Boufdil H, Mtalsi M, El Arabi S, Bousfiha B Apexification with calcium hydroxide vs. revascularization. Case Rep Dent. 2020; 2020 https://doi.org/10.1155/2020/9861609
Witherspoon DE, Small JC, Regan JD, Nunn M Retrospective analysis of open apex teeth obturated with mineral trioxide aggregate. J Endod. 2008; 34:1171-1176 https://doi.org/10.1016/j.joen.2008.07.005
Steinig TH, Regan JD, Gutmann JL The use and predictable placement of mineral trioxide aggregate in one-visit apexification cases. Aust Endod J. 2003; 29:34-42 https://doi.org/10.1111/j.1747-4477.2003.tb00496.x
El-Meligy OA, Avery DR Comparison of apexification with mineral trioxide aggregate and calcium hydroxide. Pediatr Dent. 2006; 28:248-253
Songtrakul K, Azarpajouh T, Malek M Modified apexification procedure for immature permanent teeth with a necrotic pulp/apical periodontitis: a case series. J Endod. 2020; 46:116-123 https://doi.org/10.1016/j.joen.2019.10.009
Fahl N, Ritter AV Composite veneers: the direct-indirect technique revisited. J Esthet Restor Dent. 2021; 33:7-19 https://doi.org/10.1111/jerd.12696
AlSaeed T, Nosrat A, Melo MA Antibacterial efficacy and discoloration potential of endodontic topical antibiotics. J Endod. 2018; 44:1110-1114 https://doi.org/10.1016/j.joen.2018.03.001
Swaikat M, Faus-Matoses I, Zubizarreta-Macho Á Is revascularization the treatment of choice for traumatized necrotic immature teeth? a systematic review and meta-analysis. J Clin Med. 2023; 12 https://doi.org/10.3390/jcm12072656
Liang Y, Ma R, Chen L Efficacy of i-PRF in regenerative endodontics therapy for mature permanent teeth with pulp necrosis: study protocol for a multicentre randomised controlled trial. Trials. 2021; 22 https://doi.org/10.1186/s13063-021-05401-7
Tang Q, Jin H, Lin S Are platelet concentrate scaffolds superior to traditional blood clot scaffolds in regeneration therapy of necrotic immature permanent teeth? A systematic review and meta-analysis. BMC Oral Health. 2022; 22 https://doi.org/10.1186/s12903-022-02605-4
Balkaya H, Topçuoğlu HS, Demirbuga S Effect of different coronal restorations on the fracture resistance of teeth with simulated regenerative endodontic treatment: an in vitro study. Aust Endod J. 2022; 48:331-337 https://doi.org/10.1111/aej.12573
Fadag A, Negm M, Samran A Fracture resistance of endodontically treated anterior teeth restored with different post systems: an in vitro study. Eur Endod J. 2018; 3:174-178 https://doi.org/10.14744/eej.2018.70299
Immature necrotic permanent teeth with a significant amount of coronal hard tissue loss are treated by apexification procedures. These procedures do not encourage further root maturation, predisposing the teeth to possible root fractures. The modified apexification procedure simulates regenerative endodontic procedures in encouraging root development in terms of increased dentine thickness contributing to improved resistance to fracture, while allowing the canal space to be used for core retention. This case report presents an immature tooth treated by the modified apexification procedure with an 18-month follow-up.
CPD/Clinical Relevance: An alternative therapy in managing immature necrotic permanent teeth is of relevance to clinicians.
Article
Immature permanent teeth with necrotic pulps may be a challenge to treat because of their thin dentinal walls, shortened roots, and open apices, which could result in the extrusion of root-filling material into the peri-apical tissues.1 Such teeth are often managed by apexification, a method employed to induce an apical barrier in necrotic teeth with incompletely formed roots. Various bio-ceramic materials have been used to create an apical calcified tissue barrier.
Calcium hydroxide apexification is no longer routinely employed to manage open apices because of prolonged treatment time, further weakening of tooth structure and unpredictability of the calcified barrier formed.1 Mineral trioxide aggregate allows single-visit apexification with the formation of a reliable calcified barrier.2,3 These procedures do not encourage further root maturation, predisposing the root to fracture. Hence, regenerative endodontic procedures must ideally be employed for immature necrotic permanent teeth.4 Teeth with significant coronal tooth tissue loss may require the canal space for post retention and might not be ideal candidates for regenerative procedures.5 In such teeth, the modified apexification procedure may be employed. This includes placement of a collagen sponge in the apical one-third followed by 3–4 mm of MTA/Biodentine (Septodont, Saint-Maur-des-Fossés, France) to prevent extrusion into peri-apical tissues. The remainder of the canal space can serve for core retention.6
Case report
A 13-year-old boy reported to the clinic with a chief complaint of fractured maxillary anterior teeth. His medical and family history was non-contributory. Extra-oral findings were unremarkable. Clinical examination revealed the presence of an Ellis Class III fracture of maxillary left and right central incisors (UR1 and UL1). The teeth were slightly tender to percussion, and poor oral hygiene was noted (Figure 1). However, there were no associated periodontal findings. The teeth were non-responsive to pulp sensitivity tests, while the adjacent teeth responded within normal limits. A sinus opening was seen in relation to UR1 (Figure 1).
