Danin J, Linder LE, Lundqvist G, Ohlsson L, Ramskold LO, Stromberg T. Outcomes of periradicular surgery in cases with apical pathosis and untreated canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:227-232
Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal therapy: a review. Dental Traumatol. 1994; 10:105-108
London: RCS Eng; 2001
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006; 39:921-930
London: GDC Standards Guidance; 2005
Bahcall JK, Olsen EK. Integrating ultrasonic tips into the endodontic treatment armamentarium. Dent Today. 2007; 26:120-123
Tzanetakis GN, Lagoudakos TA, Kontakiotis EG. Endodontic treatment of a mandibular second premolar with four canals using operating microscope. J Endod. 2007; 33:318-321
Passarinho-Neto JG, Marchesan MA, Ferreira RB, Silva RG, Silva-Sousa YT, Sousa-Neto MD. In vitro evaluation of endodontic debris removal as obtained by rotary instrumentation coupled with ultrasonic irrigation. Aust Endod J. 2006; 32:123-128
Smadi L, Khraisat A. Detection of a second mesiobuccal canal in the mesiobuccal roots of maxillary first molar teeth. Oral Surg Oral Med Oral Path Oral Rad Endod. 2007; 103:e77-81
Yoshioka T, Kikuchi I, Fukumoto Y, Kobayashi C, Suda H. Detection of the second mesiobuccal canal in mesiobuccal roots of maxillary molar teeth ex vivo. Int Endod J. 2005; 38:124-128
Kvist T, Reit C, Esposito M, Mileman P, Bianchi S, Petterson K, Andersson C. Prescribing endodontic retreatment: towards a theory of dentist behavior. Int Endod J. 1994; 27:285-290
Kvist T, Reit C. Postoperative discomfort associated with surgical and nonsurgical endodontic retreatment. Dent Traumatol. 2000; 16:71-74
Kvist T, Reit C. Results of endodontic retreatment: a randomized clinical study comparing surgical and nonsurgical procedures. J Endod. 1999; 25:814-817
Torabinejad M, Corr R, Handysides R, Shabahang R. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009; 35:930-937
Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998; 85:86-93
Bergenholtz G, Lekholm U, Milthon R, Heden G, Ödesjö B, Engström B. Retreatment of endodontic fillings. Eur J Oral Sci. 1979; 87:217-224
Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006; 32:601-623
Arx TV. Failed root canals: the case for Apicoectomy (periradicular surgery). J Oral Maxillofacial Surg. 2005; 63:832-837
Wong R. Conventional endodontic failure and retreatment. Dent Clin North Am. 2004; 48:265-289
Peri-radicular surgery is a valuable treatment modality allowing thorough treatment of chronic infection of the peri-radicular tissues. It is important that this treatment option is prescribed appropriately and steps are taken to help improve outcomes of surgery. We discuss the indications for peri-radicular surgery, considerations when planning treatment for teeth where orthograde endodontics has failed and present the findings of an audit into the appropriateness of referrals for peri-radicular surgery to the Department of Oral and Maxillofacial Surgery at a District General Hospital.
Clinical Relevance: This article highlights the indications and contra-indications for peri-radicular surgery to general dental practitioners.
Article
Peri-radicular surgery involves the access and visualization of peri-radicular tissues including the root apex, alveolar bone and any associated chronic apical granulomatous tissue. The technique allows for removal of the root apex along with the terminal (apical) plexus of root canal anatomy, thorough curettage of the apical tissues and retrograde endodontic obturation. Peri-radicular surgery is often carried out when conventional root canal treatment has failed. Such failure may be the result of inadequate disinfection of the root canal system or subsequent re-infection due to breakdown of coronal restoration seal. Where endodontic obturation is short of the apex or poorly condensed, non-surgical orthograde re-treatment may provide an opportunity to remove necrotic tissue and disinfect the root canal system more thoroughly than surgical treatment, and there is evidence to suggest that a poor coronal seal is one of the main reasons for failure of root canal treatment.1,2 Detailed description of the technique is outside the scope of this paper.
Multiple considerations need to be taken into account when treatment planning for teeth where conventional orthograde endodontic treatment has failed. The indications for peri-radicular surgery and considerations which should be made when deciding on re-treatment of failed endodontically treated teeth are discussed and the findings of an audit of referrals to the Department of Oral and Maxillofacial Surgery at a District General Hospital are presented.
Indications for peri-radicular surgery
Peri-radicular surgery is indicated in situations when repeat orthograde endodontic treatment is not possible or may put a tooth at risk of irreparable damage. In 2001, The Royal College of Surgeons of England (RCS Eng) published guidelines for the appropriate indications for surgical endodontics which include:3
Peri-radicular disease in a root-filled tooth, where non-surgical endodontic re-treatment cannot be undertaken or where conventional re-treatment might risk the restorability of the tooth, eg sclerotic root canals and teeth with full coverage restorations where conventional access may jeopardize the root.
