Stoopler ET, Sollecito TP, Chen SY. Amyloid deposition in the oral cavity: a retrospective study and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:674-680 https://doi.org/10.1067/moe.2003.136
Dobson M, Wright A, White S, Macluskey M. Localised oral amyloidosis in the context of oral epithelial dysplasia: literature review and report of two cases. Oral Surg. 2022; 15:333-339 https://doi.org/10.1111/ors.12619
Muchtar E, Dispenzieri A, Magen H Systemic amyloidosis from A (AA) to T (ATTR): a review. J Intern Med. 2021; 289:268-292 https://doi.org/10.1111/joim.13169
Memari F, Jahandideh H, Moghtader K, Amini-Harandi A. Narrowing of the upper airway due to amyloidosis: A case report. J Clin Med Res. 2011; 3:52-56
Li Y, Liu N, Xu Y Widespread purple bulla-like masses of the oral mucosa. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 114:552-557 https://doi.org/10.1016/j.oooo.2011.11.007
Foli A, Palladini G, Caporali R The role of minor salivary gland biopsy in the diagnosis of systemic amyloidosis: results of a prospective study in 62 patients. Amyloid. 2011; 18:80-82 https://doi.org/10.3109/13506129.2011.574354029
Deng J, Chen Q, Ji P Oral amyloidosis: a strategy to differentiate systemic amyloidosis involving the oral cavity and localized amyloidosis. Oral Dis. 2019; 25:670-675 https://doi.org/10.1111/odi.12870
van der Waal RI, van de Scheur MR, Huijgens PC Amyloidosis of the tongue as a paraneoplastic marker of plasma cell dyscrasia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:444-447 https://doi.org/10.1067/moe.2002.126342
Wechalekar AD, Gillmore JD, Bird J Guidelines on the management of AL amyloidosis. Br J Haematol. 2015; 168:186-206 https://doi.org/10.1111/bjh.13155
Maurer MS, Schwartz JH, Gundapaneni B Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018; 379:1007-1016 https://doi.org/10.1056/NEJMoa1805689
Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol. 1995; 32:45-59
Mahmood S, Sachchithanantham S, Bridoux F Risk of progression of localised amyloidosis to systemic disease in 606 patients over 30 years. Blood. 2013; 122 https://doi.org/10.1182/blood.V122.21.3143.3143
Although oral manifestations of amyloidosis are rare, it is important to exclude systemic involvement in patients who present with amyloidosis involving the oral cavity. Improved understanding of the oral manifestations of amyloidosis and the additional investigations required can lead to timely diagnosis and subsequent management. Treatment of localized forms of amyloidosis include resection, biologics, laser therapy and corticosteroids.
CPD/Clinical Relevance: Understanding the oral manifestations of amyloidosis can lead to timely diagnosis and management.
Article
Localized or systemic amyloidosis results from the abnormal folding of proteins, forming insoluble amyloid fibrils with subsequent deposition in various tissues and organs.1 Based upon the specific protein form that is deposited, it is classified as:
Localized amyloidosis;
Acquired systemic amyloidosis;
Reactive systemic AA amyloidosis;
Hereditary systemic amyloidosis.
