Bjorndal L, Laustsen MH, Reit C. Root canal treatment in Denmark is most often carried out in carious vital molar teeth and retreatments are rare. Int Endod J. 2006; 39:785-790
Swift Jr EJ, Trope M, Ritter AV. Vital pulp therapy for the mature tooth – can it work?. Endod Topics. 2004; 5:49-56
Kebke S, Fransson H, Brundin M Tooth survival following root canal treatment by general dental practitioners in a Swedish county – a 10-year follow-up study of a historical cohort. Int Endod J. 2021; 54:5-14
Bernstein SD, Horowitz AJ, Man M Outcomes of endodontic therapy in general practice: a study by the Practitioners Engaged in Applied Research and Learning Network. J Am Dent Assoc. 2012; 143:478-487
Gilbert GH, Tilashalski KR, Litaker MS Outcomes of root canal treatment in dental practice-based research network practices. Gen Dent. 2010; 58:28-36
Bjorndal L, Simon S, Tomson PL Management of deep caries and the exposed pulp. Int Endod J. 2019; 52:949-973
Duncan HF, Galler KM, Tomson PL European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int Endod J. 2019; 52:923-934
Smith AJ, Cassidy N, Perry H Reactionary dentinogenesis. Int J Dev Biol. 1995; 39:273-280
Randow K, Glantz PO. On cantilever loading of vital and non-vital teeth. An experimental clinical study. Acta Odontol Scand. 1986; 44:271-277
Stanley HR. Pulp capping: conserving the dental pulp – can it be done? Is it worth it?. Oral Surg Oral Med Oral Pathol. 1989; 68:628-639
Schwendicke F, Stolpe M. Direct pulp capping after a carious exposure versus root canal treatment: a cost-effectiveness analysis. J Endod. 2014; 40:1764-1770
Taha NA, Khazali MA. Partial Pulpotomy in Mature Permanent Teeth with Clinical Signs Indicative of Irreversible Pulpitis: A Randomized Clinical Trial. J Endod. 2017; 43:1417-1421
Sonmez D, Duruturk L. Ca(OH)2 pulpotomy in primary teeth. Part I: internal resorption as a complication following pulpotomy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106:e94-98
Sjogren U, Hagglund B, Sundqvist G Factors affecting the long-term results of endodontic treatment. J Endod. 1990; 16:498-504
Ng YL, Mann V, Rahbaran S Outcome of primary root canal treatment: systematic review of the literature – part 1. Effects of study characteristics on probability of success. Int Endod J. 2007; 40:921-939
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011; 44:583-609
Friedman S, Abitbol S, Lawrence HP. Treatment outcome in endodontics: the Toronto Study. Phase 1: initial treatment. J Endod. 2003; 29:787-793
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011; 44:610-625
Ng YL, Mann V, Gulabivala K. Tooth survival following non-surgical root canal treatment: a systematic review of the literature. Int Endod J. 2010; 43:171-189
Tronstad L, Mjor IA. Capping of the inflamed pulp. Oral Surg Oral Med Oral Pathol. 1972; 34:477-485
Bjorndal L, Reit C, Bruun G Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci. 2010; 118:290-297
Barthel CR, Rosenkranz B, Leuenberg A Pulp capping of carious exposures: treatment outcome after 5 and 10 years: a retrospective study. J Endod. 2000; 26:525-528
Baume LJ, Holz J. Long term clinical assessment of direct pulp capping. Int Dent J. 1981; 31:251-260
Guideline on Pulp Therapy for Primary and Immature Permanent Teeth. Pediatr Dent. 2016; 38:280-288
Endodontic Diagnosis. Endodontics Colleagues for Excellence. 2013; 1-6
Bogen G, Kim JS, Bakland LK. Direct pulp capping with mineral trioxide aggregate: an observational study. J Am Dent Assoc. 2008; 139:305-315
Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 2011; 37:581-587
Asgary S, Eghbal MJ, Fazlyab M Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority multicenter randomized clinical trial. Clin Oral Investig. 2015; 19:335-341
Taha NA, Ahmad MB, Ghanim A Assessment of Mineral Trioxide Aggregate pulpotomy in mature permanent teeth with carious exposures. Int Endod J. 2017; 50:117-125
Ricucci D, Siqueira JF, Li Y Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J Dent. 2019; 86:41-52
Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol. 1963; 16:846-871
Mejare IA, Axelsson S, Davidson T Diagnosis of the condition of the dental pulp: a systematic review. Int Endod J. 2012; 45:597-613
Dummer PM, Hicks R, Huws D. Clinical signs and symptoms in pulp disease. Int Endod J. 1980; 13:27-35
Ricucci D, Loghin S, Siqueira JF. Correlation between clinical and histologic pulp diagnoses. J Endod. 2014; 40:1932-1939
Cox CF, Bergenholtz G, Fitzgerald M Capping of the dental pulp mechanically exposed to the oral microflora – a 5 week observation of wound healing in the monkey. J Oral Pathol. 1982; 11:327-339
Mohammadi Z, Dummer PM. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J. 2011; 44:697-730
Hilton TJ, Ferracane JL, Mancl L Comparison of CaOH with MTA for direct pulp capping: a PBRN randomized clinical trial. J Dent Res. 2013; 92:16S-22S
Cox CF, Bergenholtz G, Heys DR Pulp capping of dental pulp mechanically exposed to oral microflora: a 1–2 year observation of wound healing in the monkey. J Oral Pathol. 1985; 14:156-168
Bakland LK, Andreasen JO. Will mineral trioxide aggregate replace calcium hydroxide in treating pulpal and periodontal healing complications subsequent to dental trauma? A review. Dent Traumatol. 2012; 28:25-32
Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review. Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010; 36:400-413
Parirokh M, Torabinejad M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part I: vital pulp therapy. Int Endod J. 2018; 51:177-205
Taha NA, About I, Sedgley CM Conservative management of mature permanent teeth with carious pulp exposure. J Endod. 2020; 46:S33-S41
Aeinehchi M, Eslami B, Ghanbariha M Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: a preliminary report. Int Endod J. 2003; 36:225-231
Asgary S, Eghbal MJ, Bagheban AA. Long-term outcomes of pulpotomy in permanent teeth with irreversible pulpitis: a multi-center randomized controlled trial. Am J Dent. 2017; 30:151-155
Galani M, Tewari S, Sangwan P Comparative evaluation of postoperative pain and success rate after pulpotomy and root canal treatment in cariously exposed mature permanent molars: a randomized controlled trial. J Endod. 2017; 43:1953-1962
Taha NA, Abdelkhader SZ. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int Endod J. 2018; 51:819-828
Taha NA, Abdulkhader SZ. Full pulpotomy with Biodentine in symptomatic young permanent teeth with carious exposure. J Endod. 2018; 44:932-937
Asgary S, Hassanizadeh R, Torabzadeh H Treatment outcomes of four vital pulp therapies in mature molars. J Endod. 2018; 44:529-535
Whitworth JM, Seccombe GV, Shoker K Use of rubber dam and irrigant selection in UK general dental practice. Int Endod J. 2000; 33:435-441
Edwards D, Bailey O, Stone S The management of deep caries in UK primary care: a nationwide questionnaire-based study. Int Endod J. 2021; 00:1-15 https://doi.org/10.1111/iej.13585
Ireland L. The rubber dam – its advantages and application. Tex Dent J. 1962; 80:6-15
Lin LM, Ricucci D, Saoud TM Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust Endod J. 2020; 46:154-166
Vital pulp therapy (VPT) aims to preserve pulpal sensation. Historically VPT was considered a treatment option for deciduous teeth or young immature permanent teeth. Carious pulp exposure in permanent mature teeth was considered a contraindication for VPT and warranted root canal treatment (RCT). Recently, VPT has been used for management of carious pulp exposures in mature permanent teeth, with good outcomes, even in the presence of clinical signs and symptoms suggestive of irreversible pulpitis. VPT is a simple and conservative alternative to root canal treatment in a few clinical situations. It is imperative that dentists understand its indications and techniques.
CPD/Clinical Relevance: The reader should understand the evidence-based changes in approach to VPT and the future direction of this treatment modality.
