Burns LE, Kim J, Wu Y Outcomes of primary root canal therapy: an updated systematic review of longitudinal clinical studies published between 2003 and 2020. Int Endod J. 2022; 55:714-731 https://doi.org/10.1111/iej.13736
Kakehashi S, Stanley HR, Fitzgerald RJ The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965; 20:340-349 https://doi.org/10.1016/0030-4220(65)90166-0
Krmpotic M, Macan D, Skrlin J, Peric B A microbiological study of periapical lesions in single rooted teeth with open and closed root canal. Int J of Oral Sci and Dent Med. 2002; 36:375-379
Segura-Egea JJ, Cabanillas-Balsera D, Martín-González J, Cintra LTA Impact of systemic health on treatment outcomes in endodontics. Int Endod J. 2023; 56:219-235 https://doi.org/10.1111/iej.13789
Ng YL, Mann V, Rahbaran S Outcome of primary root canal treatment: a systematic review of the literature – Part 2. Influence of clinical factors. Int Endod J. 2008; 41:6-31 https://doi.org/10.1111/j.1365-2591.2007.01323.x
Dawood A, Patel S The Dental Practicality Index – assessing the restorability of teeth. Br Dent J. 2017; 222:755-758 https://doi.org/10.1038/sj.bdj.2017.447
Ordinola-Zapata R, Noblett WC, Perez-Ron A Present status and future directions of intracanal medicaments. Int Endod J. 2022; 55:613-636 https://doi.org/10.1111/iej.13731
Lin PY, Huang SH, Chang HJ, Chi LY The effect of rubber dam usage on the survival rate of teeth receiving initial root canal treatment: a nationwide population-based study. J Endod. 2014; 40:1733-1737 https://doi.org/10.1016/j.joen.2014.07.007
Richardson N, Mordan NJ, Figueiredo JA Microflora in teeth associated with apical periodontitis: a methodological observational study comparing two protocols and three microscopy techniques. Int Endod J. 2009; 42:908-921 https://doi.org/10.1111/j.1365-2591.2009.01594.x
Ordinola-Zapata R, Noblett WC, Perez-Ron A Present status and future directions of intracanal medicaments. Int Endod J. 2022; 55:613-636 https://doi.org/10.1111/iej.13731
Mergoni G, Ganim M, Lodi G Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2022; 12 https://doi.org/10.1002/14651858.CD005296.pub4
Yen C, Pawar K Significance of apical patency in endodontics: a narrative review. Dentistry. 2021; 11
Ajina M, Billis G, Chong BS The effect of glide path preparation on root canal shaping procedures and outcomes. Eur Endod J. 2022; 7:92-105 https://doi.org/10.14744/eej.2022.97659
Management of Persistently Symptomatic Teeth in Primary Root Canal Treatment: Advice on Maximizing Successful Outcomes Menna Shykhon David Green Philip Lumley Dental Update 2025 51:11, 756-765.
The aim of root canal treatment is chemo-mechanical debridement of the root canal system to promote healing. Root canal treatment is a predictable modality in the treatment of apical periodontitis; however, there are situations during primary root canal treatment where signs and symptoms persist despite repeated chemo-mechanical disinfection. This article highlights such situations and offers practical solutions on how to minimize them.
CPD/Clinical Relevance:
Understanding the possible causes of a persistently symptomatic tooth during treatment may allow for appropriate management.
Article
The aim of root canal treatment is chemo-mechanical debridement of the root canal system to promote apical healing. Root canal treatment has key sequential clinical stages, commencing by accessing the root canal system to locate the canals, while also ensuring all pulpal tissue is removed. The root canal is subsequently instrumented and shaped, with a variety of instruments including hand-files and rotary nickel–titanium (NiTi) files. Mechanical shaping of the root canal facilitates irrigation towards the apical region of the canals, while also allowing for more controlled and efficient obturation.1 Chemical disinfection with irrigants such as sodium hypochlorite may allow the microbial load to be reduced, facilitating the healing process and aiming to prevent further re-infection.2 The complete process of chemo-mechanical disinfection can be performed in a single visit, or over multiple visits, with placement of an intra-canal medicament between appointments.
Although primary root canal treatment is a predictable treatment modality for the management of endodontic lesions, with a success rate of up to 93%, it is often time consuming for general dental practitioners and it can be frustrating when symptoms fail to resolve despite repeated disinfection.3 Therefore, understanding the possible causes of persistently symptomatic teeth can aid clinicians in using effective and efficient clinical techniques to reduce the incidence of persistently symptomatic teeth and maximize successful outcomes.
Microbiology
Understanding the aetiology of endodontic disease allows us to appreciate the aims of root canal treatment. Kakehashi et al undertook an experimental study, concluding that apical periodontitis did not develop in germ-free rats, thereby proving that peri-apical periodontitis is caused by micro-organisms colonizing the root canal system.4 Studies have shown this flora to be polymicrobial, with a higher proportion of anaerobic bacteria.5-7
Micro-organisms may reach the pulp through a variety of routes. Carious lesions or dental procedures can result in the micro-organisms reaching the pulp via the dentinal tubules and a distance of 0.2 mm between the infected dentine and pulp has been shown to allow microbial access to the pulp.6 Open cavities caused by iatrogenic factors, inadequate or leaking restorations or trauma resulting in coronal fracture, directly exposes the pulp to the oral environment, resulting in infection of the pulpal tissues by commensal organisms found within the oral cavity. Once the micro-organisms invade the coronal aspect, the infection will migrate apically towards the peri-apical tissues. Micro-organisms can also gain access via the periodontal tissues, via lateral or apical foramen, in cases such as periodontal–endodontic lesions, or dental trauma where the periodontal ligament has been damaged. When the micro-organisms overcome the body's natural defences, endodontic disease develops and, in advanced cases, these micro-organisms may pass into the extra-radicular spaces resulting in apical abscesses.6,7
As these micro-organisms are required for the progression of endodontic disease, eradication and adequate disinfection will promote and allow healing.
Clinical findings
During the root canal treatment, clinically the root canal should be dry, with no suppuration prior to obturation. There should be no evidence of swellings and sinuses prior to completion of the root filling and essentially, the tooth should be free of infection prior to obturation. Persistent exudate following thorough chemo-mechanical debridement may be a sign of a cystic lesion.8
Favourable successful outcomes of root canal treatment include no loss of function, the absence of pain, swelling and sinus tracts, and a normal periodontal ligament space surrounding the root.9,10 Persistence of the above signs and symptoms may suggest non-healing.
Causes of non-healing
Unsuccessful endodontic treatment is a result of micro-organisms remaining within the root canal system following primary treatment, or re-infection from inadequate coronal or apical seals. This can be within the intra-radicular or extra-radicular spaces.
Causes of non-healing can be procedural factors that clinicians are able to control, while some are non-procedural and beyond the control of the treating clinician (Table 1).