Localized amyloidosis occurs most commonly whereby the amyloid protein is restricted to a particular organ or tissue and results in deposition of AL (L stands for light chain, the protein that mutates and causes the disorder) protein.2 In systemic AL amyloidosis, previously termed primary amyloidosis, the AL deposits are located in any, or all, of the viscera, connective tissue and blood vessel walls. It is usually secondary to benign low-grade monoclonal gammopathy.3 Reactive systemic AA (serum amyloid A protein) amyloidosis, formerly known as secondary amyloidosis, occurs as a complication of chronic infections (for example tuberculosis) and inflammatory conditions (e.g. rheumatoid arthritis and Crohn's disease). It is characterized by an increased production of AA (serum amyloid A) protein.4 Hereditary systemic amyloidosis is rare and a result of autosomal dominant diseases in which there is production of amyloid fibrils from inherited variant proteins, such as transthyretin, gelsolin and apolipoprotein A-1 and fibrinogen.5
Both localized and systemic amyloidosis may present with head and neck manifestations.1,2 The tongue and the larynx are the most frequent sites of amyloid deposition.6 Amyloid deposition within muscle, manifesting as macroglossia, results in restriction of tongue movement with difficulty eating and talking.6 Scalloping may be noted on the lateral borders of the tongue from impingement on the teeth. Papules and nodules, haemorrhagic bullae, ecchymosis and ulceration, which frequently involves the floor of the mouth, gingiva, lip and buccal mucosa, are recognized clinical presentations. However, the incidence of amyloid deposits in these areas is much lower when compared with the tongue and larynx.1,7,8 Soft tissue involvement may present with submental and submandibular lymphadenopathy.9 Vascular infiltration in the salivary glands will manifest as xerostomia.10,11 Jaw claudication, suggestive of giant cell arteritis, can occur in AL amyloidosis.12
The clinical manifestations of amyloidosis depend on the type of precursor protein, the tissue distribution and the amount of amyloid deposited. Features suggestive of amyloidosis include waxy skin and easy bruising, enlarged muscles, cardiac failure, cardiac conduction abnormalities, hepatomegaly, nephrotic syndrome, peripheral and/or autonomic neuropathy, and impaired coagulation. Investigations include echocardiography, troponin and NT-proBNP, liver function tests, nerve conduction studies, renal function, and 24-hour urine and serum amyloid P component (SAP) scintigraphy. When inflammation is suspected as the cause of AA amyloidosis, then additional testing is required in line with primary disease, for example a chest radiography or IGRA with tuberculosis, and colonoscopy for Crohn's disease. Amyloidosis of the tongue should be regarded as a paraneoplastic marker of haematological disease. A thorough medical work-up should be performed to exclude underlying disorders, focusing on the existence of gammopathies and underlying lymphoid and plasma cell malignancies.13
There is no cure for amyloidosis and current management focuses on slowing the amyloid accumulation and any subsequent organ dysfunction. AA amyloidosis treatment is primarily based on the underlying inflammatory disease with first-line biologics, such as infliximab or etanercept.14 Localized AL amyloidosis may be managed with local resection, which is usually curative in cases of localized amyloidosis in the head and neck; however, there can be recurrence.15 Management options include observation, surgery for any functional or cosmetic disability, laser therapy, corticosteroids, radiotherapy and chemotherapy. Treatment of familial amyloidosis is with liver transplantation and pharmacological agents, such as tafamidis, a transthyretin stabilizer that has been shown to reduce mortality by approximately 30%.16 Although treatment may slow amyloid deposition, it is important that patients are aware of the prognosis. Localized forms have an excellent prognosis and affected individuals are not at increased risk of developing systemic involvement.2
AL amyloidosis has a median survival of 1–2 years if left untreated, and depending on the extent of organ involvement.17,18
Case report
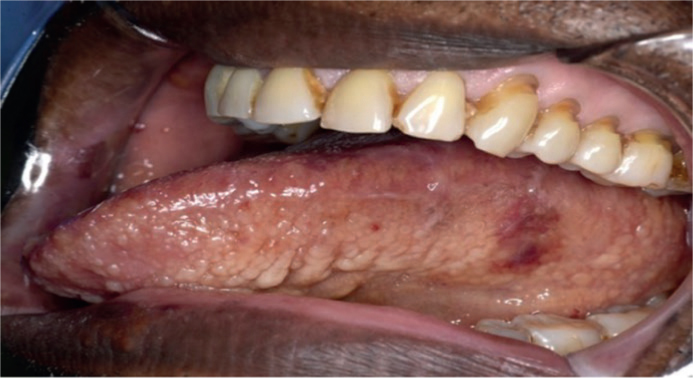
A 63-year-old male presented with a 1-year history of generalized asymptomatic nodules involving the tongue. There was no restriction of tongue movement. The medical history was significant for hypertension, monoclonal gammopathy of unknown significance, hypercholesterolaemia and plasmacytoma. He was a non-smoker and consumed no alcohol. On examination, there were multiple small pink/yellow nodules involving the lower lip, dorsum and lateral tongue and labial mucosa (Figures 1 and 2). Purpuric lesions were noted on the buccal mucosa (Figure 3).
Figure 1. Left lateral border of tongue appears thickened and a purple nodule is present.Figure 2. Multiple small pink and yellow nodules on lower lip.Figure 3. Purpuric lesions on the buccal mucosa and bilateral tongue scalloping associated with macroglossia.
Investigations revealed reduced immunoglobulin A (IgA) and IgM and increased serum kappa light chains and increased kappa lambda ratio. Immunofixation showed a free kappa paraprotein band in the beta region consistent with a monoclonal gammopathy in line with the patients' existing medical history.
