Article
Anything you can do…
‘Clocking’ the cover photograph of the latest issue of Dental Update, showing an avulsed central incisor holding on for dear life by a thread of saliva, I was reminded of a trauma case I saw initially in 2015, and not wishing to be outdone, the lyric ‘Anything you can do I can do better’ (Annie Get Your Gun) rang loudly in my head.
I was getting back into the swing of things after a nice Christmas break when on the 6th January 2015, I received a call from a patient saying her 12-year-old son had had an accident with his skateboard and had knocked out a tooth. The relevant advice was given and she was told to bring him in immediately. On arrival I was presented with a young man with a very swollen lip and bloody mouth and an avulsed front tooth. A very large blood clot was obscuring most of the upper anterior maxillary region.
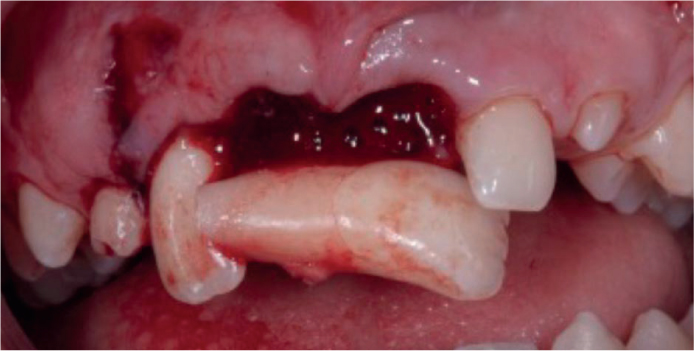
After initial debridement of the clot, I was faced with this: UL1 had been completely avulsed but UR1 had also been avulsed, but was jammed between the subluxed UR2 and the relatively undamaged UL2 (Figure 1).
Teeth were replanted, repositioned and after multiple appointments, including root treatment of the three teeth involved, with Figure 2 showing what had been achieved 15 months later. He was advised that the long-term prognosis wasn't good but I hoped he could keep his natural teeth until maturity and implants might be an option.

In spite of requests to come back, other than one visit about a year later, he didn't present again for over 6 years complaining his teeth didn't look very nice (Figure 3). All three teeth had very significantly resorbed and were ankylosed. He refused a referral to secondary care and asked if something could be done to improve the appearance without resorting to extensive treatment. With some reshaping of the root-filled UR2 and composite bonding we were able to give him an acceptable result, albeit possibly short lived (Figure 4).


Having graduated in 1983, when bonding and composites were in their infancy, I could never have imagined, 32 years later, treatment such as this might be possible. As I am writing this another song, from the Italian Job 1969, comes to mind, ‘The Self Preservation Society’.
Change ‘self’ for ‘tooth’ and this reflects nicely on what we should all be focusing on.
Pragmatic minimally invasive, aesthetic dentistry and, in this case, avoiding the need for extractions and prosthetic replacements in a young teenager, which will hopefully last into his late 20s and beyond.