Article
Conventionally, when a mature permanent tooth has been compromised by caries, and pulp exposure is inevitable, traditional treatment would be in the form of pulp extirpation and root canal treatment (RCT) before restoring the tooth to function and aesthetics.1 This approach is underpinned by the acceptance that the cariously exposed pulp is irreversibly damaged even after removal of the noxious stimulus.2 However, RCT can be challenging and requires both clinical training and the use of dedicated equipment, particularly in the case of multi-rooted teeth. Heavily restored molar teeth, complex anatomy, curved and narrow canals, long and thin roots and difficult access to posterior teeth may make conventional root canal treatment challenging.3 Cross-sectional studies have demonstrated suboptimal outcomes for root canal treatment provided by general dental practitioners (GDPs).4–6 Therefore, a treatment option to successfully manage deep caries and carious pulp exposure that is conservative, appropriate for primary care and demonstrates a favourable outcome would be welcomed.
VPT procedures, advantages and disadvantages over RCT
Vital pulp therapy (VPT) is a biologically based concept that aims to preserve all or part of the pulp that has been compromised by caries or trauma.7 Techniques range from application of a biomaterial placed over a thin dentine barrier to prevent pulp exposure (indirect pulp capping) (Figure 1), capping the exposed pulp directly with a biomaterial intended to stimulate healing (direct pulp capping), or partial or full removal of the coronal pulp followed by capping the remaining pulp with a biomaterial intended to promote healing (partial and full pulpotomy, respectively) (Figures 2 and 3).8 By preserving the vital pulp in a healthy condition, the sensory mechanism of the tooth (thermal, nociception and proprioception) is preserved, its ability to secrete secondary and tertiary dentine is maintained and root development can continue.9,10 VPT is technically easier to perform than RCT11 and may prove to be more cost-effective.12 It does not require specialist training and is manageable in primary care. It also satisfies the minimal intervention concept.7
