Torabinejad M, Hong CU, McDonald F, Pitt Ford TR Physical and chemical properties of a new root-end filling material. J Endod. 1995; 21:(7)349-353
Torabinejad M, Hong CU, Lee SJ, Monsef M, Pitt ford TR Investigation of mineral trioxide aggregate for root-end filling in dogs. J Endod. 1995; 21:(12)603-608
Torabinejad M, Watson T, Pitt Ford TR Sealing ability of a mineral trioxide aggregate when used as a root-end filling material. J Endod. 1993; 19:(12)591-595
Torabinejad M, Chivian N Clinical applications of mineral trioxide aggregate. J Endod. 1999; 25:(3)197-205
Belobrov I, Parashos P Treatment of tooth discoloration after the use of white mineral trioxide aggregate. J Endod. 2011; 37:(7)1017-1020
Han L, Okiji T Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J. 2011; 44:1081-1087
Bachoo I, Seymour D, Brunton P A biocompatible and bioactive replacement for dentine: is this a reality? The properties and uses of a novel calcium-based cement. Br Dent J. 2013; 214:(2)
Koubi G, Colon P, Franquin JC Clinical evaluation of the performance and safety of a new dentine substitute, Biodentine, in the restoration of posterior teeth – a prospective study. Clin Oral Investig. 2013; 17:(1)243-249
Tanomaru-Filho M, Tanomaru JM, Barros DB In vitro antimicrobial activity of endodontic sealers, MTA-based cements and Portland cement. J Oral Sci. 2007; 49:(1)41-45
Cox CF, Bergenholtz G, Heys DR Pulp capping of dental pulp mechanically exposed to oral microflora: a 1–2 year observation of wound healing in the monkey. J Oral Pathol. 1985; 14:(2)156-168
Fuks A, Bielak S, Chosak A Clinical and radiographic assessment of direct pulp capping and pulpotomy in young permanent teeth. Pediatr Dent. 1982; 4:(3)240-244
Farsi N, Alamoudi N, Balto K, Al Mushayt A Clinical assessment of mineral trioxide aggregate (MTA) as direct pulp capping in young permanent teeth. J Clin Pediatr Dent. 2006; 31:(2)72-76
Cvek M A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endod. 1978; 4:(8)232-237
Eghbal MJ, Asgary S, Baglue RA MTA pulpotomy of human permanent molars with irreversible pulpitis. Aust Endod J. 2009; 35:(1)4-8
Al-Hiyasat AS, Barrieshi-Nusair KM, Al-Omari MA The radiographic outcomes of direct pulp-capping procedures performed by dental students: a retrospective study. J Am Dent Assoc. 2006; 137:(12)1699-1705
Hargreaves KM, Diogenes A, Teixeira FB Treatment options: biological basis of regenerative endodontic procedures. J Endod. 2013; 39:(3)S30-S43
Murray PE, Garcia-Godoy F, Hargreaves KM Regenerative endodontics: a review of current status and a call for action. J Endod. 2007; 33:(4)377-390
Diogenes A, Henry MA, Teixeira FB An update on clinical regenerative endodontics. Endod Topics. 2013; 28:(1)2-23
Trevino EG, Patwardhan AN, Henry MA Effect of irrigants on the survival of human stem cells of the apical papilla in a platelet-rich plasma scaffold in human root tips. J Endod. 2011; 37:(8)1109-1115
Egusa H, Sonoyama W, Nishimura M Stem cells in dentistry – Part I: stem cell sources. J Prosthodont Res. 2012; 56:(3)151-165
Cehreli ZC, Isbitiren B, Sara S, Erbas G Regenerative endodontic treatment (revascularization) of immature necrotic molars medicated with calcium hydroxide: a case series. J Endod. 2011; 37:(9)1327-1330
Torabinejad M, Turman M Revitalization of tooth with necrotic pulp and open apex by using platelet-rich plasma: a case report. J Endod. 2011; 37:(2)265-268
Chen MH, Chen KL, Chen CA Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int Endod J. 2012; 45:(3)294-305
Narayana P, Hartwell GR, Wallace R, Nair UP Endodontic clinical management of a dens invaginatus case by using a unique treatment approach: a case report. J Endod. 2012; 38:(8)1145-1148
Sugaya T, Kawanami M, Noguchi H Periodontal healing after bonding treatment of vertical root fracture. Dent Traumatol. 2001; 17:(4)174-179
Andreasen J, Pitt Ford T A radiographic study of the effect of various retrograde fillings on periapical healing after replantation. Dent Traumatol. 1994; 10:(6)276-281
Modern endodontic principles part 8: the future of endodontics Reza Vahid Roudsari Sarra Jawad Carly Taylor James Darcey Alison Qualtrough Dental Update 2025 43:5, 430-441.
Authors
Reza VahidRoudsari
DDS, MFDS, MSc, PGCert(OMFS)
Clinical Lecturer/Honorary Specialty Registrar in Restorative Dentistry, Dental School, University of Manchester
Although the principles of endodontics have remained unchanged for many decades, root canal treatment has been subject to major changes in the past few years. This paper outlines the cutting-edge advances including the materials and techniques used.
CPD/Clinical Relevance: This article provides an overview of bioactive materials and insight into regenerative endodontics, vital pulp therapy and intentional replantation.