Tooth related factors
Systemic factors
Persistent intra-radicular infection
Endogenous cholesterol crystal formation
Extra-radicular infection
Scar tissues formation during healing
Re-infection due to poor coronal or apical seals
Immunosuppression or reduced healing
Unrestorable teeth
Root fractures
Extruded exogenous material
True cystic lesions
Controllable factors
Procedural reasons for non-healing include insufficient aseptic control, suboptimal access cavity design resulting in incomplete removal of coronal pulp, missed canals, inadequate chemo-mechanical debridement and extruded exogenous material.11
Uncontrollable factors
Factors that are beyond the control of the treating clinician can often be identified during the initial assessment. This includes unrestorable teeth or those with root fractures, and complex endodontic lesions and anatomy.
The presence of these factors does not equate to non-healing as the process of healing is complex and depends on the ability of organisms to induce disease, and the host-immune response to the disease process.
Studies have shown that endogenous cholesterol released by the degenerating inflammatory cells present can result in a foreign body-type reaction. Cholesterol crystals irritate the tissues and are detrimental to post-treatment healing when present in large numbers.11 Furthermore, patient factors such as systemic conditions (e.g. diabetes), can impair healing and reduce the chances of success of root canal treatment.12
Maximizing success: pre-operatively
A thorough pre-operative assessment allows clinicians to identify and address any factors that could compromise the success of treatment.
Restorability assessment
Although patients are often keen to avoid extractions, ensuring that a tooth is restorable prior to undertaking endodontic treatment is key to ensuring success. Teeth that are unrestorable should not be root treated as an inability to achieve a post-operative coronal seal will inevitably result in re-infection and recurrence of symptoms.13
The amount of coronal tooth structure remaining and the structural integrity of this should be carefully assessed. Where extra-coronal restorations are required post-treatment, the clinician should assess whether there is enough of a ‘ferrule’, which is defined as 1.5–2 mm of dentine coronal to the margin of the restoration. This reduces the stresses within the tooth, protects the underlying tooth structure and reduces restoration failure.14
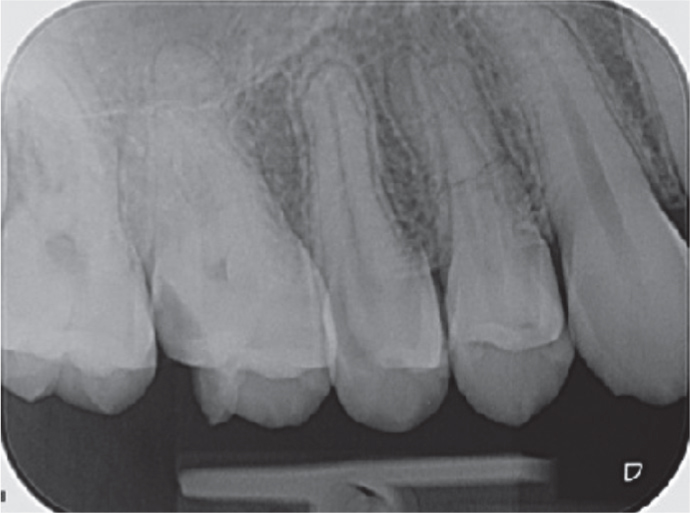
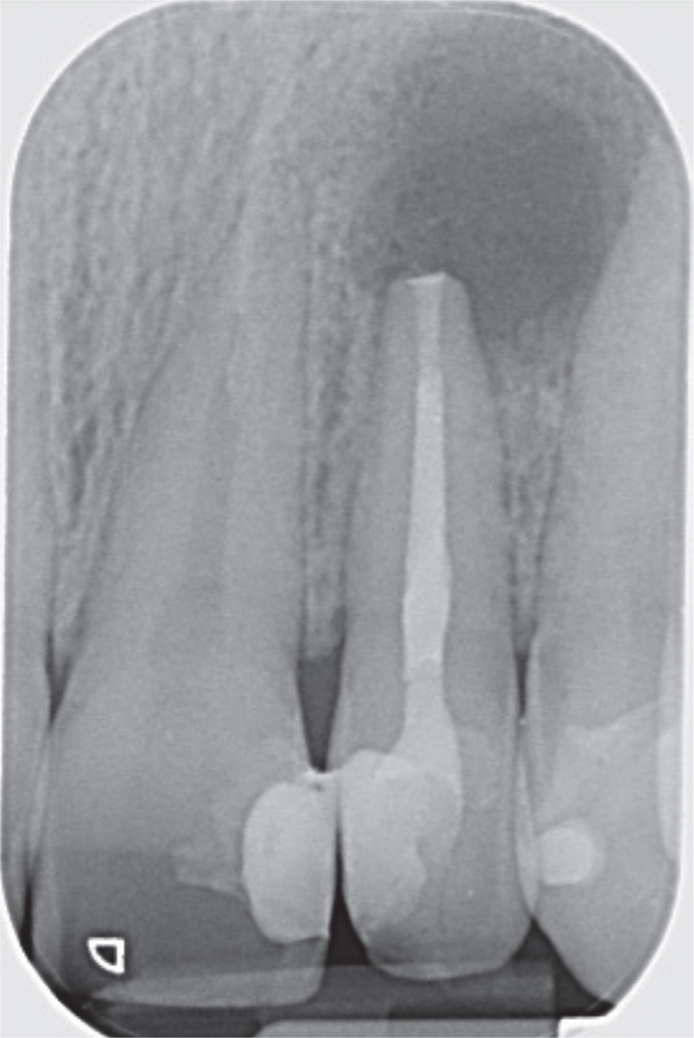
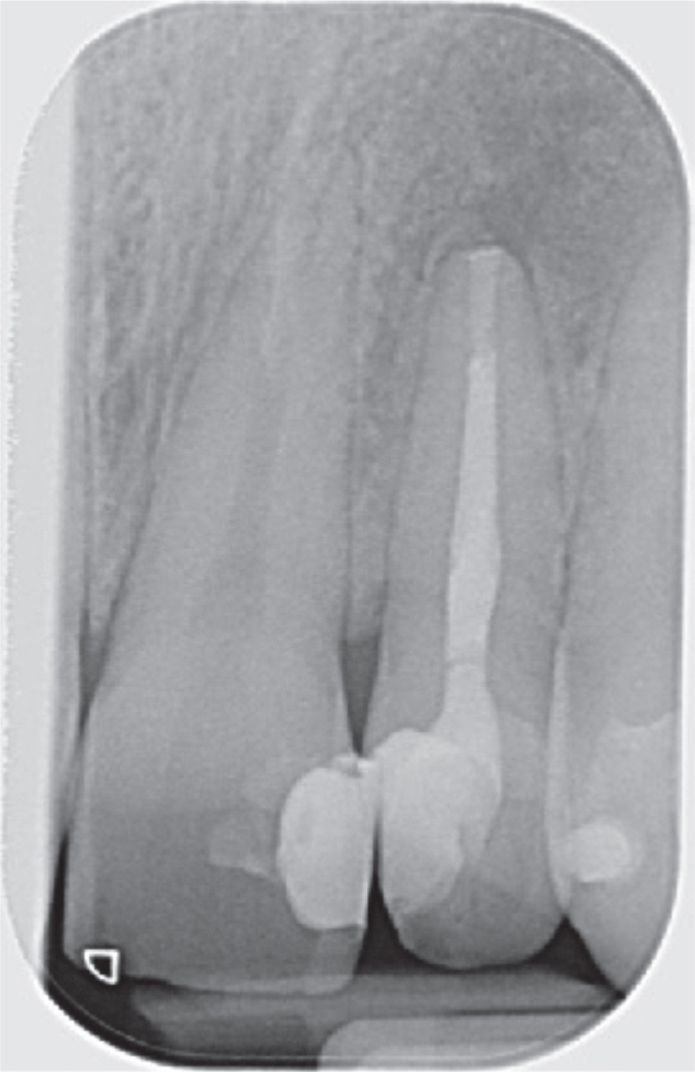
The periodontal status, to include the presence of periodontal pocketing and associated tooth mobility, should also be taken into consideration. It is important to note that mobility can occur in teeth that show periodontal stability, owing to the large extent of a peri-apical lesion. Therefore, the mobility should be carefully assessed and the distinction made. Single isolated periodontal pockets may be an indication of vertical root fractures. In single-rooted teeth, extraction will be required, and multi-rooted teeth will require either extraction or consideration of a hemi-section or root resection (Figures 1 and 2).15
Figure 1. Image of unrestorable UR5 due to inadequate coronal structure. UR4 is unrestorable due to medial-distal fracture.Figure 2. Peri-apical radiograph showing root fracture of UR4 which is seen clinically in Figure 1.