Peri-radicular disease in a tooth where iatrogenic or developmental anomalies prevent non-surgical root canal treatment being undertaken, eg irretrievable fractured instruments.
Where a biopsy of peri-radicular tissue is required.
Where visualization of the peri-radicular tissues and tooth root is required when perforation, root crack or fracture is suspected.
Where procedures are required that require either tooth sectioning or root amputation.
Where it may not be expedient to undertake prolonged non-surgical root canal re-treatment because of patient considerations.
It must be stressed that these are guidelines and each clinical situation must be assessed on its own merits. It is also important to note that in some clinical situations where, according to the RCS Eng guidelines, peri-radicular surgery may be indicated, more conservative measures are available. Examples include the treatment of teeth with sclerotic root canals by conventional root treatment, or bypassing fractured instruments in a canal with the aid of magnification, and the removal of posts with ultrasonic endodontic instrumentation. These options may not be widely available in general practice, however, they should be considered when discussing treatment options and considering referral of patients.
The European Society of Endodontology has published more recent guidelines on the appropriate indications for peri-radicular surgery which include:4
Radiographic evidence of apical periodontitis and/or root canal obstruction (which has proved not to be negotiable and where further attempts to bypass the obstruction will risk damage to the tooth).
Extruded material with clinical or radiological findings of apical periodontitis and/or symptoms continuing over a prolonged period.
Persisting or emerging disease following root canal treatment when root canal re-treatment is inappropriate.
Perforation of the root or the floor of the pulp chamber and where it is impossible to treat from within the pulp cavity.
Considerations for failed endodontic treatment
In order for consent to be valid, the patient should be aware of the availability of other forms of treatment, their risks and benefits, and whether or not you consider the treatment is appropriate’.5 Referral to specialist endodontic services is an option when presented with a failed root canal treatment, and should be discussed with patients. With improvements in magnification and use of ultrasonic endodontic instrumentation, historic barriers to successful endodontics, such as canal obstruction by sclerotic dentine or debris, difficulties in locating all canals and presence of post-and-core crown restorations, etc may be overcome.6–10
The decision of when to re-treat a tooth that has undergone root canal therapy is a difficult one. If we assume that, as described by Kvist et al, there is a continuum of health states between peri-apical health to peri-apical disease, the decision at which point on that scale dentists and patients would opt for re-treatment is largely subjective and depends on a number of variable factors such as cost, strategic value of the tooth, experience of symptoms by the patient, etc.11 As a result of this, it is useful for clinicians to use accepted definitions of success from societies such as the European Society of Endodontology. In their consensus report for quality guidelines in endodontic treatment definitions of endodontic outcome are divided into favourable, uncertain and unfavourable.4 Favourable outcomes are indicated by:
Absence of pain, swelling and other symptoms;
No sinus tract;
No loss of function; and
Radiographic appearance of a normal periodontal ligament space around the root.
Uncertainty of outcome is categorized by a persistence or reduction in the size of any peri-apical radiographic lesion. Persistence of the lesion after four years would tend to suggest the presence of peri-apical disease. An unfavourable outcome, with the implication therefore that re-treatment is needed, would be indicated by:
Signs of pain or other signs and symptoms;
Presence of a radiological lesion when there was none pre-treatment or increase in size of a pre-treatment radiological lesion;
Persistence of a radiological lesion at the same size or only slight reduction in size compared to pre-treatment when assessed after 4 years;
Signs of continuing root resorption.
An exception to this list would be where a particularly large radiological lesion has significantly reduced in size but has left an irregularly mineralized area which may indicate scar tissue formation rather than a persistent apical disease. Here one should continue to assess the lesion.
Which treatment method has higher rates of long-term success, surgical or non-surgical endodontics? Again the answer depends upon the definition of success and, like the decision when to re-treat, may be considered subjective. The evidence to answer this question is, so far, inconclusive, and evaluation of research is complicated by various definitions of what success/failure used in trials.