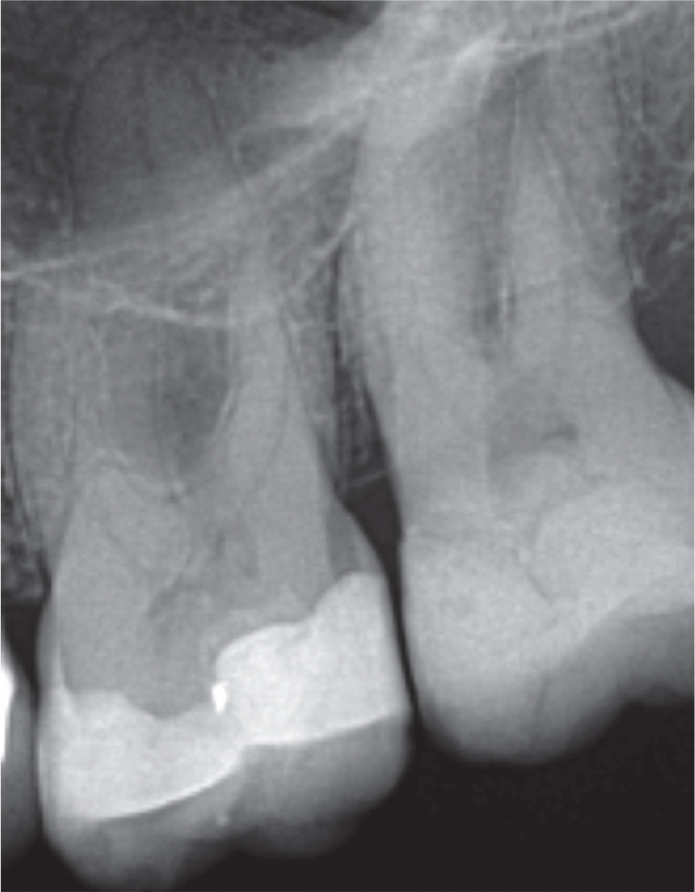
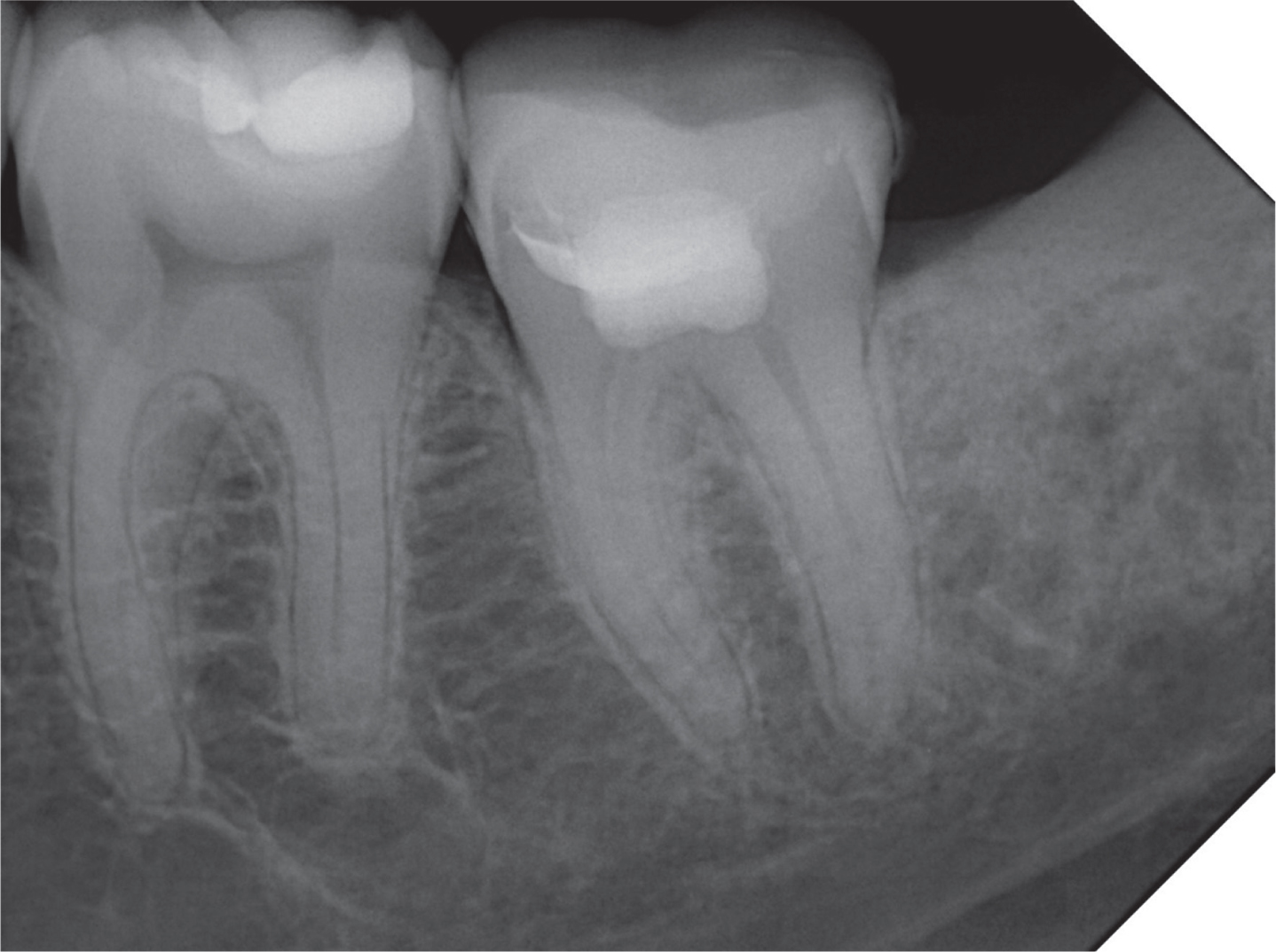
Figure 1. Indirect pulp capping of teeth LL6 and LL7 using Biodentine. (a) The patient presented with sensitivity to hot and cold drinks in her lower left quadrant. A diagnosis of reversible pulpitis with normal apical tissues in teeth LL5, LL6 and LL7 was made after clinical and radiographic examination. (b, c) Defective restorations were removed under rubber dam isolation. No pulp exposure was encountered. (d) LL6 and LL7 were restored with Biodentine. (e, f) After 1 week, the cavities were prepared under rubber dam isolation, leaving a lining of Biodentine to protect the pulps. (g) Definitive composite restorations were placed. After 1 year, the patient was symptom free, and all three teeth responded normally to cold testing, with no tenderness to palpation or percussion. (h) The peri-apical radiograph showed no signs of apical pathology.Figure 2. A 6-year follow-up radiograph after partial pulpotomy with Biodentine. The patient originally presented with signs and symptoms suggestive of irreversible pulpitis with a distinct distobuccal pulp horn exposure upon caries excavation. After 6 years, the patient presented with no symptoms, a normal response to vitality testing and no tenderness to percussion.Figure 3. A 1-year follow-up peri-apical radiograph of LL7, which had received an MTA full pulpotomy owing to signs and symptoms suggestive of irreversible pulpitis. On the review appointment, the patient presented with no symptoms or tenderness to palpation or percussion. The tooth was functional, but there was no response to cold or electric stimulation.