Indices such as the Tooth Restorability Index and the Dental Practicality Index can aid clinicians in taking a structured approach to restorability assessment.16,17 Restorability assessment allows a clear conversation with patients regarding the prognosis of the tooth in question and is a vital part of the consent process.
Endodontic assessment
Studies have shown that root-treated teeth with associated apical periodontitis may harbour residual infection within the complex apical anatomy. Residual microbes have been found mainly within uninstrumented spaces within the main canals, within the isthmus joining two canals, such as the mesial roots of mandibular first molars, and also within accessory/lateral canals. This can result in persistent intra-radicular infection, thereby preventing the resolution of endodontic lesions.11
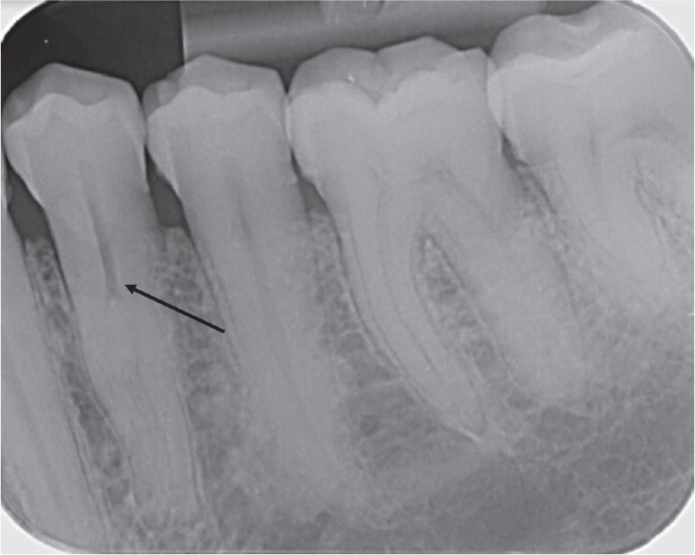
Radiographic examination plays a pivotal role in the endodontic assessment. Plain film radiography techniques, such as the use of the parallax technique, whereby two long cone peri-apical radiographs are taken at differing angles, can help to locate additional canals and visualize the anatomy. For example, where a canal appears to disappear on a radiograph in the mid or apical third, this suggests that the canal bifurcates and taking a parallax view can allow identification of this pre-operatively. Furthermore, in cases where symptoms do not resolve despite the outcome appearing favourable radiographically, a cone beam computed tomography (CBCT) scan can be useful in detecting further canals that may have been missed in the initial treatment.18 CBCT scans can also be used pre-operatively and are becoming more common as part of the initial assessment, to allow assessment of the canal anatomy and the presence and extent of apical lesions (Figure 3).
Figure 3. Deep apical divide seen within root canal of LL4.
There are several key clinical factors that have been shown to reduce the prognosis of root canal treatment and are useful to note when undertaking an endodontic assessment of a tooth. These are listed in Table 2 and an awareness of these is useful when determining the prognosis of each clinical case.
Presence of an apical lesion
Size of pre-operative lesion
Pre-operative sinus tract
Pre-operative pain
Inter-appointment flare-ups
The Royal College of Surgeons released guidelines to aid clinicians in determining the complexity of restorative treatment. Factors that contribute to the highest complexity within root canal assessment include a root curvature greater than 40°, canals that appear non-negotiable throughout their entire length, iatrogenic damage, pathological resorption, difficult root anatomy and peri-radicular surgery.20 The British Endodontic Society also has an online case assessment tool to help clinicians in assessing the risks and difficulties of individual cases.21
General dental practitioners may consider referral to a specialist in these complex cases if it is beyond their scope. A complexity assessment of a tooth prior to undertaking root canal treatment is highly recommended.
Maximizing success: operatively
Healing occurs when there is hard tissue regeneration and reduction in the size of the peri-apical radiolucency.22 All inflammatory peri-apical lesions should initially be treated with non-surgical methods and good procedural techniques will help to promote healing and maximize success.