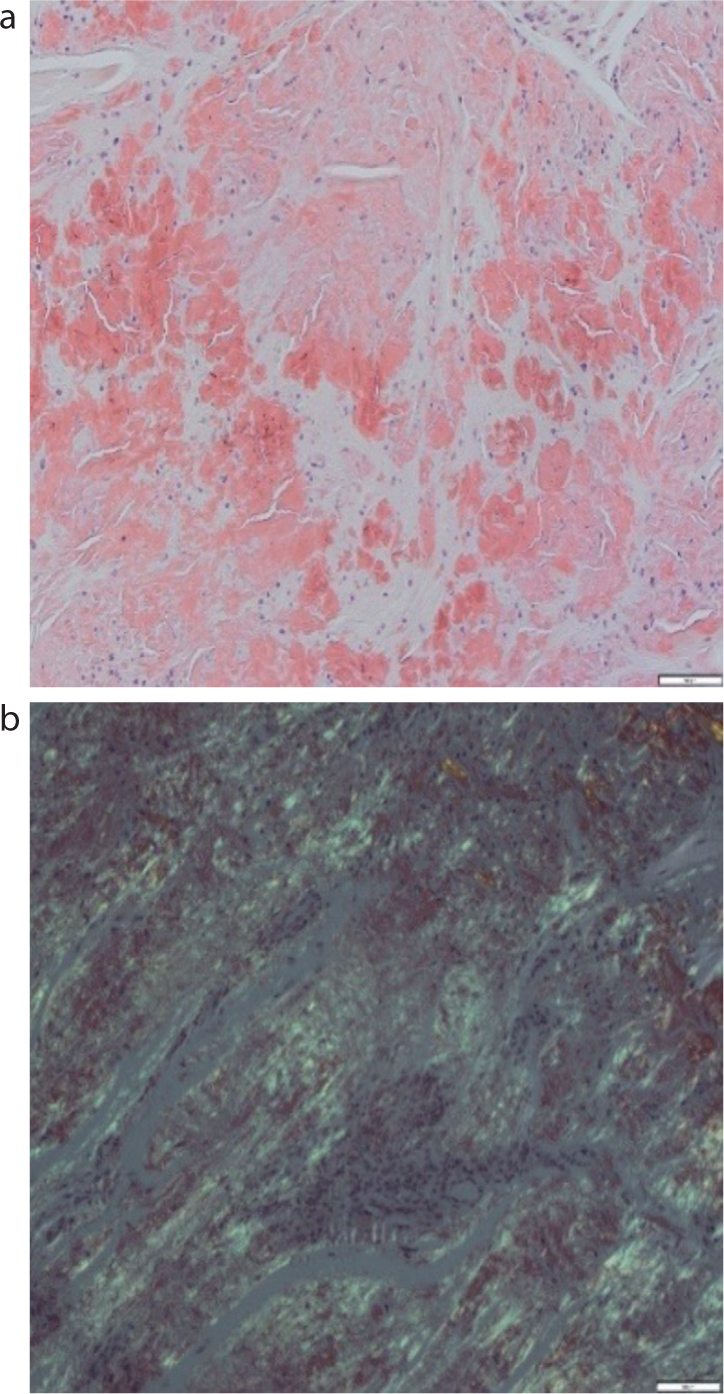
Incisional biopsy of dorsal surface of the tongue and right buccal mucosa identified an accumulation of eosinophilic material that stained positive with Congo red (Figure 4a) and demonstrated green birefringence under polarized light (Figure 4b), consistent with amyloidosis.
Figure 4. (a) Congo red staining of tissue from the dorsal surface of the tongue. (b) Positive green birefringence under polarized light.
The patient was referred to the Centre for Amyloidosis and Acute Phase Proteins, University College London, for further assessment and management. Standard first-line treatment of AL consisting of bortezomib-cyclophosphamide-dexamethasone was commenced to prevent progressive tongue enlargement and subsequent complications of this. Treatment with bortezomib-thalidomide-dexamethasone was another option. Autologous stem cell transplantation remains an alternative treatment option given the absence of vital organ involvement in this case.
Conclusion
Oral manifestations of amyloidosis are rare. It is imperative to exclude systemic involvement in patients with isolated amyloidosis involving the oral cavity. A high index of clinical suspicion is essential to aid in timely diagnosis and prompt specific investigations. Long-term follow-up is suggested for localized disease.