However, if the VPT procedure fails, the patient may experience pain and/or infection.13 Root canal treatment may become more difficult to perform following failed VPT as the remaining pulp space may undergo varying levels of mineralization or root resorption.14 Furthermore, if VPT failure is not detected in a timely manner, the pulp space may become heavily infected and the subsequent RCT will have a reduced prognosis.12,15 Therefore, the decision to perform a VPT procedure must be made after thorough assessment of all the prognostic factors, and its advantages and disadvantages explained and discussed with the patient. Once carried out, appropriate and timely follow up is recommended to avoid complications associated with failure.
VPT between the past and the present: outcomes and indications
Root canal treatment is a well-established treatment modality with success rates of up to 83–92% when performed on teeth without peri-apical lesions,16–18 and a survival rate of 86–97%.19,20
Until the early 21st century, studies on VPT reported poor outcomes.21 Bjorndal et al used calcium hydroxide paste to treat carious pulp exposures and reported a 31.9% and 34.5% success rate related to direct capping and partial pulpotomy, respectively.22 In a retrospective study of carious pulp exposures, direct pulp capping was reported to have a success rate of 37% and 13% after 5 and 10 years, respectively.23
Carious pulp exposure has been considered a contraindication for VPT.24 The American Association of Endodontists and the American Academy of Pediatric Dentistry recommended VPT for treating either primary teeth, or permanent teeth with immature apices with mechanical or traumatic pulp exposure of healthy or reversibly inflamed pulps.25,26 Mature permanent teeth with carious pulp exposure or a clinical diagnosis of irreversible pulpitis were considered to be appropriate for root canal treatment.25,26
In 2003, a review article discussed the possibility of performing VPT on mature permanent teeth.2 The recommendations were that pulp capping can be performed on recent (<24 h) traumatic or mechanical non-carious exposures during cavity preparation, and that mature teeth with inflamed pulps, as with carious pulp exposures, should not be pulp capped.
In 2008, Bogen et al reported a success rate of 98% after 9 years of direct capping of cariously exposed pulps using mineral trioxide aggregate (MTA).27 Despite the limitations of this study, it was among the first to report a favourable outcome for VPT on cariously exposed pulps in mature permanent teeth. Having said that, the pre-operative diagnosis was to be ‘no more than reversible pulpitis’. Multiple reports and clinical studies have been performed thereafter on the outcome of VPT. In 2011, a systematic review was published on VPT in mature permanent teeth with cariously exposed pulps. It was concluded that teeth with carious exposure should not always be diagnosed as having irreversible pulpitis and, therefore, requiring a pulpectomy.28 In 2015, Asgary et al published the results of a randomized clinical trial comparing pulpotomy and root canal treatment for management of mature permanent teeth diagnosed clinically with symptomatic irreversible pulpitis.29 They reported a similar outcome for both treatment options after a 5-year follow-up period. In 2017, Taha et al reported a success rate of 93% after 3 years for MTA coronal pulpotomy in mature permanent teeth with carious exposures and signs and symptoms of irreversible pulpitis.30 In the same year, Taha et al demonstrated a higher success rate for MTA partial pulpotomy compared to that using calcium hydroxide (85% vs 43%, respectively) in mature permanent teeth with carious exposures and signs and symptoms of irreversible pulpitis.13
In 2019, the European Society of Endodontology (ESE) published a position statement regarding management of deep caries and the exposed pulp.8 While summarizing the recommendations of this paper is beyond the scope of the present article, the ESE recommended VPT as an alternative to root canal treatment for management of carious pulp exposure in mature permanent teeth even in the presence of signs and symptoms of irreversible pulpitis if certain conditions are met. Ricucci et al proposed similar guidelines for the conservative management of mature teeth with deep caries based on histopathology. They concluded that VPT can be an alternative to pulpectomy if certain conditions are met.31
So what has changed?