In terms of post-operative discomfort and indirect costs to treatment, Kvist et al used a 100 mm Visual Analogue Scale (VAS) to assess the incidence of post-operative pain and swelling during the first week after treatment for 95 patients randomly assigned to either surgical or non-surgical endodontic treatment. Patients who underwent surgical treatment showed higher levels of pain and swelling, were more likely to consume analgesics and were more likely to miss work due to swelling or discoloration to the skin.12
Kvist et al reported a randomized clinical study comparing surgical with non-surgical treatment on 95 teeth randomly assigned to either surgical or non-surgical re-treatment and followed up for a period of 4 years. After 12 months they found that the group treated surgically demonstrated a statistically significant higher healing rate, though after 48 months this difference was no longer seen, perhaps owing to slower healing in the non-surgical group or ‘late failures’ in the surgical group. They were unable to demonstrate any systematic differences in outcomes, though their results suggested that surgical treatment may be associated with a higher risk of ‘late failures’.13
Torabinejad et al carried out a systematic review with robust methodology looking at outcomes of non-surgical retreatment and endodontic surgery. They found that, for follow-up periods of between two and four years, teeth treated surgically have a significantly higher success rate (77.8%) than those treated non-surgically (70.9%). For follow-up between four to six years, however, this relationship was reversed, with statistically significant higher rates of success for non-surgically re-treated teeth (83%) compared to teeth treated with surgery (71.8%).14
Each clinician must make judgements based upon the clinical situation before them. One may evaluate the quality of previous root canal treatment based upon radiographic assessment of the obturation and clinical/radiographic assessment of the coronal restoration. For teeth that one might evaluate as having technical deficiencies, some research evidence would suggest very favourable outcomes from non-surgical re-treatment. Sundqvist et al were able to demonstrate success rates of up to 74% for conventional re-treatment cases followed for five years.15 Bergenholtz et al demonstrated success rates of up to 94% for teeth re-treated owing to technical inadequacies alone when followed for two years.16
Clinical audit
Methods and materials
Data were gathered prospectively over six months using a data collection sheet completed by the consulting clinician. Appropriateness criteria were developed using guidance from The Royal College of Surgeons of England, The European Society of Endodontology, departmental referral criteria and a literature search of relevant, peer reviewed, published papers.1–4,6–19 For the purpose of the audit, appropriate referrals included teeth with a satisfactory, conventional root canal filling. Acceptable reasons for referral included presence of a complicating factor such as:
Extruded material beyond the apex of the root;
Separated instruments;
Suspected root fracture or perforation;
Large apical cyst (that required the use of extra-oral radiographic imaging to see its full extent).
The presence of a post alone was not seen as a valid enough reason not to repeat orthograde non-surgical endodontics owing to techniques and instruments being available to overcome this problem. Some of the above criteria for appropriateness are subjective (ie instrument separation and material extrusion) and could be overcome using appropriate instrumentation and magnification by a clinician with a special interest in endodontics, however, as referrals were being made by general practitioners in primary care, it was felt that referral would be appropriate even if only for a second opinion for such cases.
