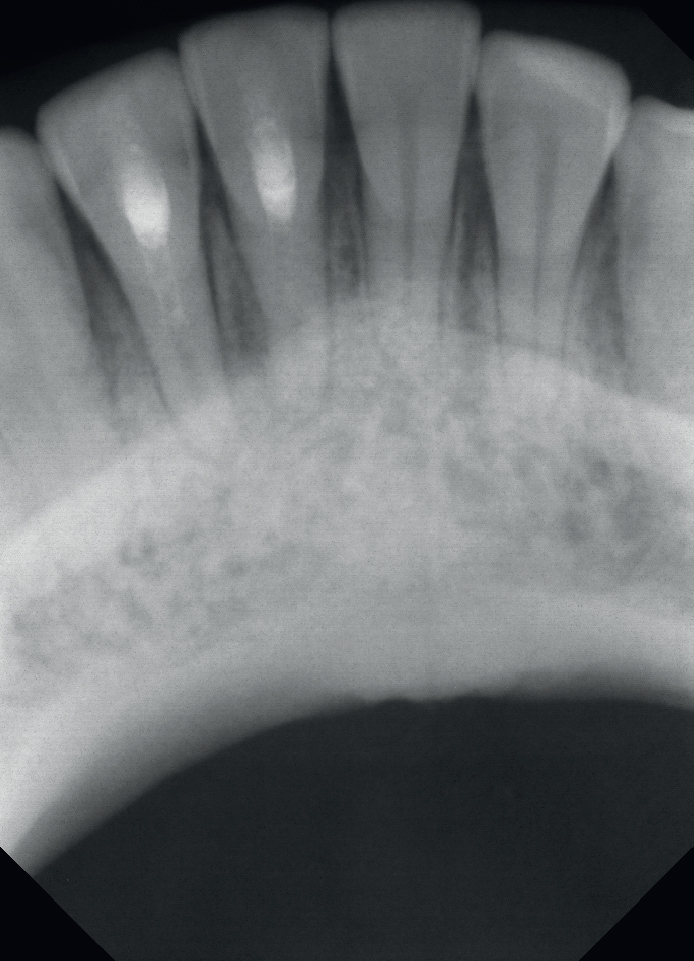
Case 4. The lower right central and lateral incisors (LR1 and LR2) with a peri-apical lesion around both teeth.Figure 5.
Case 5. The lower right first mandibular molar (LR6) with furcal bone loss and a periapical lesion extending from the mesial to the distal roots.
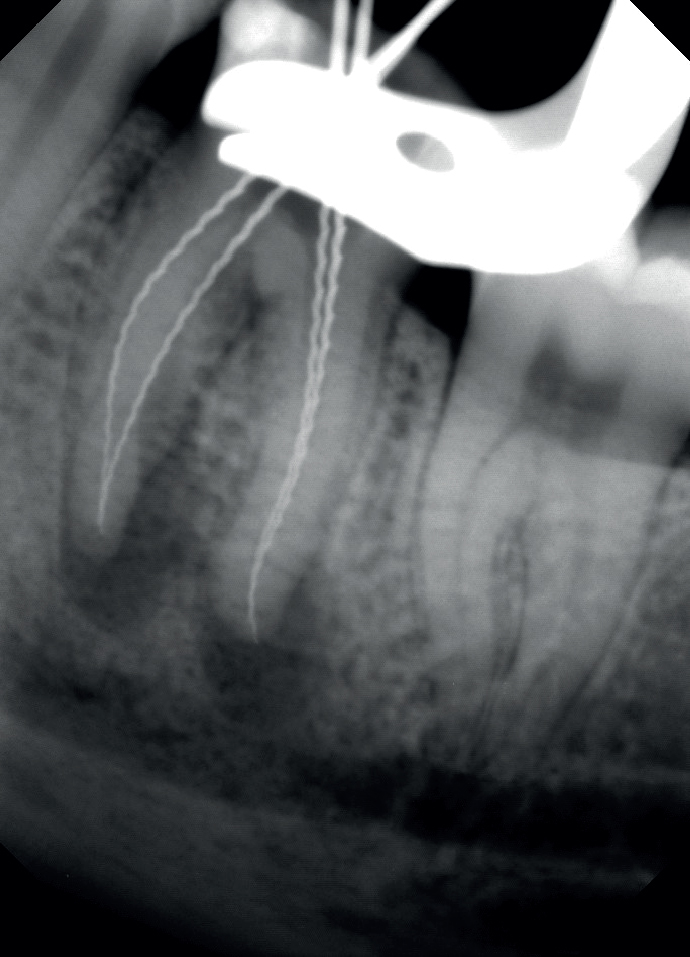
For all five cases, root canal treatment was initiated under rubber dam isolation. The canals were located with the aid of an operating microscope (Leica M320, Leica Microsystems, Singapore). Hedström files (ISO size 10) were then used to successfully negotiate the canals to the estimated working lengths. Working lengths were determined using an electronic apex locator (Tri Auto ZX, J Morita Corp, USA), and then verified with a peri-apical radiograph. A hybrid instrumentation technique involving the ProTaper and Vortex (Dentsply, Maillefer, Ballaigues, Switzerland) systems was employed. The molar canals were all instrumented to an apical size and taper of 40/.04 (Vortex) and F4 (Protaper) for anteriors (incisors). Copious irrigation with 4% sodium hypochlorite, along with ultrasonic irrigation (EndoActivator, Dentsply Sirona) and 17% ethylenediamine tetra-acetic acid (EDTA) were used throughout the instrumentation process. The canals were dressed with calcium hydroxide paste (Pulpdent Paste, Pulpdent Corp, Watertown, USA) using a rotary paste filler before the tooth was temporized with a double seal, consisting of Cavit and Fuji II LC (light-cured glass ionomer cement) (Figures 6-10).
Figure 6.
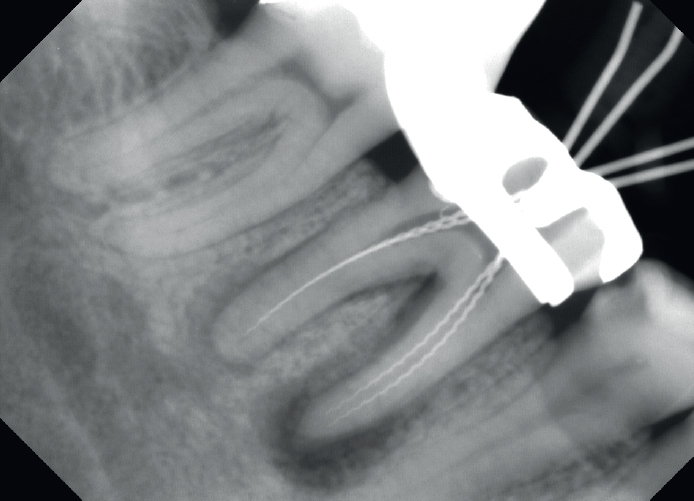
Case 1. Working length radiograph of LL6.Figure 7.
Case 2. Working length radiograph of UI1.Figure 8.
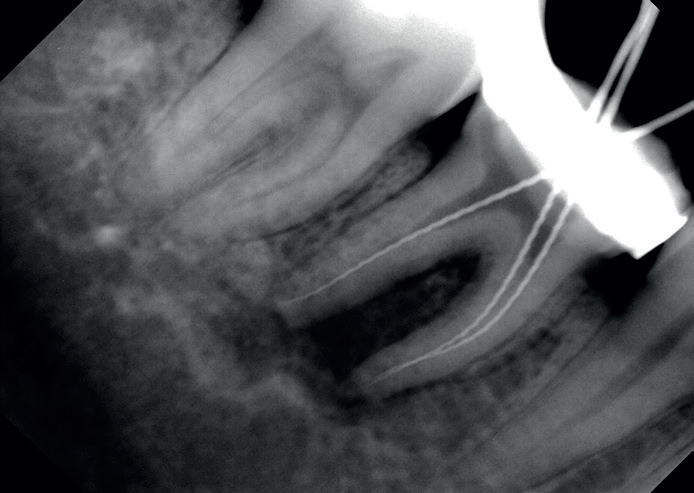
Case 3. Working length radiograph of LR6.Figure 9.