Adequate access
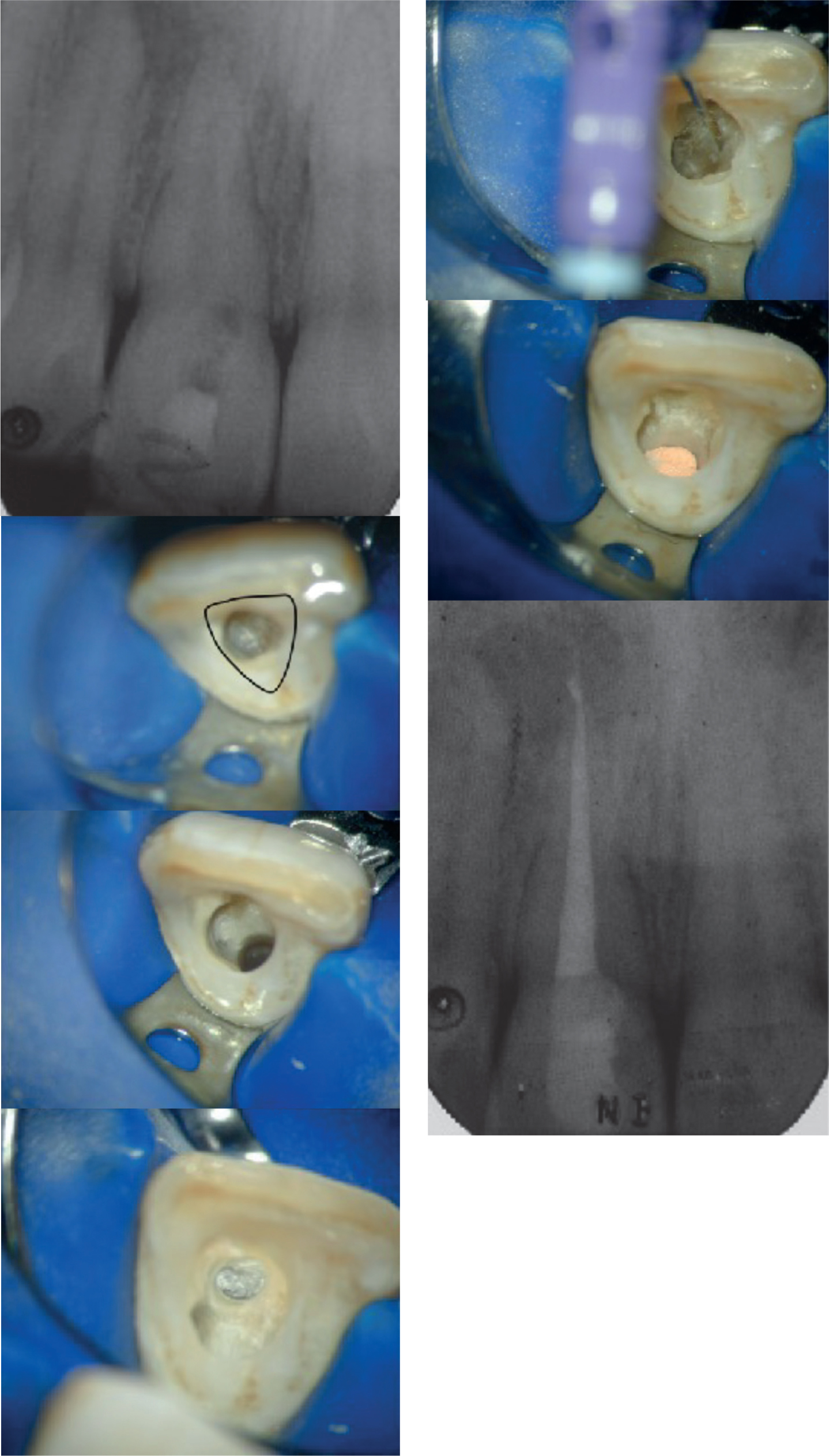
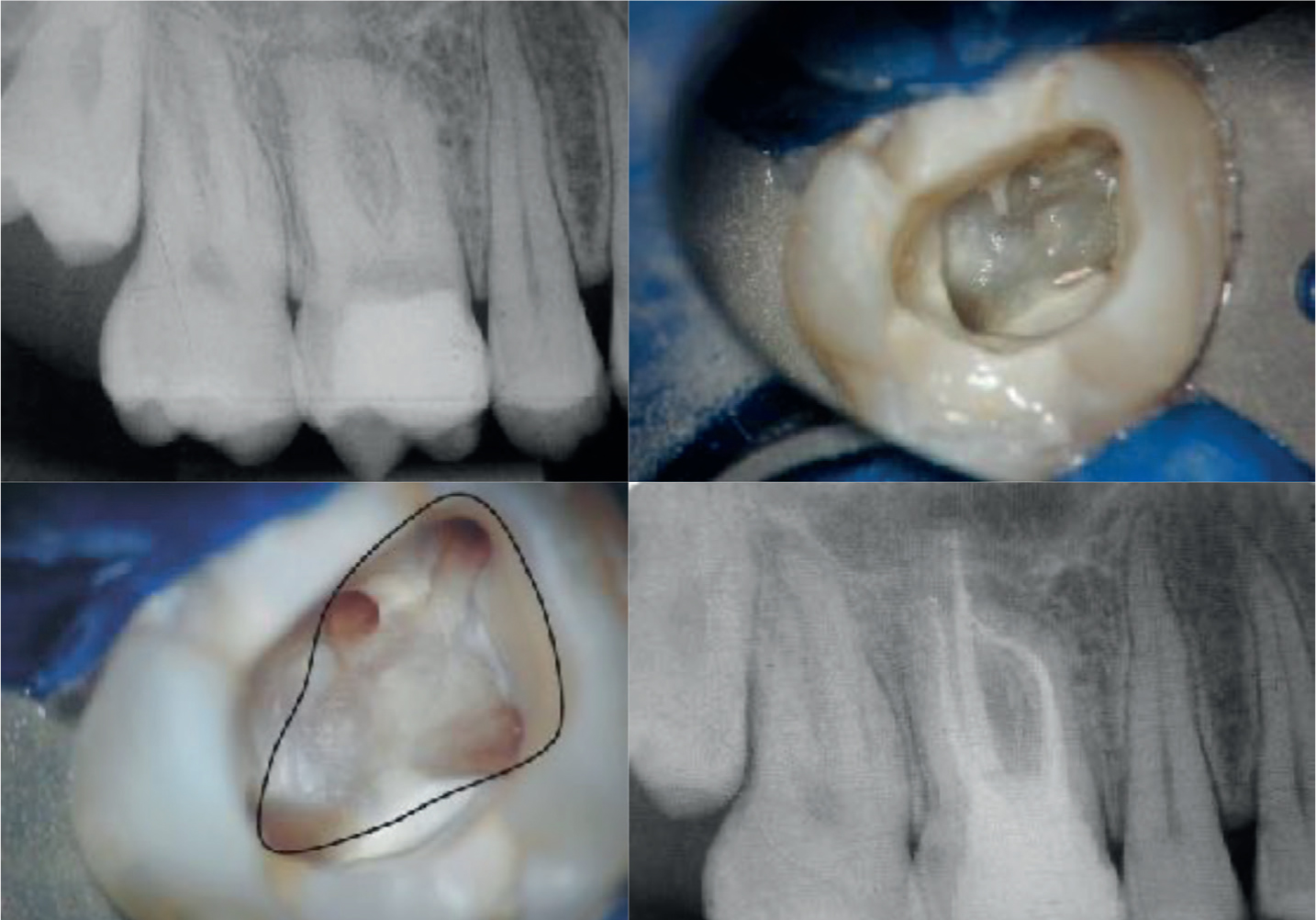
Adequate access allows removal of all of the coronal pulp tissues within the pulp canal chamber, including the pulp horns. It also ensures that all the root canals within the tooth have been identified and allows instrumentation along the entire length. Research has shown that incorrect access results in instrumentation of only the coronal aspect of the root canal. Achieving straight line access is important to improve instrumentation of the apical portion and decreases the chance of instrument fracture.23 Understanding of the root canal anatomy is required when determining how to access a tooth. The shape of the access cavity should reflect the shape of the pulp chamber and research by Krasner and Rankow determined ‘laws’ of anatomy that can aid in the identification of canal orifices (Figures 4–8).24
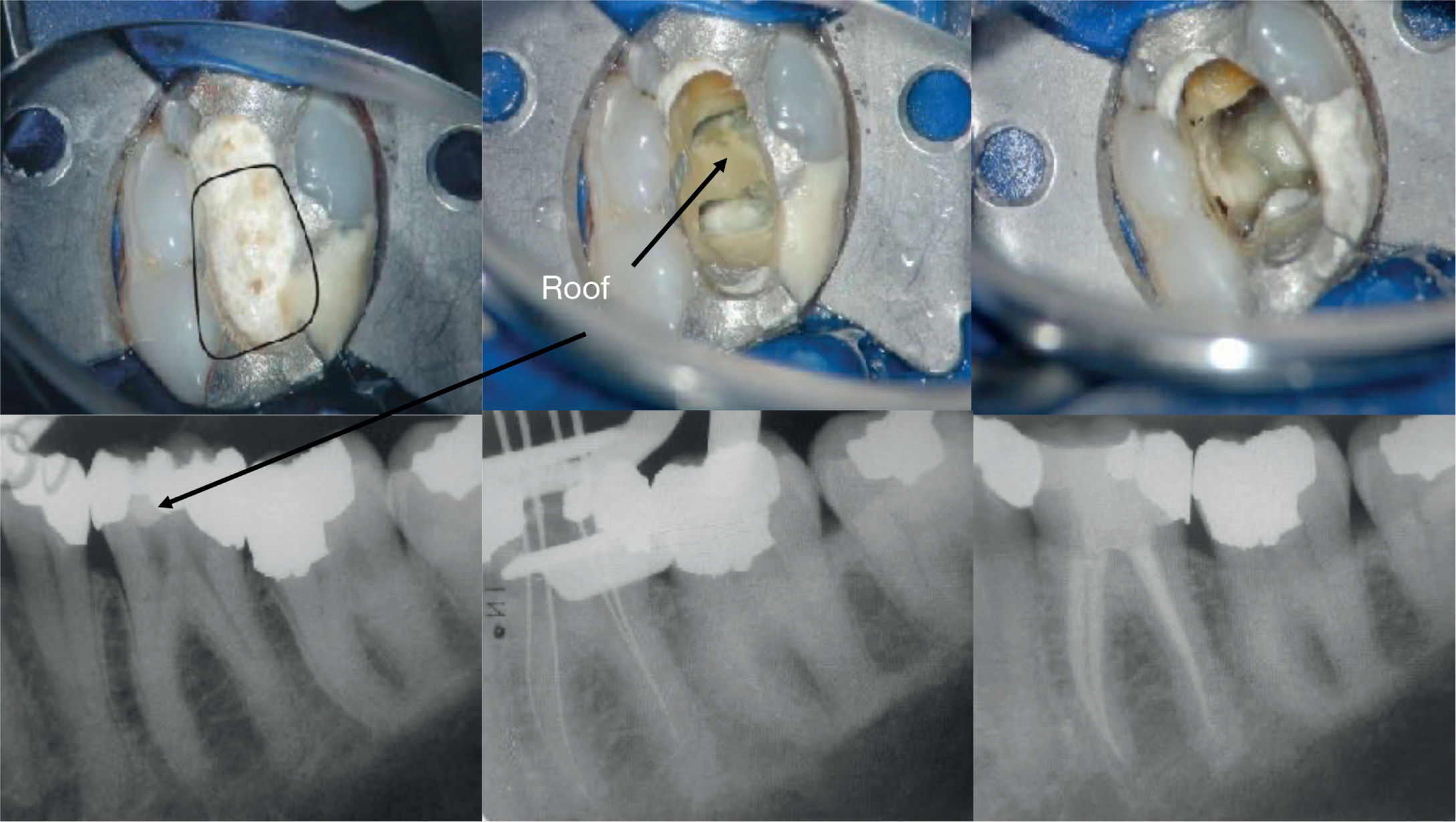
Figure 4. Insufficient initial access of UR1. Access was extended towards the incisal edge to allow canal identification and straight line access.Figure 5. Common error in maxillary molars: access is under-extended in the mesial marginal ridge area.Figure 6. Common error in maxillary molars: furcal perforation.Figure 7. Common error in maxillary molars: overextended mesially or distally. This case demonstrates overextension distally.Figure 8. Common errors in mandibular molars: overextended distally and incomplete removal of pulp chamber roof. Files demonstrate straight line access achieved. NB The pulp chamber floor is usually darker than the surrounding tooth structure.
Micro-organisms are the aetiological factor of endodontic disease, and the success of treatment relies on adequate disinfection. Disinfection ensures that all pulpal remnants and micro-organisms are removed from the canal prior to obturation. This is achieved via mechanical debridement using endodontic files, and the use of chemical irrigants. An ideal irrigant should provide lubrication for files, dissolve the organic matter and smear layer, and disinfect the root canal system, while also being biocompatible.25 Rubber dam should be used to ensure aseptic control, as well as provide protection of the airway and soft tissues. In addition, research has shown a significant improvement in endodontic outcomes with the use of rubber dams.26
Sodium hypochlorite (NaOCl) is considered the gold standard for endodontic irrigation because it has a broad spectrum of antimicrobial activity and organic tissue dissolution properties. The concentration used ranges from 0.5–6%, with higher concentrations showing increased ability to dissolve organic tissue and a faster rate of antimicrobial action. Lower concentrations should therefore be used in higher volumes and higher frequencies to ensure continuous replacement. A dwell time of 30 minutes has been suggested for NaOCl to allow sufficient bathing and debridement of the canals.25 Clinicians should therefore be mindful that there is adequate time for disinfection when using newer one-step file systems that can reduce treatment times, therefore reducing the duration of irrigant activity.
