Laukkanen E, Vehkalahti MM, Kotiranta AK. Impact of systemic diseases and tooth-based factors on outcome of root canal treatment. Int Endod J. 2019; 52:1417-1426 https://doi.org/10.1111/iej.13143
Winning L, Linden G. Periodontitis and systemic disease. BDJ Team. 2015; 2
Aminoshariae A, Kulild JC, Fouad AF. The impact of endodontic infections on the pathogenesis of cardiovascular disease(s): a systematic review with meta-analysis using GRADE. J Endod. 2018; 44:1361-1366.e3 https://doi.org/10.1016/j.joen.2018.06.011
Cotti E, Dessì C, Piras A Association of endodontic infection with detection of an initial lesion to the cardiovascular system. J Endod. 2011; 37:1624-1629 https://doi.org/10.1016/j.joen.2011.09.006
Wang CH, Chueh LH, Chen SC Impact of diabetes mellitus, hypertension, and coronary artery disease on tooth extraction after nonsurgical endodontic treatment. J Endod. 2011; 37:1-5 https://doi.org/10.1016/j.joen.2010.08.054
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011; 44:610-625 https://doi.org/10.1111/j.1365-2591.2011.01873.x
Liljestrand JM, Mäntylä P, Paju S Association of endodontic lesions with coronary artery disease. J Dent Res. 2016; 95:1358-1365 https://doi.org/10.1177/0022034516660509
Cotti E, Mercuro G. Apical periodontitis and cardiovascular diseases: previous findings and ongoing research. Int Endod J. 2015; 48:926-932 https://doi.org/10.1111/iej.12506
Hex N, Bartlett C, Wright D Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet Med. 2012; 29:855-862 https://doi.org/10.1111/j.1464-5491.2012.03698.x
López-López J, Jané-Salas E, Estrugo-Devesa A Periapical and endodontic status of type 2 diabetic patients in Catalonia, Spain: a cross-sectional study. J Endod. 2011; 37:598-601 https://doi.org/10.1016/j.joen.2011.01.002
Fouad AF, Burleson J. The effect of diabetes mellitus on endodontic treatment outcome: data from an electronic patient record. J Am Dent Assoc. 2003; 134:43-51 https://doi.org/10.14219/jada.archive.2003.0016
Britto LR, Katz J, Guelmann M, Heft M. Periradicular radiographic assessment in diabetic and control individuals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:449-452 https://doi.org/10.1016/s1079-2104(03)00034-9
Segura-Egea JJ, Martín-González J, Cabanillas-Balsera D Association between diabetes and the prevalence of radiolucent periapical lesions in root-filled teeth: systematic review and meta-analysis. Clin Oral Investig. 2016; 20:1133-1141 https://doi.org/10.1007/s00784-016-1805-4
Marotta PS, Fontes TV, Armada L Type 2 diabetes mellitus and the prevalence of apical periodontitis and endodontic treatment in an adult Brazilian population. J Endod. 2012; 38:297-300 https://doi.org/10.1016/j.joen.2011.11.001
Arya S, Duhan J, Tewari S Healing of apical periodontitis after nonsurgical treatment in patients with type 2 diabetes. J Endod. 2017; 43:1623-1627 https://doi.org/10.1016/j.joen.2017.05.013
Orstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986; 2:20-34 https://doi.org/10.1111/j.1600-9657.1986.tb00119.x
Oscar P, López A, Lizama A Radiographic characteristics in the periapical healing post endodontic treatment in patients of the Autonomous University of Yucatan, School of Dentistry. Nova Scientia. 2018; 10:379-390
Smadi L. Apical periodontitis and endodontic treatment in patients with type II diabetes mellitus: comparative cross-sectional survey. J Contem Dent Pract. 2017; 18:358-362
Alley BS, Buchanan TH, Eleazer PD. Comparison of the success of root canal therapy in HIV/AIDS patients and non-infected controls. Gen Dent. 2008; 56:155-157
Shetty K, Garcia J, Leigh J. Success of root canal therapy in HIV-positive patients. Gen Dent. 2006; 54:397-402
Drake MT, Clarke BL, Khosla S. Bisphosphonates: mechanism of action and role in clinical practice. Mayo Clin Proc. 2008; 83:1032-1045 https://doi.org/10.4065/83.9.1032
Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003; 61:1115-1117 https://doi.org/10.1016/s0278-2391(03)00720-1
Hsiao A, Glickman G, He J. A retrospective clinical and radiographic study on healing of periradicular lesions in patients taking oral bisphosphonates. J Endod. 2009; 35:1525-1528 https://doi.org/10.1016/j.joen.2009.07.020
Imura N, Pinheiro ET, Gomes BP The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007; 33:1278-1282 https://doi.org/10.1016/j.joen.2007.07.018
Interactions between systemic and oral diseases have been investigated in many contexts. This is a narrative review discussing the impact of several systemic diseases, including cardiovascular disease and diabetes mellitus, on non-surgical endodontic treatment outcomes. There is currently a lack of conclusive evidence to support links between systemic disease and endodontic outcomes. Further high-quality research is needed for systemic disease to be reliably considered a prognostic factor.