Case 4. Working length radiograph of LR1 and LR2.Figure 10.
Case 5. Working length radiograph of LL6.
The five patients returned between 12 and 18 months later, and all had radiographic healing evident. The teeth were clinically asymptomatic, with periodontal health within normal limits, no clinical evidence of coronal leakage, and a positive healing response was seen around the roots in the radiographs (Figures 11-15).
Figure 11.
Case 1. Healing response seen around LL6.Figure 12.
Case 2. Healing response seen around UL1.Figure 13.
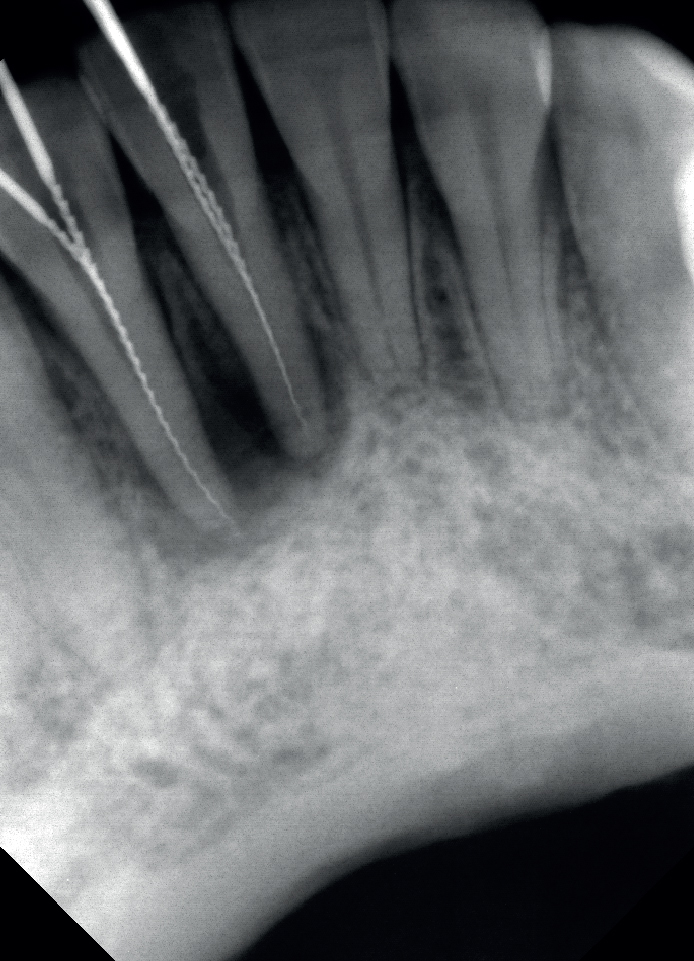
Case 3. Healing response seen around LR6.Figure 14.
Case 4. Healing response seen around LR1 and LR2.Figure 15.
Case 5. Healing response seen around LR6.
Discussion
When planning treatment for root canal treatment, the benefits of root canal treatment must be weighed against extraction of the tooth.1 During the COVID-19 pandemic, the enforced movement restrictions meant that many patients only sought dental care for emergency reasons. This meant that unusually long gaps occurred between a patient's initial root canal treatment and their follow up visit. This extended time between appointments suggests that positive healing responses can be seen with calcium hydroxide medicaments following apical enlargement of the root canals and highlights the importance of adequate temporary restorations being placed between appointments so as not to expose root canals to risks of coronal leakage and contribute to endodontic failure.