Referrals were deemed inappropriate if teeth had no initial root canal treatment and, despite none of the complicating factors mentioned above being present, conventional re-treatment had not been attempted by the referring dentist (Table 1). We deemed 95% of appropriate as an acceptable gold standard.
Criteria for inappropriate referral
How was this measured?
Poor coronal seal
Deficiency at the crown margin (measured with a sharp probe)History of crown de-cementation
Poor lateral condensation
Visible deficiency on radiographic examination
No initial root canal filling (RCF)
Absence of conventional root canal filling material on radiographic examination
Short obturation
Root canal filling material >2 mm short of the radiographic apex
Results
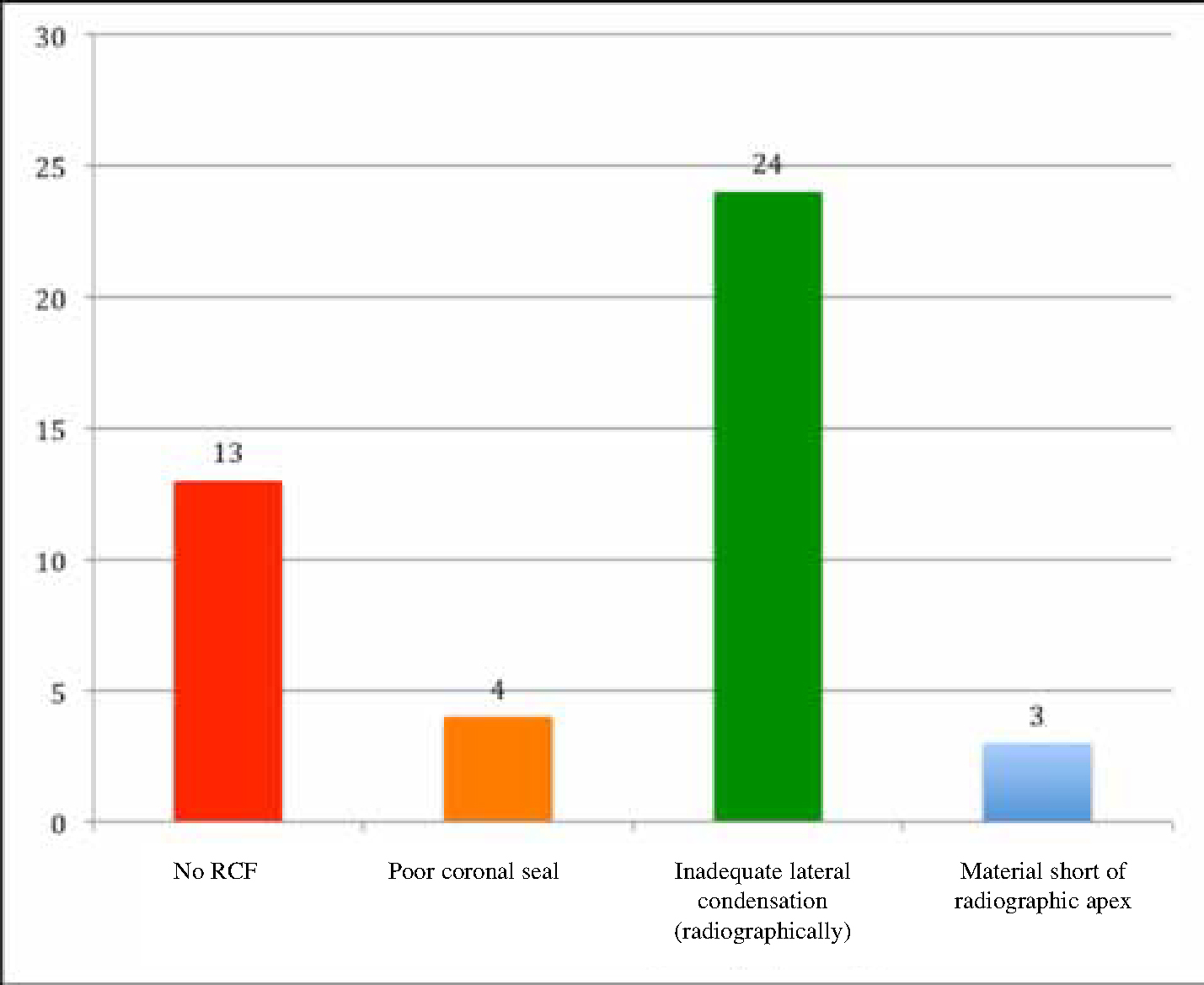
Over a six-month period, 49 patients (25 females and 24 males), 68 teeth in total were eligible for inclusion in the audit. Of the 68 teeth (19%), 13 had no conventional root canal filling (this included absence of conventional root-filling material apical to an intra-radicular post) and two teeth had not even undergone endodontic access. A total of 44 (65%) teeth were referred inappropriately according to criteria set out in Table 1. Reasons for referrals being deemed inappropriate included:
No radiographic conventional root canal filling (n = 13);
Inadequate lateral condensation on radiographic inspection (n = 24);
Root canal filling material more than 2 mm short of the radiographic apex (n = 3); and
Figure 1. Reasons for referrals being deemed inappropriate.
Conventional orthograde repeat endodontics had been attempted on only three teeth (5%).
Discussion
The authors accept that the relatively small number of teeth included in the audit and the limitations of the methodology in only providing cross-sectional observational data, and the use of subjective outcome measures, prevents making any sweeping conclusions. However, 19% of teeth had not undergone initial conventional root canal treatment, two teeth had not undergone endodontic access and only 5% of teeth were non-surgically re-treated before referral. These figures fell short of the gold standard set in the audit. It is impossible, from this audit, to deduce the reasons for so few teeth undergoing repeat endodontic treatment before referral. However, limited remuneration on the NHS for a time consuming treatment may be a factor.
Conclusions
This audit has demonstrated, within the limitations of the methodology, that referrals for peri-radicular surgery to our department were not all entirely appropriate. The authors considered that some were indeed inappropriate. The decision to re-treat teeth endodontically, either surgically or non-surgically, is a difficult one. Where teeth have deficient coronal restoration margins, or technical deficiencies are evident on radiographic examination, conventional non-surgical re-treatment should be discussed with patients as a valid alternative to surgery. Peri-radicular surgery should not be considered as a fallback position following poor quality orthograde root canal treatment procedures, such as inadequate isolation and irrigation techniques, treatment short of the root apex and deficient seal of coronal restorations. Where technical failings in initial treatment such as these can be demonstrated, efforts to rectify the situation by non-surgical re-treatment should be made before considering surgery.
Further randomized controlled clinical trial research to compare non-surgical and surgical endodontic treatment success rates over longer follow-up periods would help clinicians and patients to make these difficult decisions.