Article
Although the basic principles of endodontics have remained unchanged for nearly a century, there have been significant improvements in the materials and instruments used. The introduction of bioactive materials has been a major step forward and, recently, endodontic regeneration is changing shape from myth to reality. This paper will begin by focusing on the latest information on available bioactive materials and will continue by discussing our current understanding of endodontic regeneration and intentional replantation.
Bioactive materials
The term ‘bioactive materials’ covers a range of similar calcium silicate-based materials that are not only biocompatible but promote healing and regeneration of tissues. The most notable examples of these are ProRoot MTA (Tulsa Dental Products, USA) and MTA Angelus (Angelus, Brazil). MTA is hydrophilic and when mixed with water the powder forms a colloidal gel and sets via a hydration reaction. The setting time is approximately 2 hours 45 minutes.1
Set MTA contains calcium hydroxide in a silicate matrix. The pH of MTA is 10.2–12.5. The material is regarded as bioactive as it triggers the precipitation of hydroxyapatite crystals through the interaction of calcium and phosphate ions forming a ‘dentine bridge’. This hydroxyapatite layer not only forms a seal at the interface with dentine but is both osteoconductive and osteogenic at the interface with vital tissues. There is therefore the capacity for new cementum to form on the surface of MTA.2 This sets MTA apart from all other traditional restorative materials and has become a significant step forward in the goal of tissue regeneration.3 These bioactive properties and excellent sealing abilities of MTA result in a variety of clinical uses in the field of endodontics:4
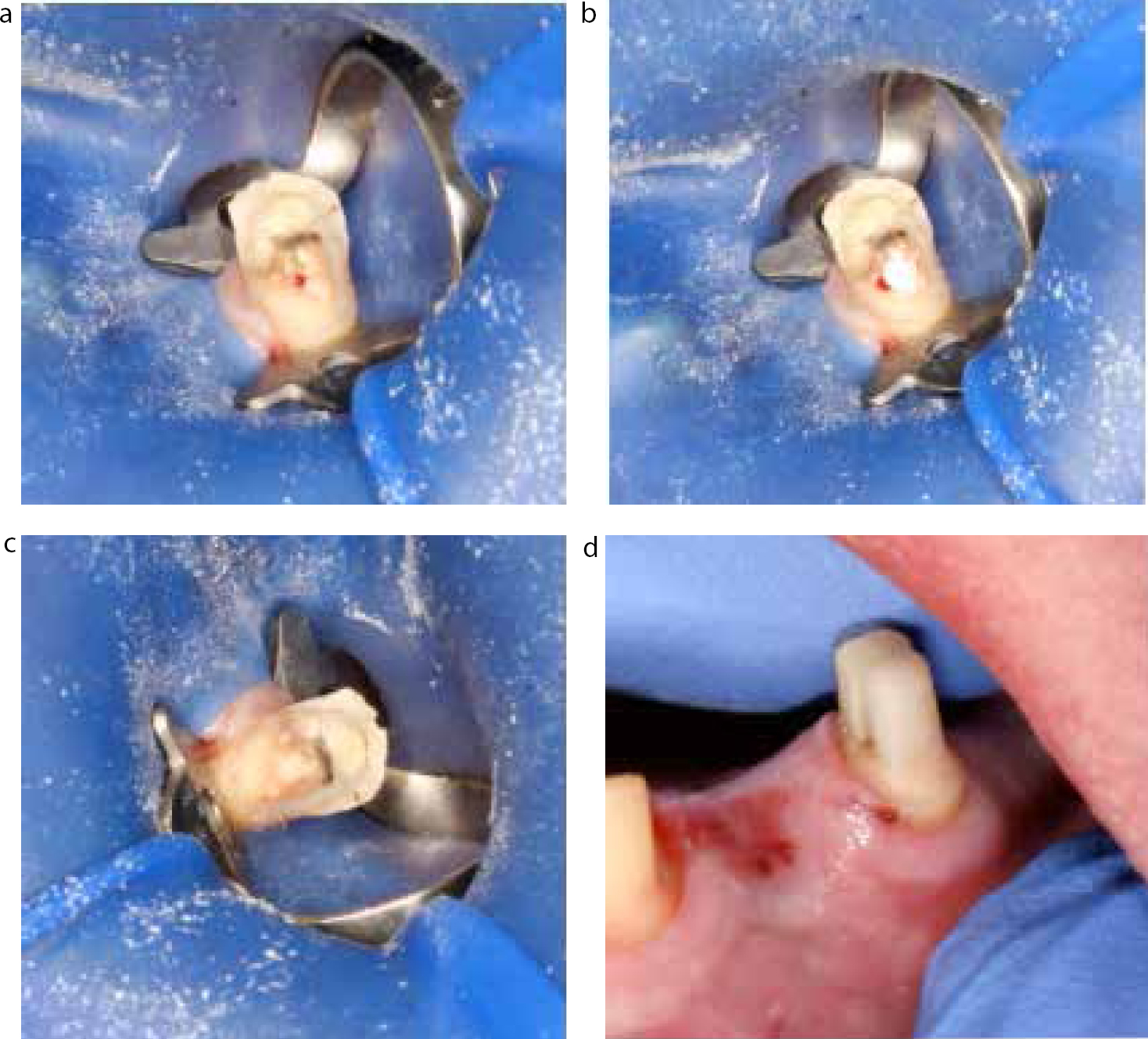
Vital pulp therapy, including indirect and direct pulp capping, partial and complete pulpotomy (Figure 1);
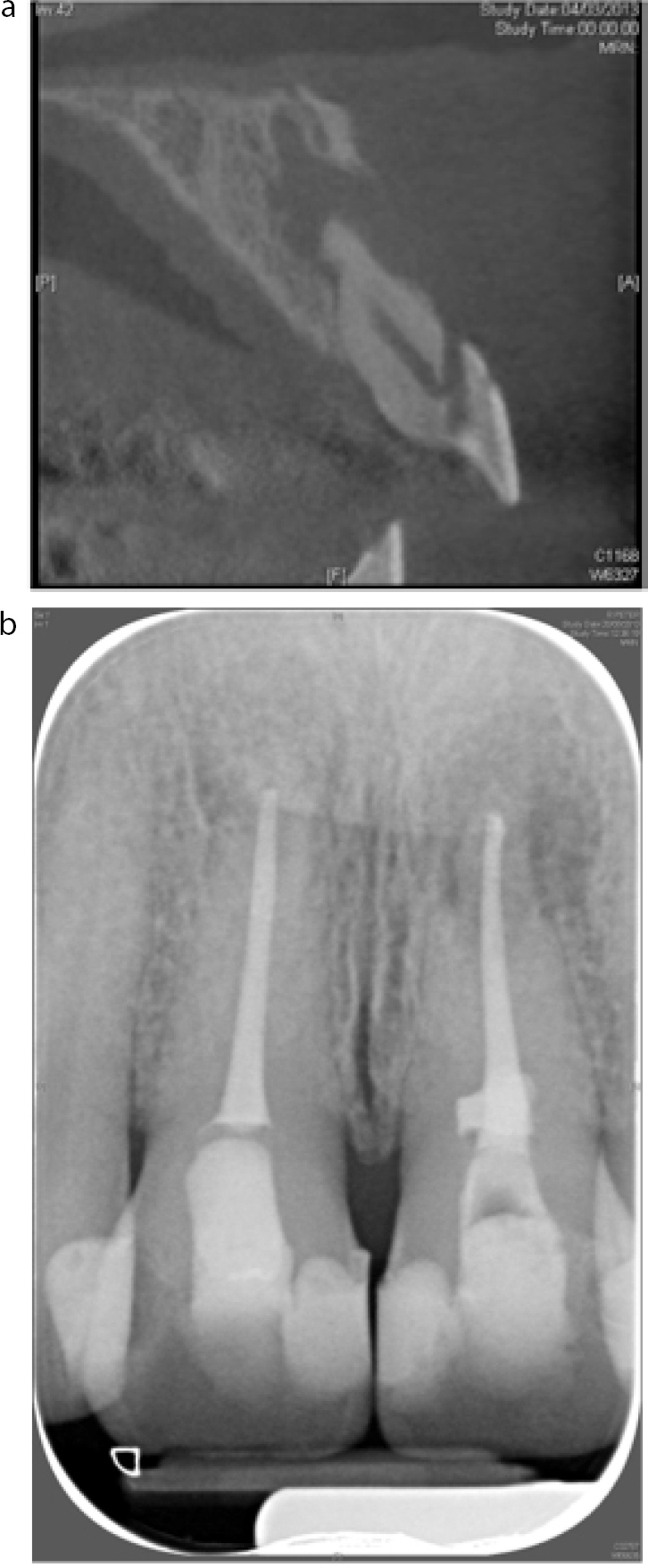
Apexification of wide or incomplete apices (Figure 2);
Apical obturation in surgical endodontics (Figure 4).
Figure 1.
(a–d) Indirect pulp capping UL4 with Biodentine (Septodont, St Maur, France). This will form a dentine substitute and a direct composite restoration will be placed over the Biodentine.Figure 2.