CPD/Clinical Relevance: If systemic disease is found to impact upon non-surgical endodontic treatment outcomes, dentists could learn essential information regarding the prognosis of endodontic treatment by looking at a patient's medical history.
Article
Endodontology is the study of disease, prevention and treatment of the dental pulp and peri-radicular regions, with the principle disease being apical periodontitis caused by infection.1 Diseases of pulpal origin can severely affect quality of life through physical and psychological discomfort.2 Endodontic treatment offers a solution to treat pulpal disease and avoid the loss of natural teeth.
Success rates for endodontic treatments are high; however, multiple factors can affect outcome, such as the presence or extent of peri-radicular disease, amount of remaining tooth structure and the treatment methods used.3 While some of these factors can be modified, the patient's medical history needs further consideration. A key question that has arisen is whether a patient's systemic disease can affect the success of endodontic treatment outcomes.4 The direct impact of systemic disease on endodontic treatment outcomes has not been conclusively determined and is currently not well understood.
Evidence from other oral conditions indicates that systemic disease can manifest in the mouth. Association between periodontitis and systemic diseases such as diabetes mellitus, Crohn's disease and thrombocytopenia are well established.5 There is emerging evidence to suggest an association between systemic disease and endodontic pathology.6
This article is a narrative review discussing the effects of systemic disease on non-surgical endodontic treatment outcomes. The World Health Organization (WHO) published a report on ageing and health in 2015, which listed the most common systemic conditions affecting the global population and included:7
Cardiovascular disease (CVD);
Diabetes mellitus;
Respiratory diseases;
Cancer;
Liver cirrhosis;
Osteoarthritis;
Conditions involving neurocognitive impairment, such as unipolar depression, Alzheimer's disease, and other dementias.
Using this list as guidance, this article reviews the systemic conditions outlined and the current evidence that suggests their association with endodontic treatment outcomes. Those which have an established association with endodontic outcome could be an important pre-operative prognostic factor to discuss in the consent process if found in the patient's medical history.
Cardiovascular disease
Cardiovascular disease (CVD) is a collective term for diseases of the heart and blood vessels. It includes coronary artery disease, such as angina and myocardial infarction, as well as other conditions such as heart failure, congenital heart disease and cardiomyopathy. CVDs are currently the number one cause of death globally.8 An estimated 17.9 million people died from CVD in 2016, representing 31% of all global deaths. In 2018, it was estimated around 7 million people in the UK are living with CVD, and this is the cause of 25% of deaths annually; one death every 3 minutes.9 The dominance of CVD as a major contributor to global mortality increases the importance in determining oral–systemic links. It is interesting to note that the disease process in CVD and endodontic infections share common inflammatory mediators, as shown by a reduction in mediators following successful endodontic treatment.10 A link between CVD and the success of endodontic treatment has been investigated in various studies, discussed hereafter.
Recurrence of infection and pain following unsuccessful treatment can lead to extraction, or secondary re-treatment with either the general dental practitioner or following a specialist referral.11 Wang et al12 proposed that there is an increased risk of tooth extraction following root canal treatment if the patient has coronary artery disease, hypertension, diabetes mellitus or a combination of these. Experiencing two or more diseases was a robust and significant indicator for an increased long-term risk of extraction following endodontic treatment. This could suggest that CVD predisposes an unsuccessful endodontic outcome. However, it is important to consider pain and persistent infection as prominent indicators for extraction, and factor this along with systemic disease involvement.
Ng et al13 conducted a prospective study, which set out to investigate factors influencing tooth loss following root canal treatment. Following annual follow-up of 2–4 years and a patient total of 1220, there were several prognostic factors affecting tooth survival after primary or secondary root canal treatment. Pre- and intra-operative factors that were found to negatively impact tooth survival included pain, deep periodontal probing depths and extrusion of root-filling material. Post-operative restorative factors for tooth loss included the type of coronal restoration and number of proximal contacts. Significant patient factors included a medical history of diabetes and systemic steroid therapy. These factors are categorized in Table 1. However, this study did not report a link between CVD and endodontic treatment outcomes.