Ethylenediaminetetraacetic acid (EDTA) is a chelating agent that is effective in removing the smear layer and inorganic debris. The smear layer prevents penetration of the irrigant into the dentinal tubules, which contain bacteria and nutrients that allow for bacterial growth. EDTA has positive synergistic effects when used with NaOCl and is particularly effective in endodontic re-treatment cases and in the elimination of Enterococcus faecalis. EDTA 17% is often used as a penultimate rinse for 1 minute and repeated alternation with NaOCl should be avoided to prevent erosion of dentine, which can compromise tooth structure.25,27 Direct contact between EDTA and chlorhexidine should be avoided as a white precipitate can form.25
Chlorhexidine is a broad spectrum disinfecting agent and is bactericidal at higher concentrations by decomposing bacterial cell membranes. Use of chlorhexidine alone is not recommended, and it is often used in combination with other irrigants, although should not come in direct contact with NaOCl as they react and precipitate forms that blocks canals. There is evidence to suggest that it has pre-carcinogenic properties.25
It has been shown that bacteria in apical aspects of the root canal were associated more with the canal wall. Therefore, ensuring adequate chemo-mechanical disinfection of the canal wall in the apical region is vital (Table 3).28 A 27- or 30-gauge side-venting needle is advised, which reduces the risk of extrusion because the irrigant does not exit further than 1–2 mm beyond the needle tip.25 The root canal should therefore be adequately instrumented to an appropriate working length to allow irrigant penetration to the apical regions. Furthermore, the efficacy of the irrigant can be improved by manual agitation of the irrigation needle or the use of ‘GP-pumping’, whereby a gutta-percha (GP) cone is used to agitate the irrigant within the canal. Ultrasonic activation and heating of the chemical irrigant are alternative methods that can be used.25
27 or 30 gauge side-venting needle
Adequate instrumentation of all canals to within 2 mm of apex
Continuous and frequent replacement of irrigant
Manual agitation with master GP cone or ultrasonic activation
Sufficient time for irrigant contact
Recapitulation
The use of EDTA as a penultimate rinse to aid removal of smear layer
Intra-canal medication and multiple appointments
Calcium hydroxide is a widely used intra-canal medicament owing to its antibacterial properties and ability to dissolve tissue and neutralize endotoxins. Calcium hydroxide destroys the bacterial cell membrane components owing to its high alkalinity, with a pH around 12.5, acts as a physical barrier for bacterial proliferation and prevents coronal leakage.29 In cases of persistent apical periodontitis, calcium hydroxide may be left within the root canal for longer periods of time to help promote healing. The use of intra-canal medication also helps to dry persistently wet canals.30 The addition of iodine to calcium hydroxide-based medicaments, such as Vitapex (Neo Dental International, USA), enhances antibacterial properties and promotes hard tissue formation. It is recommended in the treatment of resorption, traumatized teeth and extensive apical lesions, although it can be difficult to remove (Figure 9).31,32
Figure 9. Peri-apical radiograph showing LR5 with Vitapex intra-canal medication that was used owing to persistent swelling.
Antibiotic-based medicaments have also been used widely, often during the initial access in cases of symptomatic pulpitis. An example of this is Odontopaste (ADM Australian Dental Manufacturing, Australia), which is a zinc oxide-based dressing containing clindamycin, alongside a steroid-based anti-inflammatory agent and calcium hydroxide. Ledermix (Ozdent Dental Products, Australia) is another antibiotic-containing medication that includes demeclocycline alongside a corticosteroid, triamcinolone acetonide.
Root canal treatment can be carried out as a single-visit approach or a multiple-visit approach. Research has shown that both approaches are equally effective, with no evidence to suggest that a particular approach is preferred.34 However, advantages of multiple appointments include allowing the use of intra-canal medication, more time for irrigant delivery and it allows the clinician the opportunity to assess healing and resolution of symptoms or sinus tracts prior to obturation.
Therefore, in cases with large apical lesions, persistently exudative canals and persistent sinus or symptoms, the use of intra-canal medication over multiple appointments should be considered to promote healing.
Recapitulation and apical patency
The most complex anatomy is within the apical portion of the root canal and instrumentation of the apical portion is required to ensure adequate disinfection. Ensuring apical patency via continuous recapitulation involves passively passing a small flexible K-file, 0.5–1 mm past the apical constriction, without widening the diameter. Instrumentation of the root canal should be up to the working length, which is advised to be 1–2 mm short of the radiographic apex. However, recapitulation past this point with a small file, ensures that the canal is not blocked with debris during instrumentation, which helps to avoid ledge formation, perforations and apical transportation, and ensures that apical patency is maintained. Care should be taken not to widen the apical constriction as this iatrogenic damage can result in loss of an apical seal.34 The use of glide path files has been shown to be beneficial in maintaining original root canal anatomy and decreasing apical extrusion.35
Apical seal and preventing extrusion
Apical gauging involves measuring the size of the apical constriction prior to obturation. The master cone GP point should have ‘tug back’ to ensure an adequate apical seal, which can help to prevent extrusion. The size of the GP point at the apex can be checked using a GP gauge and can be adjusted to give a more accurate fit using apical gauge rulers. Although large extruded pieces of GP can be well encapsulated and tolerated by the body, fine particles can lead to a localized tissue response and aggregation of inflammatory cells. This excess material, contaminated with chemicals that can irritate the tissues, results in a foreign body reaction and impairs apical healing.11 Research has shown that success rates drop by 62% in overextruded cases.36
Other materials used in endodontic treatments, such as paper points and cotton wool, can be pushed into the apical tissues during instrumentation. These contain cellulose fibres that cannot be degraded by the body and so remain within the tissues with the potential to induce a foreign body reaction. Further materials found within apical biopsies include amalgam, endodontic sealers and calcium salts from extruded calcium hydroxide.11 Care should be taken when removing coronal restorations to prevent displacement of materials into the root canal space and clinicians may find that sponges are easier to retrieve in comparison to cotton wool. Copious irrigation with careful suction should be used and files should be regularly cleaned.
Obturation and coronal seal
There are several techniques available for obturation, including cold lateral condensation, warm vertical or lateral compaction, single-cone obturation and carrier-based techniques. There is little difference in the long-term outcome of these different methods and generally the technique used is down to clinician preference.36 The aim of obturation is to ensure the root filling is well condensed, with no voids and within 2 mm of the radiographic apex.13 Research has shown that the success rates of root canal treatment falls by 12% for every millimetre that the canal is underfilled. Underfilled canals suggest inadequate preparation of the canal walls, which may still harbour bacterial colonies.36
Following obturation, the placement of an effective coronal seal immediately is essential to prevent re-infection and allow healing (Tables 4 and 5).13
Obturation with no voids
Obturation within 2 mm of radiographic apex
Satisfactory coronal seal
Pre-operative assessment
Radiographic examination: consider parallax techniques and CBCT to look for missed canals or complex anatomy
Restorability assessment: sufficient coronal tooth structure, ferrule, no root fractures, adequate bone levels
Endodontic assessment: patent canals, apical curvature, fractured instruments, canal deviations, calcification and pulp stones, accessory canals, root resorption, iatrogenic damage, consider specialist referral if too complex
Patient factors: compliance, reduced healing
Adequate access
Access cavity in correct position in the centre of the tooth and correct depth (measure depth of bur)
Consider ‘laws of anatomy’ to help locate canals and dictate access cavity
All canals accessed and scouted using small handfiles
Pulp horns cleared
Straight line access achieved
Disinfection protocol
Rubber dam used
27 or 30 gauge side-venting needle
Irrigation with sodium hypochlorite and consideration of EDTA as penultimate rinse
Continuous replacement of irrigant and adequate dwell time
Manual agitation with GP or ultrasonics
Consider multiple appointments with the use of intra-canal medication for persistently exudative canals, large apical lesions or symptomatic teeth
Instrumentation
Instrument to within 2 mm of apex
Continuous recapitulation and maintain apical patency
Creation of glide path and maintain original anatomy
Obturationd
Achieve a dry canal
Apical gauging to achieve apical seal and prevent extrusion
Within 2 mm of apex
Well condensed with no voids
Satisfactory coronal seal
Consider dual obturation and apicectomy if canal persistently exudative
Dual obturation and apicectomy
A dry canal should be achieved prior to obturation. If a canal is persistently exudative following multiple appointments, it may indicate a cystic lesion. A ‘true cyst’ is self-sustaining in nature, and less likely to resolve with non-surgical treatment alone, resulting in persistent apical periodontitis.11 Alternative treatment options, such as dual obturation with apicectomy may be considered. This is discussed below, alongside a clinical case outlining the treatment performed.