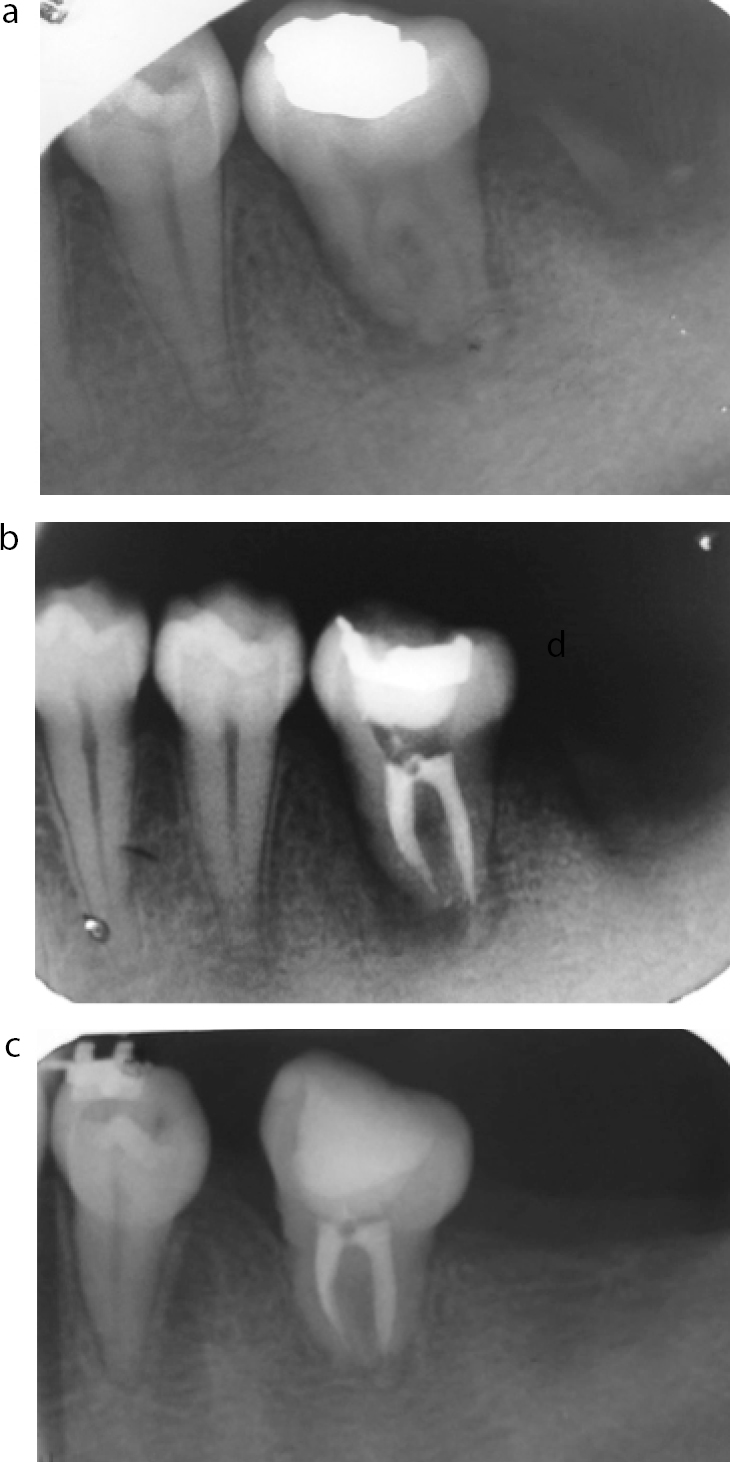
(a, b) MTA apexification UR1.Figure 3.
(a, b) Following orthograde endodontics the perforation UL1 was repaired with MTA.Figure 4.
(a, b) Apical obturation with MTA; UR1 and UR2 following root end preparation.
MTA is not an easy material to mix or manipulate; patience and practice are required to master its use and practitioners may need to invest in additional instruments to facilitate placement (Figure 5). The compressive strength of set MTA is similar to reinforced zinc oxide eugenol which remains significantly less than composites or amalgam; thus, it is not indicated for direct plastic restorations. Furthermore, the long setting time prohibits placement in sites open to the oral cavity and immediate preparation. MTA can ‘wash out’ in the presence of excess moisture. When used internally, grey MTA is associated with discoloration of teeth, thus White MTA, containing no iron compounds, has been produced. However, even white MTA can discolour teeth and patients should give their consent to this accordingly5 (Figure 6).
Figure 5. The Micro Apical Placement System: essentially a very small carrier device for controlled placement of MTA.Figure 6. Even using white MTA the teeth may discolour. This patient from Figure 3 has greying in the UL1 cervical region.
As a consequence of these limitations, there has since been a drive to produce materials with similar properties but improved handling. One such material is Biodentine (Septodont, Saint-Maur, France) (Figure 7), which consists of tricalcium silicate, calcium carbonate and zirconium dioxide. This material has similar bioactivity to MTA but with a reduced setting time of 12 minutes.6 Once set, the material has a compressive strength of 300 MPA, comparable to dentine, and a microhardness greater than glass ionomer.7 These properties vastly improve handling and permit its use as a provisional restorative material with the potential for the clinician to prepare the set material immediately after placement.
Figure 7.
(a)
Biodentine (Septodont, St Maur, France). (b) When mixed forms a creamy gel that is comparatively easy to manipulate.
It cannot be used in areas of high aesthetic need or as a long-term enamel replacement. However, once placed, the material can be cut back and used as a definitive base, of particular relevance in direct and indirect pulp capping. Using a silane-bonding agent, it is possible to bond composite to Biodentine.8 This combination of properties has led to Biodentine being regarded as a dentine replacement.
Owing to the high pH, excellent sealing abilities and biocompatibility, there has also been a drive to incorporate bioactive materials into endodontic obturation materials and systems. Products such as MTA Fillapex (Angelus Soluções Odontológicas, Londrina, PR, Brazil) and MTA Plus (Prevest-Denpro, Jammu City, India) are two such materials. These are endodontic sealers containing MTA. Fillapex has approximately 40% MTA in a resin matrix and may offer similar antibacterial and sealing abilities as conventional sealers such as AH+ (Dentsply, Konstanz, Germany).9 There is currently little clinical data demonstrating any significant advantage to the use of MTA-containing sealers.
From the clinical perspective, these materials are exciting but questions must be asked about ease of removal and biological consequences. As MTA is essentially concrete, it is virtually impossible to remove. Clinicians should exercise caution when using any materials if there are concerns about the need for future retreatment or placement of intraradicular posts to support a coronal restoration. Currently evidence around the use of alternative bioactive materials is mostly limited to in vitro studies and case reports. Therefore, clinicians may often be restricted to the manufacturers marketing material.