General patient factors
Pre-operative factors
Intra-operative factors
Post-operative restorative factors
Diabetes
Steroid therapy
Thyroxine therapy
Pain
Sinus
Periodontal probing depth (PPD)
Presence of fractured instruments
Extrusion of root filling into the peri-apical tissue
Crown or root perforation
Blockage of any canal
Patency at canal terminus
Cast post and core
Type of coronal restoration
Number of proximal contacts
Terminal tooth
A cross-sectional study investigated whether endodontic lesions may be associated with an increased risk for coronary artery disease (CAD). A total of 14 508 patients with a mean age of 62 years was reported on. The cardiovascular outcomes included no significant CAD, stable CAD, and acute coronary syndrome (ACS); endodontic lesions in patients with peri-apical pathology were determined from panoramic tomography. Patients with CAD had an increased incidence of endodontic lesions. These findings support the hypothesis that endodontic lesions could be independently associated with CAD, particularly ACS. However, this link could be justified due to the association between poor oral health, endodontic infections and cardiovascular diseases.15 In summary, while some evidence links a medical history of CVD to treatment failure, a definitive link between CVD and endodontic outcomes has not been conclusively proven and further high-quality research is required to establish a link, should it exist.
Diabetes mellitus
Diabetes mellitus (DM) is defined as high blood sugar levels over a prolonged period, with symptoms including increased thirst and frequent urination. There is a well-established link between diabetes and periodontal disease. This has been reported as a bidirectional relationship; diabetes is a major risk factor for periodontal disease and periodontal disease has been shown to negatively impact glycaemic control.16 Globally, there was estimated to be 422 million people living with diabetes in 2014, compared to 108 million in 1980.17 The prevalence of this disease has been increasing over the last three decades, corresponding with the increase in obesity, a major risk factor for Type 2 diabetes. Diabetes and its complications bring substantial economic loss to people and healthcare systems alike. It is estimated that the NHS annual spending on diabetes will increase to 16.9 million by 2035, which would subsequently represent 17% of the total budget.18 The high prevalence and substantial effects generate interest in an oral–systemic connection.
A cross-sectional study investigated radiographic prevalence of apical periodontitis requiring endodontic treatment in a sample of 50 adult patients with well controlled Type 2 diabetes and 50 control patients.19 The results indicated that in adult patients, diabetes has a significant association with the prevalence of endodontic treatment due to infection. This study was primarily investigating whether diabetes is related to the pathogenesis of apical periodontitis, but the long-term survival of the endodontically treated teeth was not investigated. There have, however, been studies to compare healing outcomes following root canal therapy in diabetic and normoglycaemic patients to determine whether there is a correlation. One study investigated endodontic treatment outcomes in patients with and without diabetes, using an electronic record system.20 There was a 2-year follow-up post-operatively of 540 cases (including 73 cases in patients with diabetes), and it was concluded that patients with diabetes have a reduced likelihood of success of endodontic treatment in cases with pre-operative peri-radicular lesions.
Britto et al21 reported the prevalence of apical lesions in treated and untreated teeth in patients with diabetes, and a control group. The outcomes of interest were treated teeth with lesions, treated teeth without lesions and untreated teeth with lesions. Specifically, men with Type 2 diabetes who had endodontic treatment were more likely to have post-treatment lesions. From this it could be concluded that type 2 diabetes raises the probability of infection in the peri-radicular tissues following endodontic treatment. However, it would have been pertinent to consider that males have been shown to delay treatment compared to females and therefore often present with large chronic lesions, thereby increasing the likelihood of post-operative lesions. Similarly, a systematic analysis and meta-analysis was performed indicating similar results.22 Diabetic patients had a higher prevalence of apical periodontitis in endodontically treated teeth.