The Royal College of Surgeons released updated guidelines for peri-radicular surgery in 2020. Indications for peri-radicular surgery include a persistently exudative canal ‘despite repeated chemo-mechanical debridement’ (Table 6). Peri-radicular surgery can help to resolve microbial infection as it allows access to the apical tissues and can by-pass apical anatomical complications.8
Symptomatic or progressive peri-radicular disease following optimal primary root treatment
Tooth is unrestorable or root fracture
To maintain structural integrity or a well-fitting fixed prosthesis or avoid removal of post in an otherwise well-filled tooth which is symptomatic or with progressive peri-radicular disease
Poor coronal seal
Where iatrogenic or developmental anomalies prevent orthograde treatment
Periodontal–endodontic lesions
Biopsy of peri-radicular tissue
Compromised bone support or root length following resection
Visualization of peri-radicular tissue required for perforation or root fracture
Difficult or risky access
Medical history factors
Lack of experience or equipment/materials
Clinical case
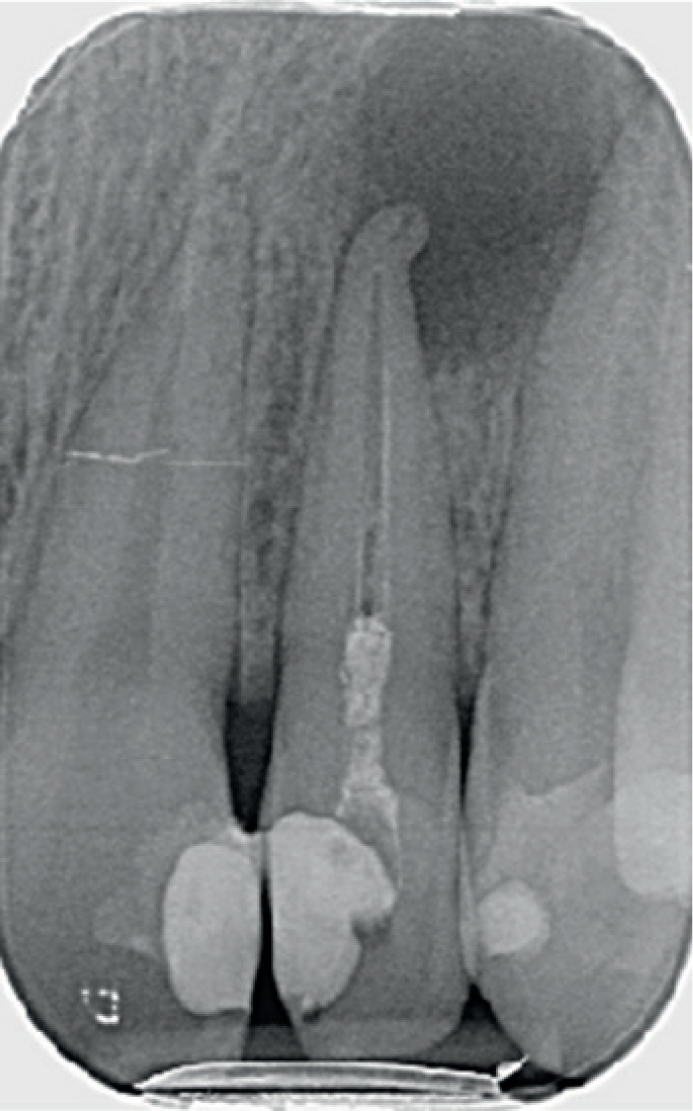
A 17-year-old patient attended the restorative department at the Birmingham Dental Hospital following referral from the community dental services. The referral stated that primary disease had been stabilized, with restoration of multiple carious teeth, and primary endodontic treatment had been initiated on the UL2. This endodontic treatment had been undertaken over multiple appointments with calcium hydroxide used as an intra-canal medicament for several weeks; however, obturation was not completed owing to an inability to achieve a dry canal prior to obturation. Figure 10 shows the radiograph taken by the referring clinician. Signs and symptoms of a chronic apical abscess persisted, although instrumentation and disinfection had been undertaken over multiple visits.
Figure 10. Pre-operative radiograph showing the temporary intra-canal medication and a large, potentially cystic, apical lesion.
The UL2 was re-assessed clinically and radiographically. The pre-operative radiograph showed a lack of Ca(OH)2 dressing to the apex of the tooth. The tooth had been accessed relatively palatally and had a large peri-apical radiolucency. There was a distal curvature on the plain film (with the position of the lesion indicating a further disto-palatal curvature and palatal peri-apical infection). There was a loss of the canal continuity from the main root canal to the apical 2 mm and acute complex apical anatomy. Large NiTi files had been used, but patency was not established, which was discussed in the referral letter. A moderate-sized restoration was in situ, which appeared well sealed. The careful pre-operative assessment noted a restorable tooth, with adequate access cavity and a restorable remaining tooth structure. The diagnosis was determined using the American Association of Endodontics guidelines as: UL2 previously initiated treatment, symptomatic apical periodontitis. This was complicated by suspected apical transportation of the canal, and acute apical curvature with a large peri-apical radiolucency.
The findings were discussed with the patient and the clinical complexity reinforced. An orthograde approach was initially indicated with the aim of achieving apical patency using small pre-curved files, instrumenting and chemo-mechanical disinfection.
The UL2 was re-accessed under rubber dam, the access was refined and brought towards the incisal tip. Further chemo-mechanical debridement was undertaken using small stainless steel K-files to attempt to achieve apical patency and copious 5% sodium hypochlorite irrigation was used. After two visits, the apical anatomy could not be negotiated, and the working length determined to this point. Even after irrigation and inter-appointment dressing with Ca(OH)2, a large amount of canal exudate was present and a dry canal unachievable. The tooth was therefore temporized with a provisional restoration.