Vital pulp therapy
The aim of vital pulp therapy is to preserve the vitality of the pulp following exposure due to trauma, caries and restorative procedures. This can be carried out via a number of methods including direct and indirect pulp capping, Cvek partial pulpotomy and full pulpotomy. The success of such procedures is intimately related to the inflammatory status of the pulp, the material used and the ability to create a seal preventing bacterial ingress. Bioactive materials offer two distinct advantages. The first is an improved quality of the dentinal bridge formation underneath the material. The second is a superior seal against micro-leakage, this being thought to be a significant cause of failure.10
Traditional direct pulp capping involves direct placement of calcium hydroxide on the exposed pulp and has a reported success rate of 80%11 (Figure 8). Owing to limitations in our accuracy of diagnosis of the inflammatory state of the pulp and challenges in providing good coronal seal, the success rate is rather low. In cases with no signs of irreversible pulpitis and in the presence of complete haemostasis after caries excavation, direct pulp capping with MTA has favourable success. It is as high as 93% at 2 years.12
Figure 8.
(a–d) Direct pulp capping. During temporary crown removal the buccal cusp fractured UR5 exposing the pulp. Rubber dam was applied immediately, setting calcium hydroxide (Life™) placed directly on to the exposure, a glass ionomer layer over the dressing and the core completed in composite resin.
Partial or Cvek pulpotomy has advantages over pulp capping. Since the inflamed coronal pulp is removed approximately 2–3 mm below the exposure point in conjunction with effective irrigation, this treatment can result in a success rate of up to 96%.13 This method is indicated for teeth with a history of no or minimal pain, as well as no sign of radiographic changes, tenderness to percussion, sensitivity or mobility.
A full pulpotomy is indicated in symptomatic permanent teeth when the inflammation has extended through the coronal pulp and the level of inflammation cannot be predicted. One study has reported 100% success rates in teeth with irreversible pulpitis treated with full MTA pulpotomy (Figure 9).14
Figure 9. Full pulpotomy. (a) Pre-operative radiographic image of a young lower permanent first molar. (b) Full pulpotomy complete and (c)Biodentine placed. (d) Immediate post-operative radiographic image.
It must be highlighted that it is impossible to assess pulpal health clinically accurately. The judgement as to whether to cap, partially remove the pulp, or extirpate is not a precise science. The clinician must recognize that outcomes may be different, depending upon whether trauma or caries are the principal reasons for exposure: carious exposures have worse outcomes.15 Should the clinician elect to perform vital pulpotomy? If irreversible pulpal disease or pulpal necrosis develop subsequently, re-access through MTA may be challenging. Furthermore, pulp canal obliteration following vital pulp therapy may, at best, complicate but, at worst, prevent orthograde root canal treatment in such instances. It is therefore essential that the patient is fully aware of the risks as well as the benefits.