Figure 1. Pre-operative intra-oral photograph.
Intra-oral peri-apical radiographs revealed the presence of ill-defined radiolucencies associated with the immature apices of UR1 and UL1 (Figure 2).
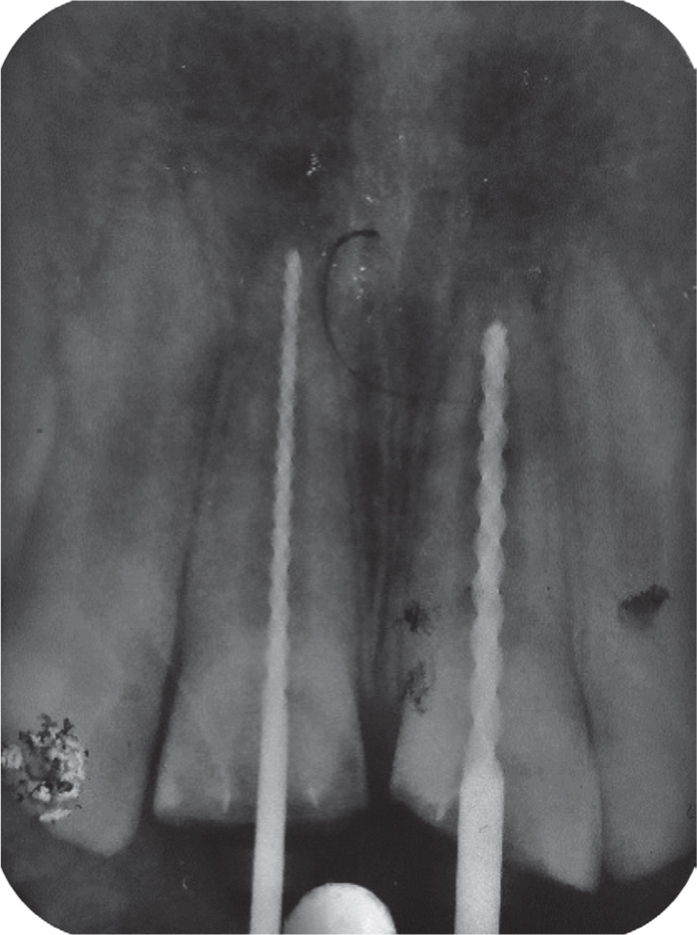
At the first visit, under local anaesthesia (2% lidocaine with 1:80,000 epinephrine) (Lignox 2%, Indoco Remedies Ltd, India) and rubber dam isolation, access openings were made for UR1 and UL1 and the root canals were irrigated using 20 ml of 1% sodium hypochlorite solution, delivered with a side-vented needle for 5 minutes. The working length was measured using hand files, and confirmed radiographically (Figure 3).
Figure 3. Working length determination.
Chemo-mechanical debridement was carried out by minimal circumferential filing and copious irrigation with 1% sodium hypochlorite. The canal was dried using absorbent paper points and then dressed with double antimicrobial paste (metronidazole and ciprofloxacin in a 1:1 ratio) carried in a propylene glycol vehicle for 3 weeks.
At the second visit, since the teeth were asymptomatic, the access cavities were re-opened under rubber dam isolation and the medicament was removed using 10 ml of 1% sodium hypochlorite and 5 ml of saline delivered through a 30-gauge side-vented needle. To ensure complete removal of the medicament and smear layer, a final rise of 1 mL 17% EDTA (MD Cleanser, Meta Biomed, India) was agitated with a sonic activator (Sonic Flush Endo Irrigator, SuperEndo, Canada) for 1 minute.
In UR1, MTA apexification was carried out, while modified apexification treatment was performed for UL1. Informed consent was obtained from the patient's parents.
Apexification of UR1
A 4-mm MTA plug (Bio-C Repair, MTA Angelus, India) was formed as an apical barrier. The remaining canal space was coated with resin sealer (AH Plus, Dentsply Sirona, India) and backfilled with thermo-plasticized gutta percha to 3 mm below the cementoenamel junction.