The apical foramen is one of the main routes of intercommunication between pulpal and periodontal tissues.2 Bacterial and inflammatory by-products may pass readily through the apical foramen to cause periapical pathosis and extend into the peri-apical tissues, causing a local inflammatory response with bone and root resorption.3 Lateral and accessory canals, mainly in the apical area and in the furcation of molars, also connect the dental pulp with the periodontal ligament.4 Gutmann5introduced safranin dye into 102 molar teeth placed in a vacuum chamber and found 28.4% of the teeth had furcation canals, although only 10.2% of the total group exhibited canals on the lateral root surface. The accessory canals contain connective tissue and vessels that connect the circulatory system of the pulp with that of the periodontium.17 Rubach and Mitchell21 found that serial sectioning of 74 teeth revealed that 45% showed accessory canals present primarily in the apical region. The presence of patent accessory canals provides further potential pathways for the spread of bacterial and toxic by-products, resulting in a direct inflammatory process in the periodontal ligament.17 Hence, any chemomechanical debridement and the antibacterial effects from the root canal medicament should aim to target bacteria in areas where pulpal and periodontal tissues communicate with each other.
As noted earlier, if an interappointment intracanal medicament is used, calcium hydroxide paste is recommended to maximize the reduction of intracanal bacteria before obturation,11 based on its antibacterial6,22 and anti-resorptive23,24 properties. The antibacterial activity of calcium hydroxide is probably due to its alkaline pH.6,22,25,26 The ability of calcium hydroxide to diffuse through exposed dentinal tubules to raise the pH at the root surface has been shown in vitro.23‘27 This suggests that the medicament can target invasive bacteria and their by-products which enter through the dentinal tubules, causing external destruction at the root surface void of cementum.
However, the anatomical complexity of the root canal may prevent high pH levels (∼12.5) reaching all parts of the canal, which may protect bacterial species from the antimicrobial effect of calcium hydroxide.28 To overcome this, the canals should be instrumented to relatively large apical sizes. Several studies support the concept that populations of intracanal bacteria decrease as apical enlargement increases,12,29,30,31 and this may contribute to a positive healing response. Placing calcium hydroxide medicaments following apical enlargement of the root canals will help to maximize root canal disinfection. Studies show that a combined approach of increasing the size of nickel-titanium (NiTi) rotary files, using sodium hypochlorite irrigant, and applying calcium hydroxide as an intracanal medicament significantly reduces the bacterial load from infected canals.12,26
Finally, and particularly in cases where the completion of the root canal therapy does not take place for a long time, a good interim restoration that minimizes any forms of coronal leakage is very important. Saunders and Saunders32 concluded that coronal leakage may contribute to the failure of good endodontic treatments by allowing micro-organisms to contaminate the root canals. An adequately placed coronal restoration may overcome some limitations of chemomechanical preparation by serving three important functions: block any communication between the oral cavity and the periradicular tissues; entomb any surviving bacterial cells in the root canal system containing medicament; and impede tissue fluid derived from the peri-apical tissues from reaching bacterial cells in the root canal to maintain their survival.33 It is important to know that inadequate temporary restorations, placed between appointments in multiple-visit endodontic treatments, may also expose root canals to risks of coronal leakage,34 and contribute to endodontic failure.35,36
A common concern among general dentists is that long-term dressing with calcium hydroxide may affect the fracture susceptibility of root canaltreated permanent teeth. Historically, long-term dressings with calcium hydroxide-based medicaments have been used in the treatment of immature teeth with open apices.37 In an animal study, Andresen et al38 reported fractures of immature teeth filled with calcium hydroxide medicament for an extended period. However, Kahler et al39 discovered that long-term calcium hydroxide dressing did not increase root fracture susceptibility; rather, the most important risk factor for root fracture may be the root development stage. Thus, an immature root presenting with a fragile, thin structure is more likely to be the primary causative factor. Hence, in these cases, long-term calcium hydroxide placement was not a predominant risk factor for causing root fracture.
Conclusion
In these case studies, the peri-apical lesions healed following a combination of apical enlargement and the application of a long-term calcium hydroxide medical dressing. In cases of chronic apical periodontitis, it may be worthwhile to attempt long-term medication after initiating root canal therapy if the patient is keen to ‘give it a go’ and to avoid losing the tooth.