Regenerative endodontics
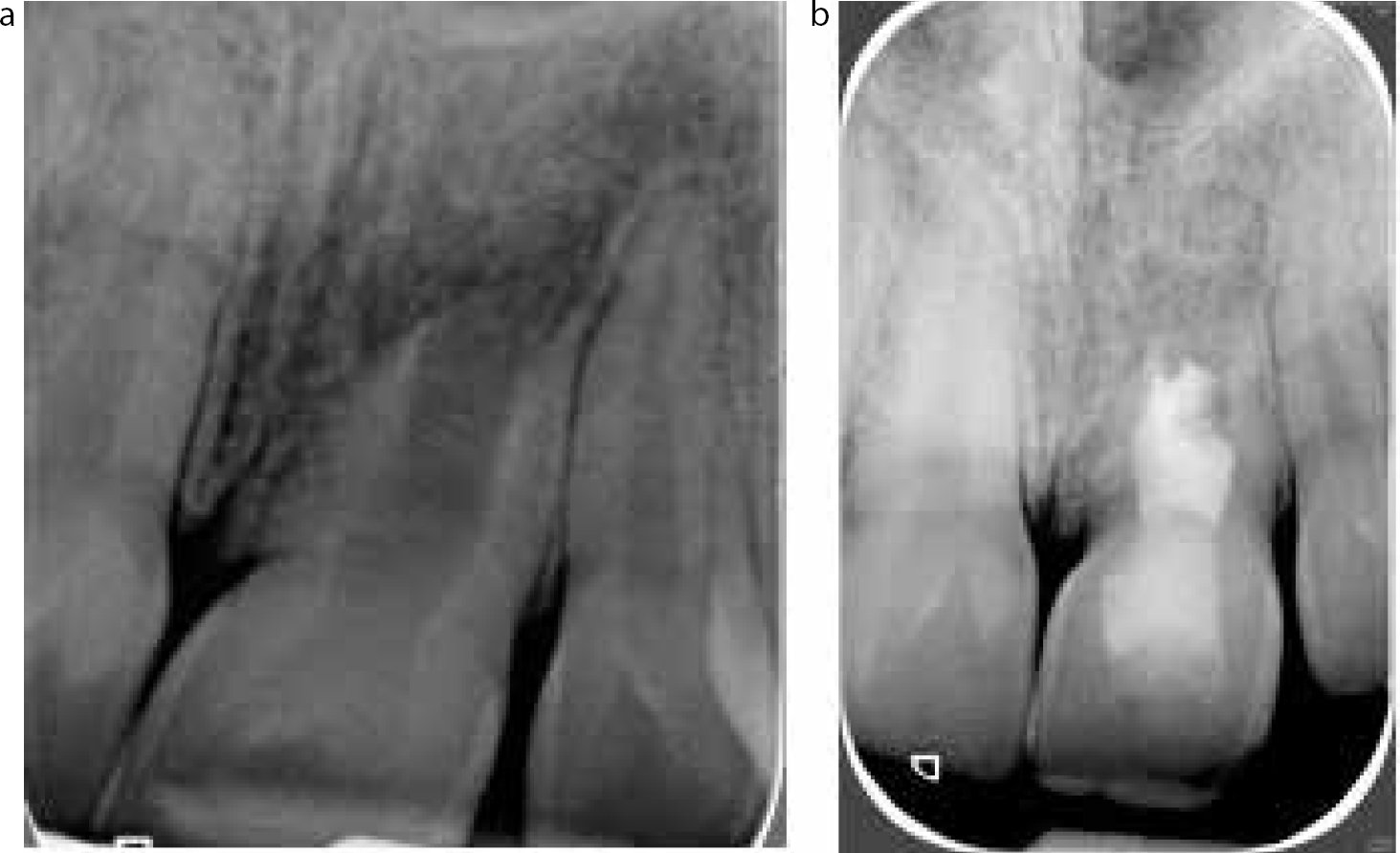
Traumatized immature teeth, with incompletely formed roots and apices, pose two problems. Firstly, the large apical foramen and lack of constriction make it virtually impossible to provide a satisfactory obturation and apical seal with conventional materials. Secondly, incomplete root formation results in thin root walls which are prone to fracture (Figure 10).
Figure 10.
(a, b) The UL1 has incomplete root development following trauma at the age of 8. In this case a regenerative endodontic procedure has been undertaken. The radiograph on the right is at 3 months and there is evidence of healing.
A relatively new treatment paradigm which aims to address both issues has been termed ‘regenerative endodontic procedures’ (REP). This approach has been described as ‘biologically based procedures designed to replace damaged structures, including dentine and root structures, as well as cells of the pulp-dentine complex’.16 Such techniques aim to stimulate continued root formation, resulting in both thickening of the root walls and maturation of the apical region. These treatments utilize the principles of tissue engineering in order to bring about continued root development and the re-introduction of vital tissue into the root canal space. In order for this to occur, three components need to be present; stem cells, a scaffold and growth factors.17
Adult tissues contain sources of multipotent stem cells which are capable of differentiating into different cell types originating from that particular embryonic tissue.18 Tissues such as the dental pulp originate from mesenchyme, and several sources of mesenchymal stem cells have been discovered in the oral cavity.18 One source of these cells exists in the apical papilla which is located immediately below the root apices and is utilized in these procedures. The method by which such cells are introduced into the canal system is by vertically penetrating beyond the root apex with an endodontic file to induce bleeding into the canal space. This not only transports stem cells and growth factors into the canal, but fibrin in the plasma acts as a scaffold for the cells, thus fulfilling the requirements for tissue engineering.
Although several clinical protocols have been employed, there appears to be agreement that disinfection of the canal space before introducing stem cells is of paramount importance. Various concentrations of sodium hypochlorite have been used; however, it is worth bearing in mind that concentrations as high as 6% appear to have a detrimental effect upon stem cell survival.19 Similarly, EDTA has also been advocated owing to its ability to release growth factors from the root dentine.20