Modified apexification for UL1
To prepare injectable platelet rich fibrin (i-PRF), 10 ml of whole blood from the median cubital vein was drawn into a 10 ml plastic tube (Kangjian Medical, Jiangsu, China) without anticoagulant reagent and centrifuged at 800 rpm for 3 minutes. After centrifugation, the upper yellow liquid (i-PRF) was syringed as close as possible to the layer of red cells. A resorbable collagen sponge (Dengen Dengofoam, India) was placed in the apical third of the root canal following which, 1 ml of i-PRF was syringed onto it. Biodentine (Septodont) was placed as an apical barrier over the collagen sponge up to 5 mm from the cemento-enamel junction, following which a glass ionomer cement barrier was placed (Figure 4).
Figure 4. Apexification for UR1 and modified apexification for UL1.
Since the patient did not attend for further treatment until 6 months later, post-endodontic restoration was delayed. The remaining canal walls were coated with a bonding agent. Ribbond (Ribbond Inc, USA) wallpapered over the canal walls and extended into the coronal access cavity to aid composite retention. For financial reasons, direct composite veneers were planned. Tooth preparation was done to establish a chamfer finish line of 1–1.5 mm.7 To mask the discolouration of the teeth, a thin layer of opaquer (Universal Opaque, Shofu, India) was applied, and composite layering was carried out. Homogeneity of thickness in the layering of opaquer and dentine shades of composite are critical in achieving a uniform shade that masks the underlying discolouration. The composites were finished using diamond points (TR-12, Mani, Japan), and polishing was carried out using abrasive discs (Shofu Super Snap Kit, Shofu) (Figure 5).
Figure 5. Immediate post-endodontic restoration.
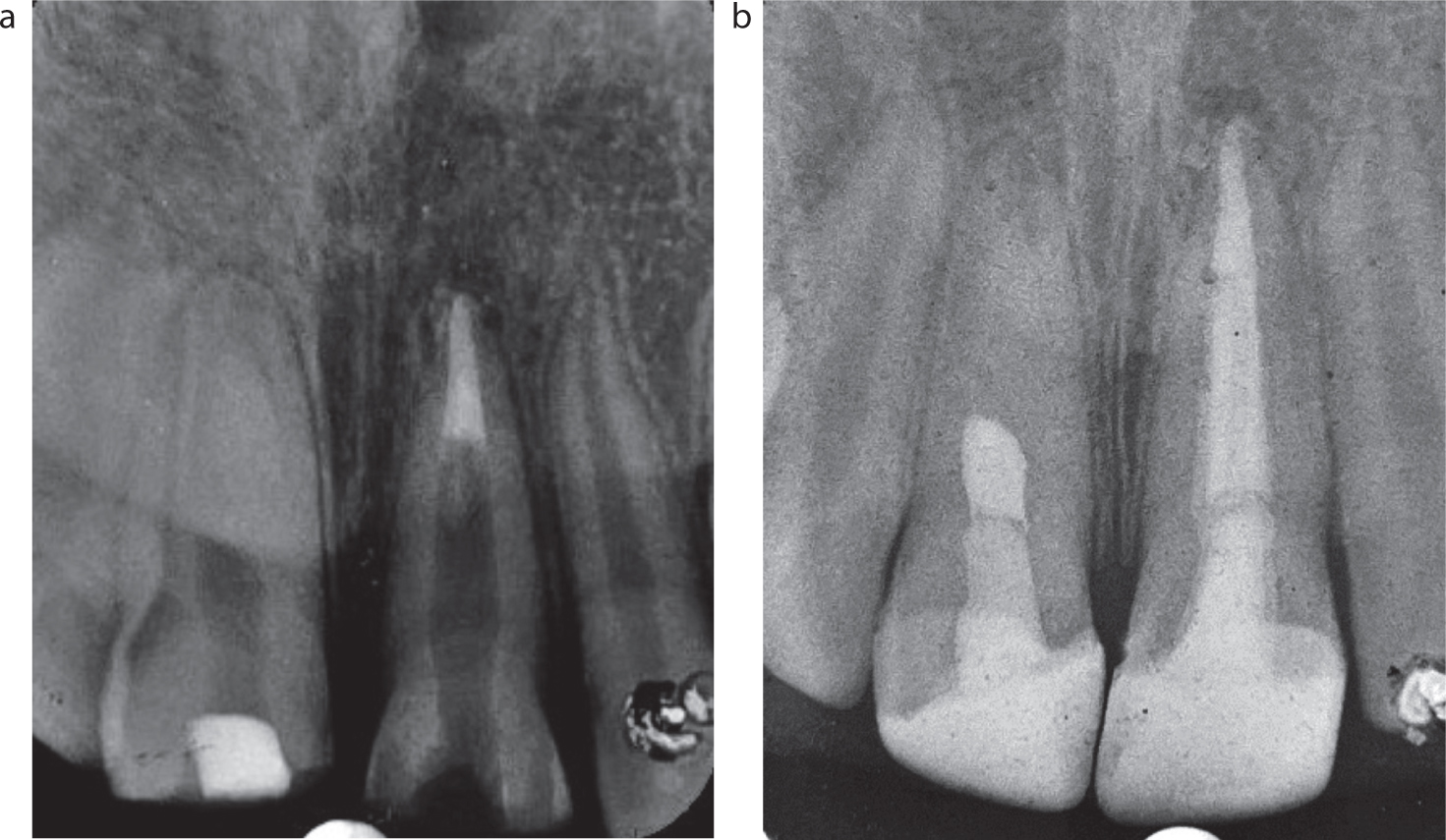
The patient was reviewed at 1, 3, 6, 12 and 18 months for follow-up. At follow-up visits, the patient remained asymptomatic, radiographs showed resolution of peri-apical radiolucency, initiation of formation of calcific barrier with re-establishment of lamina dura (Figure 6).