Our understanding of pulp histopathology
Early studies demonstrated a poor correlation between clinical symptoms and the histological status of the pulp.32–34 It was believed that clinical symptoms can only determine the probable state of the pulp.34 Ricucci et al showed that clinical diagnosis matched the histological diagnosis in 96.6% of cases when the histological diagnosis was normal pulp/reversible pulpitis, and in 84.4% of irreversible pulpitis histological diagnoses.35 This study not only showed a ‘good’ correlation between clinical and histological diagnosis, but it also demonstrated that dentists are more likely to make the wrong diagnosis when the clinical situation suggests irreversible pulpitis than when signs and symptoms are indicative of normal pulp/reversible pulpitis. Therefore, dentists are more likely to unnecessarily perform an RCT when the pulp is savable than to opt for VPT when the pulp is unsavable, when relying on the clinical signs and symptoms to determine their treatment. Furthermore, this study demonstrated that pulp pathology occurs in compartments and can vary in severity and stage according to the corono-apical level. Following carious pulp exposure, the most coronal pulp undergoes coagulation and liquefactive necrosis and is colonized by heavy bacterial infection, forming a micro-abscess.35 The extent of the micro-abscess depends on several factors, such as rate of caries progression and time of detection following pulp exposure. If detected early, and the pulp is only partially necrotic, the pulp surrounding the micro-abscess exhibits accumulation of polymorphonuclear leukocytes, macrophages and lymphocytes. Further peripherally, the inflammatory reaction tapers off, and normal pulp tissue can be encountered in the same tooth.35 This means that if the layers of necrotic/infected and severely inflamed pulp could be removed and covered with a biomaterial that allows healing, the remaining pulp can remain healthy and functional. This was supported later by clinical studies that demonstrated high success rates for VPT even in the presence of clinical signs and symptoms suggestive of irreversible pulpitis.13,29,30
The introduction of calcium silicates
For many years, the gold standard material for pulp capping was calcium hydroxide.36 However, calcium hydroxide does degrade over time37 and it provides a poor seal because it has no inherent adhesive properties.38 Moreover, calcific bridges (tertiary dentine) that form following calcium hydroxide capping were shown to exhibit multiple tunnel defects.39,40 These could potentially provide pathways for bacterial microleakage, resulting in inflammatory changes in the pulp.39 This was reflected in clinical studies, which showed discouraging outcomes that tended to decline over time when calcium hydroxide was used as the capping material.21,23
Calcium silicates have been used to cap pulps exposed mechanically or cariously.41 Calcium silicates are bioactive materials that stimulate mineralization and cell differentiation.42 They were shown to have excellent sealing ability and their solubility is minimal.42 They upregulate angiogenesis by releasing dentine matrix components.43 The use of MTA as the capping material results in a milder inflammatory reaction, less hyperaemia and necrosis, and the formation of a thicker reparative dentine bridge compared with calcium hydroxide.44 Recent studies have shown a high success rate for VPT performed using calcium silicates as the capping material.30,45–48
Future recommendations
Simplifying VPT
Partial pulpotomy seems to be the most technically demanding procedure among the range of VPT procedures. The aim is to excise the irreversibly damaged coronal pulp and dress the remaining ‘healthy’ pulp with a biomaterial that promotes pulpal healing. However, it is not easy to determine how much pulp should be excised. The current recommendation is to remove the obviously diseased pulp material (necrotic and or severely inflamed) and to observe the marginal dentine and the excised pulp (under magnification) for its vascularity, presence of yellowish liquefaction, and time needed to achieve haemostasis.8,31 Furthermore, the wound surface area that is created during partial pulpotomy is significantly larger than that created during direct pulp capping or full pulpotomy (at least in molar teeth). Thus, haemostasis can be more challenging and more post-operative pain can be anticipated. It is entirely plausible to suggest that bigger wounds may take longer to heal with more possibility for error and contamination.
A full coronal pulpotomy procedure achieves the same objectives of partial pulpotomy, namely preserving the radicular vital pulp, allowing complete root development (in the immature tooth) and avoiding an unnecessary and potentially difficult RCT while there is a similar success rate to partial pulpotomy.13,30 It has the advantage of being easier to perform and teach, has a better chance of removing the damaged pulp, and results in a smaller wound surface area. Furthermore, it can be performed without the need for magnification, which is often missing in the primary dental care setting. The obvious disadvantage of full pulpotomy could be the loss of sensation to thermal stimulation, although this is not absolute.