The procedure is usually completed over two visits, with an inter-appointment anti-bacterial dressing. Various combinations of antimicrobial agents have been utilized, including ‘triple antibiotic paste’, which consists of metronidazole, minocycline and ciprofloxacin. Owing to tooth discoloration attributed to the use of minocycline, this has been excluded to provide a ‘double paste’. The difficulty of using such medicaments is that only pure forms of the anti-microbial can be used, which are expensive and difficult to acquire. In view of this, some papers have reported the use of calcium hydroxide paste, which is widely available.21
Although endodontic files are required to determine the working length radiographically, no instrumentation of the canal should be undertaken as this may also have a detrimental effect upon stem cells.18 Coronal seal is also crucial and MTA is used for this. A useful protocol has been developed which can be easily undertaken in general practice (Figures 10 and 11 and Table 1).21
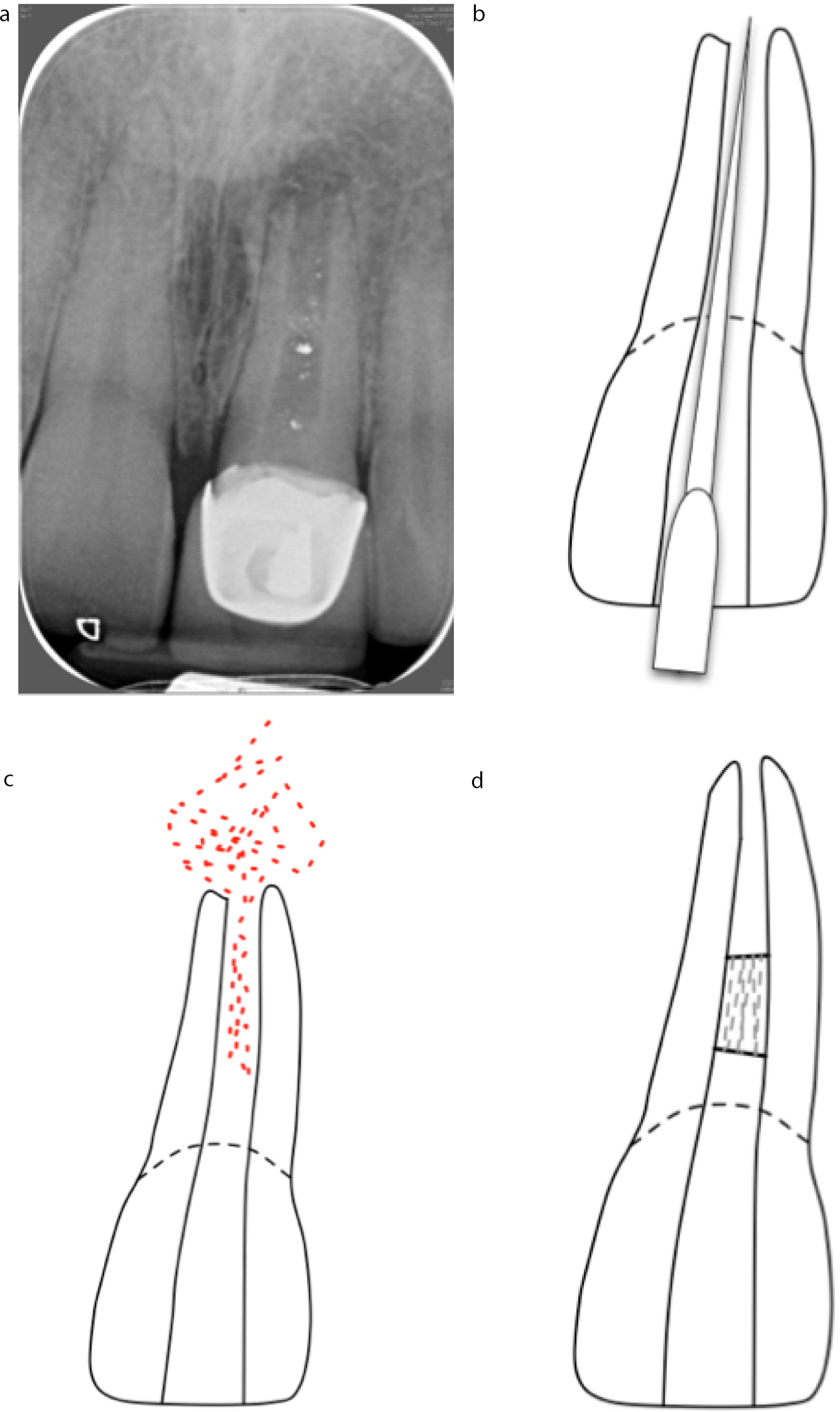
Figure 11.
(a–d) Following 3 weeks of disinfection with Ca(OH)2 the apex is instrumented until there is bleeding in the canal. A barrier is placed and the tooth left: ideally there will be continued root development.
Initial visit
Under rubber dam, access the canal and determine working length radiographically
Irrigate with 20 ml of 1.5% NaOCl followed by saline
Dress with CaOH and place a good coronal seal
Second visit (3 weeks later)
If the tooth has been asymptomatic, administer LA without vasoconstrictor, if not repeat visit one
Irrigate with copious amounts of EDTA (17%) then dry the canal
Measure 4 mm below the CEJ
Induce bleeding by placing a K file 2 mm beyond the foramen
Once blood has filled the canal to 4 mm below the CEJ, place a collagen sponge to this length
Pack a 3 mm plug of white MTA to 1 mm below the CEJ
Place a thick layer of GIC over this and restore the tooth with composite resin
Review at 3 and 6 months, and every year for 4 years
The evidence base for regenerative endodontic procedures is growing, but is currently limited to case series and reports which use a variety of clinical protocols. Studies have also discovered some practical issues and unwanted side-effects of these procedures. It may be difficult to induce satisfactory bleeding into the canal; therefore use of local anaesthetic without vasoconstrictor is advised.22 Tooth discoloration can occur due to the triple antibiotic paste or MTA. For this reason, it is advisable to terminate the MTA plug below the level of the cemento-enamel junction. Unusual morphology of the developing root has also been reported, which is thought to be due to damage of Hertwig's epithelial root sheath during laceration of the apical papilla.23 Other authors have found obliteration of the canal space, whereas some have reported no increase in root length or wall thickness.24 Histological examination of teeth that have undergone REP shows that true regeneration may not actually be occurring. These, and the lack of robust evidence for these procedures, highlight the importance of informed consent. Despite this, with improvements in technology and our understanding of the principles underpinning such procedures, regenerative endodontics holds great promise for the future.