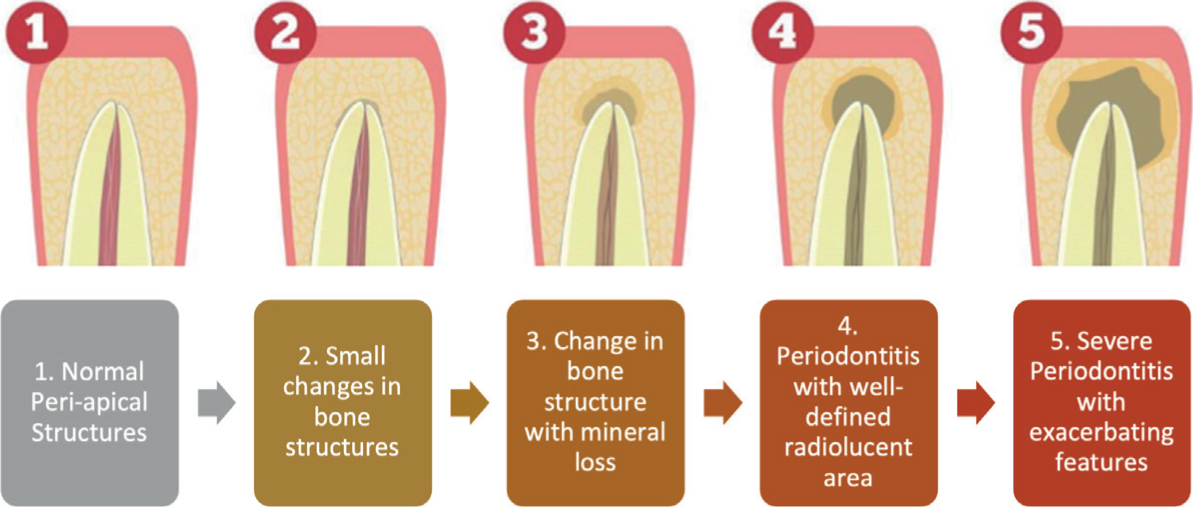
Accordingly, there have also been studies refuting the association of diabetes to endodontic outcome. A cross-sectional study showed no significant difference between patients with and without diabetes when the prevalence of apical periodontitis in root canal-treated teeth was evaluated.23 Furthermore, Arya et al24 observed that both the diabetic and non-diabetic groups showed a similar reduction in peri-apical score after endodontic treatment at the 12-month follow-up. The Periapical Index (PAI), developed by Orstavik in 1986, is a useful scoring system for registration of apical periodontitis in radiographs as shown in Figure 1.25 It provides an ordinal scale of 5, with scores ranging from 1 (healthy) to 5 (severe apical periodontitis).
Figure 1. A description of the Periapical Index (PAI) scoring method for registration of apical periodontitis in radiographs.2526
Using the WHO list of the most common systemic conditions affecting the global population, there are possible links between cardiovascular disease and diabetes mellitus. There was no evidence uncovered to link respiratory diseases, liver cirrhosis, osteoarthritis or conditions involving neurocognitive impairment and endodontic treatment outcomes. Further searching then revealed some evidence to support associations between:
HIV;
Bisphosphonates for pharmacological management of systemic disease.
Human immunodeficiency virus
HIV damages the cells in the immune system and leads to the life-threatening condition, AIDS. There have been ongoing discussions as to whether patients living with HIV are candidates for endodontic treatment and whether standard procedure should be followed due to HIV status.27
A retrospective study was conducted to compare peri-radicular healing 1 year following endodontic treatment in patients living with or without HIV.28 The PAI scoring method was used to score pre-and post-operative radiographs. There was no significant difference between the groups with regards to healing. Alley et al29 conducted a similar study to compare the success of root canal therapy in HIV/AIDs patients and non-infected controls. Two cohorts, with 50 teeth each, were sampled and a retrospective chart review conducted, which suggested there was no statistical difference in endodontic success.
Another study evaluated the success of therapy in 157 patients living with HIV, defining the parameters of success as post-operative absence of pain and swelling, as well as the absence of a peri-apical lesion (or a reduction in size compared to its pre-operative radiographic size).30 Following 6 months, the success rate in patients living with HIV was deemed to be approximately 90%, based on the predefined success criteria. However, a follow-up of only 6 months is too short to accept this as a reliable result. There was no difference in endodontic success between patients with respect to antiretroviral medication or symptomatic clinical presentation.
These studies would suggest clinicians do not need to anticipate poor healing or outcome on the grounds of HIV status alone and that HIV does not influence endodontic outcomes.
Pharmacological management of systemic disease and its effect on endodontic outcomes
In recent years, the dental profession has become much more aware of the effects of systemic drugs on dental treatment, none more so than oral and intravenous bisphosphonates. Bisphosphonates are a class of drug that prevent the loss of bone density. Primarily, they are first-line treatment for osteoporosis, but are also used to treat diseases such as Paget's disease, osteogenesis imperfecta, hypercalcaemia and cancer.31 Bisphosphonates are classed as anti-resorptive medications and are widely prescribed for a range of conditions.