Therefore, to simplify VPT, the authors suggest dividing the exposed inflamed pulps into three categories:
Minimally inflamed pulp that is expected to heal after capping with a bioactive material. This category includes pulps that were traumatically exposed or where contamination is minimal. DPC is the recommended treatment.
Moderately inflamed pulp that is expected to heal following excision of part of the irreversibly damaged coronal pulp. This category involves carious pulp exposures where infection of the exposed pulp and formation of a micro-abscess is inevitable. A full coronal pulpotomy provides a better chance of excising the damaged pulp and, possibly, a better coronal seal (compared with direct pulp capping or partial pulpotomy) and is, therefore, the recommended treatment.
Pulps where inflammation is established and has extended to the radicular pulp. This involves carious pulp exposure where bleeding following excision of the coronal pulp is excessive and cannot be controlled within a reasonable time (5–10 minutes). Pulpectomy and RCT is the recommended treatment.
The term ‘asymptomatic irreversible pulpitis’ should be reconsidered
The term asymptomatic irreversible pulpitis was adopted by the American Association of Endodontists (AAE) and the American Board of Endodontics in 2008.26 It is described as ‘a clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing, and that root canal treatment is indicated. These cases have no clinical symptoms and usually respond normally to thermal testing, but may have had trauma or deep caries that would be likely result in exposure following removal’.26 While histological studies have shown that the pulp can be irreversibly inflamed without exhibiting any symptoms, there are two main concerns with this definition:
It can be assumed that any pulp exposure (be it carious or traumatic) can be diagnosed as irreversible pulpitis. In fact, pulp exposure, especially after physical or iatrogenic trauma, most frequently occurs over healthy or reversibly inflamed pulp.
The second and bigger concern is with the recommendation ‘that the vital inflamed pulp is incapable of healing, and that root canal treatment is indicated’. Recent clinical and histopathological studies have demonstrated that a clinical diagnosis of an irreversible pulpitis (even in the presence of clinical signs and symptoms) can be treated with partial excision of the pulp (partial or full pulpotomy).13,22,30,49
This term was revised in 2020 in the AAE's 10th edition of the ‘Glossary of Endodontic Terms’.50 Asymptomatic irreversible pulpitis was defined as: ‘A clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing. Additional descriptors: no clinical symptoms but inflammation produced by caries, caries excavation, trauma’. Recently, the AAE published a position statement on vital pulp therapy that stated that a ‘pretreatment diagnosis of irreversible pulpitis is not necessarily an indication for pulpectomy, as more conservative treatment could be considered’.51 While the revised definition removed the advice that root canal treatment is indicated when a diagnosis of asymptomatic irreversible pulpitis is made, it still states that the inflamed pulp is incapable of healing. Therefore, the term asymptomatic irreversible pulpitis may still be confusing and may result in overprescription of pulpectomy and RCT. The authors suggest reconsidering both the definition and treatment recommendations for this disease category.
Rubber dam isolation during deep caries management should become mandatory
Recent guidelines and reference to the literature related to managing deep caries, including handling of vital pulp tissue is essential. Rubber dam remains the gold standard isolation technique and, in addition to many other benefits, provides a surgically clean field and aseptic environment for the restorative/endodontic procedure. However, less than 20% of UK dentists frequently use rubber dam in endodontic therapy52 and only 29.2% of primary care dental professionals within the UK used rubber dam for deep caries management.53 Ireland discussed the use of rubber dam as early as 1962, stating, ‘probably no other technique, treatment or instrument used in dentistry is so universally accepted and advocated by the recognized authorities, and so universally ignored by practising dentists’.54 Rubber dam isolation during deep caries excavation should become mandatory because the lack of an aseptic environment may preclude the use of VPT techniques.55 Additionally, when removing coronal pulp tissue, a new sterile bur using sterile saline as an irrigant/coolant would be advisable to minimize any additional infection risk.
Conclusion
Interest in VPT as an endodontic treatment modality is widespread. Its application has developed and involves carious pulp exposure in mature permanent teeth with signs and symptoms suggestive of irreversible pulpitis. The prognosis of VPT procedures has improved drastically thanks to our better understanding of pulp pathology and the introduction of calcium silicate cements. The term asymptomatic irreversible pulpitis may result in unnecessary RCTs performed and its definition should be revised.