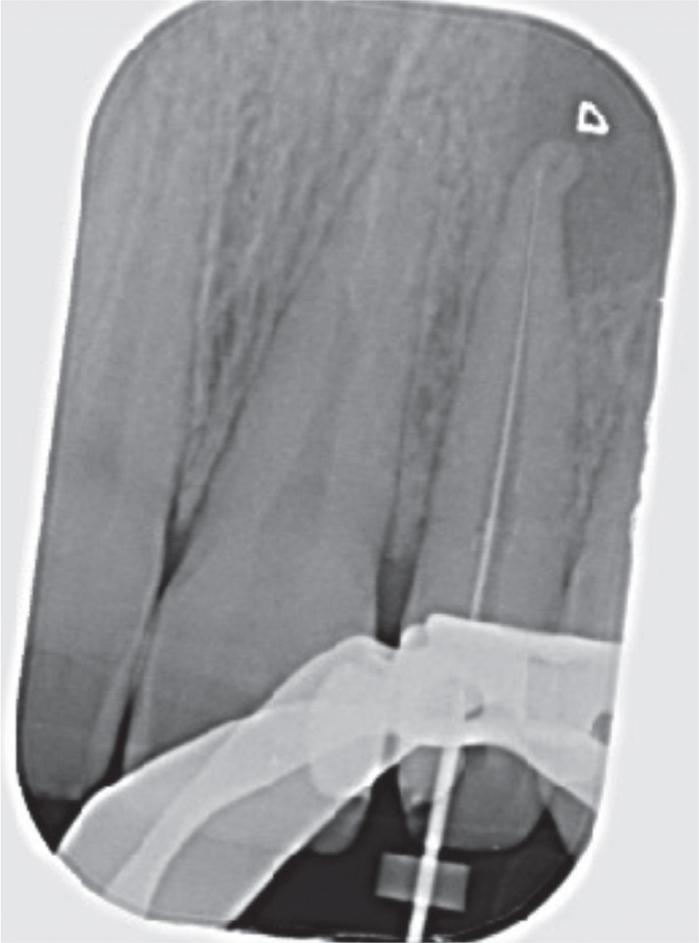
The treatment options were given to the patient, including placement of calcium hydroxide for 3 months (although this was previously attempted by the community dental team and was unlikely to resolve the infection) or peri-radicular surgery. The patient opted for peri-radicular surgery (Figure 11).
Figure 11. Working length radiograph. Note the significant apical curvature that was difficult to negotiate.
In the following appointment, the tooth was re-accessed and the master cone was cut to 6 mm short of the apex (to leave space for the root resection and root end filling). The master GP cone was used to temporarily occlude the canal and the access cavity was sealed with a temporary material.
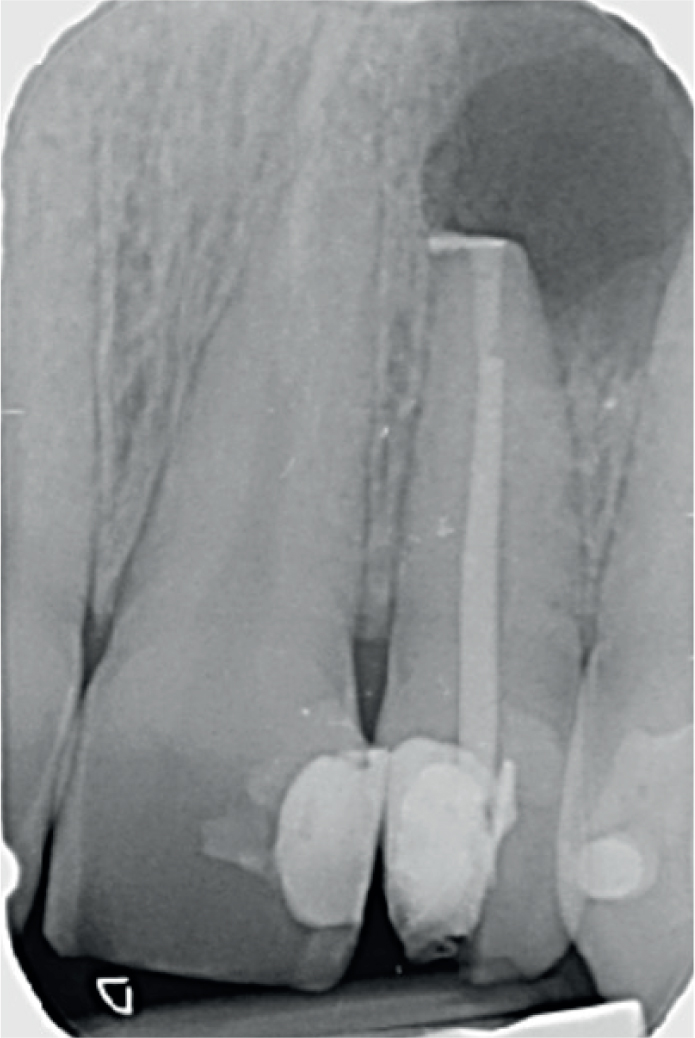
A full-thickness muco-periosteal flap was raised from the UR1 to the UL3 with a distal relieving incision, ensuring good access to the apical portion. This revealed thinning of the buccal bone at the apex of the UL2, which was accessed using hand instruments and widened using a surgical hand-piece. The crypt was debrided and a sample taken for histology. A 3 mm root end resection was completed with a back venting fast hand-piece and an ultrasonic device was used to undertake preparation of the apical 3 mm of the root end. Mineral trioxide aggregate (MTA) was used to fill the apical portion. Crypt haemostasis was achieved and the flap was repositioned with 5-0 Prolene sutures (Figure 12).
Figure 12. Mid-operative radiograph showing the master cone temporarily occluding the root canal and the root end filling, with excess MTA which was later removed prior to closure.
In the following appointment, the tooth was re-accessed and the temporary master cone was removed (Figure 13). Further irrigation of the canal was completed and a dry canal was achieved. The definitive obturation was completed using warm vertical compaction and the access cavity was definitively sealed.
Figure 13. Immediate post-operative radiograph showing a well condensed root canal and good coronal seal.
The patient was reviewed after 6 months and the tooth had remained asymptomatic (Figure 14). A repeat radiograph was taken that showed signs of apical healing. The histology confirmed the lesion to be a radicular cyst.
Figure 14. Radiograph taken at the 6-month review showing good signs of apical healing.
Discussion
This case highlights how adequate pre-operative assessment and following a systematic approach will improve success in the management of persistently symptomatic teeth. The referring dentist identified that they were unable to achieve a dry canal, despite repeated chemo-mechanical debridement and the use of intra-canal medication and appropriately referred onwards for specialist care. Pre-operative assessment highlighted the complex apical curvature and an attempt to overcome this was made by modifying the access cavity to achieve straight line access, using small pre-curved hand files to scout the canal and manual agitation of the irrigant. As there was still persistent exudate despite repeated appointments, with adequate disinfection and intra-canal medication the treatment approach was therefore adapted to dual obturation and apicectomy which resulted in a successful outcome.
General dental practitioners should ensure good procedural techniques are followed to maximize success and refer onwards to a specialist when teeth are persistently symptomatic or deemed too complex during assessment.
Conclusion
Although achieving a root canal free of micro-organisms is ideal, it is very unlikely to achieve complete disinfection. Periapical lesions may still heal even when infection is present, and this is thought to be due to the microbial quantities and virulence being below the critical levels required to maintain inflammation.10 Reducing the microbial load enough to allow the immune defences of the body to resolve the infection allows healing to take place. Success can be maximized by ensuring good endodontic techniques or, in some cases, consideration of peri-radicular surgery.