Figure 6. Radiographs taken at the (a) 6-month and (b) 12-month follow-ups.
Discussion
Hertwig's epithelial root sheath cells are primarily responsible for root development. However, in long-standing infections, pro-inflammatory cytokines, such as interleukin-1 and tumour necrosis factor-alpha, released from immuno-inflammatory cells cause damage to the apical stem cells, leading to an arrest in further root development. A potential for continued root development through repair exists if the canal infection and peri-apical inflammation is controlled by antibacterial strategies.6
In this case, canal disinfection was achieved using copious irrigation with a lower concentration sodium hypochlorite and double antibiotic paste where equal portions of metronidazole 400 mg and ciprofloxacin 500 mg were mixed in a 1:1 ratio with propylene glycol, to obtain a concentration of 0.1 mg/ml, which was used as an intra-canal medicament for 3 weeks, until symptoms subsided. Double antibiotic paste was preferred over triple antibiotic paste and calcium hydroxide to preclude any possibility of tooth discolouration arising from the minocycline component of triple antibiotic paste, and weakening of the root dentine from long-term calcium hydroxide in these immature anterior teeth.8,9
Since there was significant loss of tooth structure, which would require an intra-radicular post for retention of a coronal restoration, regenerative endodontic treatment was not considered and modified apexification was performed.6 A conventional apexification procedure was modified to allow the placement of a collagen sponge with injectable PRF, which served as a scaffold or reservoir. This was mainly employed to allow an increase in root length and thickness, which might enhance tooth strength from the increased crown:root ratio. Platelet products have shown great potential in regenerative medicine because of their potency in storing and releasing biologically active substances, regulating the innate immune response, and combating infection. Injectable PRF or i-PRF was introduced into endodontics in 2004.10 This is known to be a superior reservoir of stem cells and growth factors. Being injectable, they are superior to PRF in having a greater potential for growth factor release over a longer period, while overcoming the limitations of a solid PRF matrix.11 This would serve as a potential scaffold for maturation factors and stem cells, enhancing root maturation.10
Since the cervical third of the root is the weakest region and prone to fractures, fibre-reinforced composites, such as Ribbond, were chosen as an alternative to fibre posts. These are known to significantly improve the fracture resistance of immature teeth and hence, were adopted in this case for the retention of the coronal restoration.12,13 Direct composite veneers were constructed for UR1 and UL1 because they are minimally invasive and can provide good aesthetics.
In the follow-up radiographs, there was continued root development with a blunt apex and a partially obliterated apical canal space. This is an indication that tissue forming cells had migrated into the canal space to form mineralized tissue. Initiation of apical closure was also seen, which could be from the viable Hertwig's epithelial root sheath (HERS) and apical papilla cells that survived following effective canal space disinfection with low-concentration NaOCl and double antibiotic paste.14 In UR1 treated with a conventional apexification procedure, no barrier formation or further root maturation was seen. Various factors, such as greater healing ability with more stem cell regenerative potential in young patients, could have helped achieve a favourable result. Furthermore, minimal canal instrumentation with thorough disinfection could have preserved viable HERS cells and stem cells of the apical papilla, which then differentiate into primary odontoblasts to complete root formation.14
In conclusion, regenerative endodontics remains the mainstay treatment modality in the management of immature necrotic permanent teeth. However, a modified apexification procedure could be adopted as an alternative to regenerative procedures in necrotic immature permanent teeth requiring canal space for a coronal restoration.