The use of bisphosphonates has implications for dental practice because of the risk of medication-related osteonecrosis of the jaw (MRONJ).32 Criteria for diagnosis include current or previous treatment with anti-resorptive medication, exposed bone persisting for more than 8 weeks and no other history of radiotherapy or obvious metastatic disease of the bone. The initiating factor is often extraction leading to bone exposure, failure to heal and subsequent necrosis. Oral bisphosphonates are approved for treatment of osteoporosis and other conditions whereas intravenous (IV) bisphosphonates are used to manage cancer and cancer-related conditions, such as hypercalcaemia of malignancy (HCM). These are administered in high dose infusions, annually or quarterly, depending on the medication. It is noted that the risk of MRONJ is substantially greater in patients receiving IV bisphosphonates in the treatment of cancer.33
There has been some research conducted to investigate the effect of the drug class bisphosphonates on endodontic outcomes. One retrospective study evaluated and reported on the long-term healing of peri-radicular lesions following endodontic treatment in patients taking bisphosphonate therapy.34 The aim was to see whether bisphosphonate therapy had an impact on healing and, consequently endodontic outcomes, over a period of 7 years. There was no statistical difference between the bisphosphonate group and the control group to suggest either a positive or negative effect of drug use on outcome. While the quality of this evidence is moderate, more research is required to deem any significant association. Root canal treatment is preferable to extraction, when possible, in patients at risk of MRONJ. As such, it is relevant to consider whether there is an association between bisphosphonate therapy and endodontic treatment outcomes.
Considerations
An important factor to consider when assessing the evidence base for correlations between systemic disease and endodontic outcomes is the pre-operative status of the pulp. While some did take this factor into consideration, most studies did not differentiate between cases with a vital pulp and cases with pre-operative pulpal pathology.16,21 The presence of a pre-operative lesion is worth considering for endodontic prognosis. The presence of pre-operative apical periodontitis may negatively impact on outcome of non-surgical root canal treatment leading to a small reduction in success rate.35 A vital pulp that is extirpated may not have the same demands on the immune system to facilitate healing. Alternatively, cases with a pre-operative peri-apical radiolucency tend to have poorer prognosis and this may be down to the host response modulated by systemic disease. Future studies should aim to distinguish between cases with and without a pre-operative peri-apical radiolucency to allow for more precise and rigorous results.
There are many factors involved in determining endodontic success. Ng et al16 categorized the main factors into general patient factors, pre-operative, intra-operative and restorative considerations (Table 1). Other common factors include inadequate cleaning or filing of canals, improper coronal seal, iatrogenic procedural knowledge, and presence of bacteria, which are highlighted in Table 2.36 Dentists should carefully consider all of these during treatment. The restorability of a tooth is key; never embark on endodontic treatment without certainty of restorability. As it stands currently, the factors mentioned in Tables 1 and 2 have the greatest effect on non-surgical endodontic treatment outcomes than any possible effect due to systemic disease.
▪ Inadequate cleaning or filing of canals
▪ Improper coronal seal
▪ Iatrogenic procedural knowledge
▪ Persistence of bacteria
▪ Complications of instrumentation
▪ Inadequate or overextended root filling
Conclusions
This review discussed evidence to support a link between systemic disease and non-surgical endodontic treatment outcomes, which is summarized in Table 3. There is currently no available evidence to link respiratory diseases, cancer, liver cirrhosis, osteoarthritis or conditions involving neurocognitive impairment. Based on the research conducted:
Cardiovascular disease and diabetes mellitus may influence endodontic outcomes. However, the available evidence is of poor quality and further high-quality research is required.
HIV status and the use of bisphosphonates appear to have no association with endodontic outcomes. However, further high-quality research is needed in this area.
Cardiovascular disease (CVD)
CVD may be associated with non-surgical endodontic treatment outcomes
Diabetes mellitus
Diabetes mellitus may be associated with non-surgical endodontic treatment outcomes
HIV
There is no association between HV positive status and non-surgical endodontic treatment outcomes
Pharmacological management of systemic disease
There is no association between the use of bisphosphonates and non-surgical endodontic treatment outcomes
There was no available evidence to link endodontic outcomes with respiratory disease, cancer, liver cirrhosis, osteoarthritis or conditions involving cognitive impairment
Further high-quality research is necessary to confirm any systemic disease association
Overall, the evidence to support the effects of systemic disease on endodontic outcomes is still inconclusive, and this area of research requires further attention. It cannot be stated with certainty whether a correlation exists. While there appears to be an association with two diseases, CVD and diabetes mellitus, more robust evidence is necessary for systemic disease to be reliably considered a prognostic factor. To address this question in the future, longitudinal studies over a substantial time are needed to determine whether systemic disease has any influence on endodontic healing outcomes.