Intentional replantation
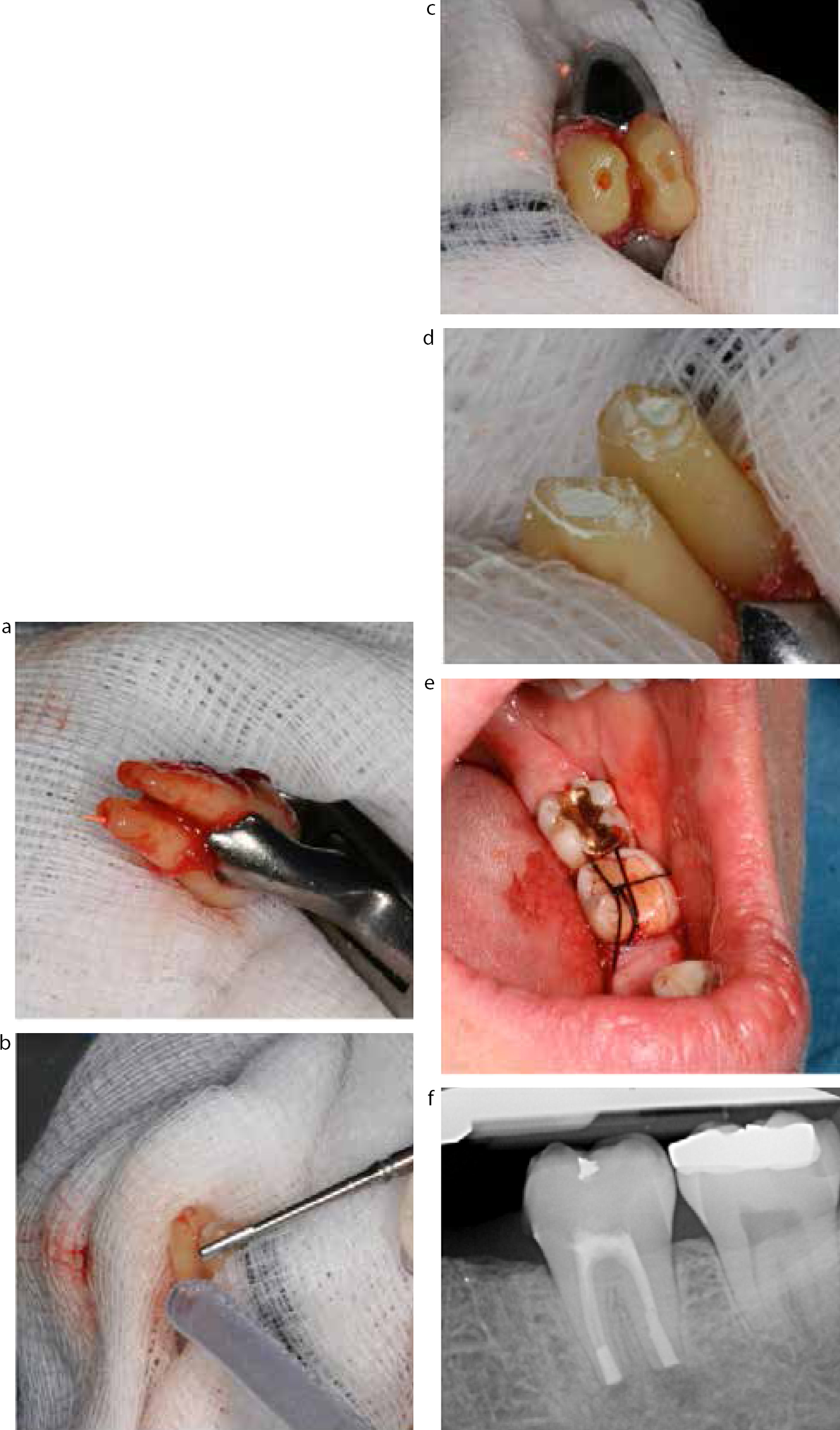
When surgical access is limited or surgery carries increased risk to the nearby anatomical structures, intentional replantation can prove to be a sensible option. In this method the tooth is extracted, apical surgery is performed outside the mouth and the tooth is replanted back in position (Figure 12). Mandibular second molars are an example of suitable teeth for this procedure due to their proximity to the inferior alveolar nerve, difficulty to access, as well as the thick cortical bone covering their roots; however, this technique can be done on any other tooth.
Contra-indications for this type of surgery include the presence of divergent roots or moderate curvature. Root fracture used to be another contra-indication; however, there is growing evidence to suggest that this technique can be used to repair fractured roots with resin with a 5-year success of 60%.25 The two important prognostic factors in this technique are the atraumatic surgery as well as the minimal extra-oral time, as these two factors have a great influence on the survival of the cells in the periodontal ligament and cementum.26
In this technique the tooth is extracted with minimal trauma, the root surface is kept moist using sterile gauze soaked in a physiologic solution and the root-end resected, prepared and filled. The tooth is then replanted and the buccal bone is compressed. The patient may bite on a cotton roll to help position the tooth back in the socket. The choice of splinting is optional but often not necessary. The occlusion is checked and adjusted to allow very minimal load on the tooth. Soft diet and avoiding sticky foods is mandatory for 7–10 days post-operatively (Figure 13).
Figure 13.
(a–f) Intentional replantation of LL7: atraumatic extraction, root amputation, preparation and obturation with MTA followed by replacement and a stabilizing suture. The procedure took less than 15 minutes. Note the careful handling of the roots: the tooth never leaves the forceps. Images courtesy of Dr J Cunliffe.
Conclusions
The preservation of pulpal health should be the fundamental principal of treatment. When pulpal health has been compromised irreversibly, the dentist must work to preserve periapical health. Materials that can promote healing and techniques that revascularize non-vital teeth may redefine our understanding of operative dentistry. We are entering an exciting era in endodontics.