Donnell CC, Johnston MJ, Foley JI. The six-year-old ‘adult’. Prim Dent J. 2021; 10:74-82
Patel TA, Donnell CC, Kirby JE, Frawley T. The orthodontic–paediatric Interface. Part 1. Dent Update. 2024; 52:42-49
Batista KB, Thiruvenkatachari B, Harrison JE, O'Brien KD. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children and adolescents. Cochrane Database Syst Rev. 2018; 3:(3) https://doi.org/10.1002/14651858.CD003452.pub4
Seehra J, Fleming PS, Newton T, DiBiase AT. Bullying in orthodontic patients and its relationship to malocclusion, selfesteem and oral health-related quality of life. J Orthod. 2011; 38:247-256
O'Brien K, Wright J, Conboy F Early treatment for Class II division 1 malocclusion with the twin-block appliance: a multi-center, randomized, controlled trial. Am J Orthod Dentofac Orthop. 2009; 135:573-579
Wiedel A-P, Bondemark L. A randomized controlled trial of self-perceived pain, discomfort, and impairment of jaw function in children undergoing orthodontic treatment with fixed or removable appliances. Angle Orthod. 2016; 86:324-330
Wiedel A-P, Bondemark L. Fixed versus removable orthodontic appliances to correct anterior crossbite in the mixed dentition – a randomized controlled trial. Eur J Orthod. 2015; 37:123-127
Mandall N, Cousley R, DiBiase A Early class III protraction facemask treatment reduces the need for orthognathic surgery: a multi-centre, two-arm parallel randomized, controlled trial. J Orthod. 2016; 43:164-175
Lombardo G, Vena F, Negri P Worldwide prevalence of malocclusion in the different stages of dentition: a systematic review and meta-analysis. Eur J Paediatr Dent. 2020; 21:115-122
Thilander B, Wahlund S, Lennartsson B. The effect of early interceptive treatment in children with posterior cross-bite. Eur J Orthod. 1984; 6:25-34
Brierley CA, Sandler J. Managing the transverse dimension. Orthod Update. 2017; 10:86-94
Dibiase DD. Midline supernumeraries and eruption of the maxillary central incisor. Dent Pract Dent Rec. 1969; 20:35-40
Lygidakis NN, Chatzidimitriou K, Theologie-Lygidakis N, Lygidakis NA. Εvaluation of a treatment protocol for unerupted maxillary central incisors: retrospective clinical study of 46 children. Eur Arch Paediatr Dent. 2015; 16:153-164
Parker K, Acharya P, Collins JM. Methods of applying traction to unerupted maxillary incisors and safety considerations. Orthod Update. 2019; 12:106-110
Andreasen JO, Petersen JK, Laskin DM.Copenhagen, Denmark: Munksgaard; 1997
Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofac Orthop. 1987; 91:483-92
Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Eur J Oral Sci. 1973; 81:12-20
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:249-256
Becker A, Smith P, Behar R. The incidence of anomalous maxillary lateral incisors in relation to palatally-displaced cuspids. Angle Orthod. 1981; 51:24-9
Naoumova J, Kjellberg H. The use of panoramic radiographs to decide when interceptive extraction is beneficial in children with palatally displaced canines based on a randomized clinical trial. Eur J Orthod. 2018; 40:565-574
Benson PE, Atwal A, Bazargani F Interventions for promoting the eruption of palatally displaced permanent canine teeth, without the need for surgical exposure, in children aged 9 to 14 years. Cochrane Database Syst Rev. 2021; 12:(12) https://doi.org/10.1002/14651858.CD012851.pub2
Frawley T, Parkin N. Management of the palatally displaced maxillary canine. Part 2: exposure and orthodontic alignment. Orthod Update. 2022; 15:175-180
Benson PE, Parkin NA. Early management of the palatally displaced maxillary permanent canine. In: Cobourne MT (ed). Cham, Switzerland: Springer; 2017
Olive RJ. Orthodontic treatment of palatally impacted maxillary canines. Aust Orthod J. 2002; 18:64-70
Leonardi M, Armi P, Franchi L, Baccetti T. Two interceptive approaches to palatally displaced canines: a prospective longitudinal study. Angle Orthod. 2004; 74:581-586
Armi P, Cozza P, Baccetti T. Effect of RME and headgear treatment on the eruption of palatally displaced canines: a randomized clinical study. Angle Orthod. 2011; 81:370-374
Baccetti T, Leonardi M, Armi P. A randomized clinical study of two interceptive approaches to palatally displaced canines. Eur J Orthod. 2008; 30:381-385
Baccetti T, Mucedero M, Leonardi M, Cozza P. Interceptive treatment of palatal impaction of maxillary canines with rapid maxillary expansion: a randomized clinical trial. Am J Orthod Dentofac Orthop. 2009; 136:657-661
De Stefani A, Bruno G, Visentin S, Lucchi P, Gracco A. Rapid maxillary expansion for interceptive orthodontic treatment of palatally displaced canine: a systematic review. Eur J Paediatr Dent. 2021; 22:139-143
Seow WK. Developmental defects of enamel and dentine: challenges for basic science research and clinical management. Aust Dent J. 2014; 59:143-154
Prado N, Caldwell S, Ashley M. Orthodontic bonding to atypical tooth surfaces. Orthod Update. 2020; 13:57-62
Papagiannis A, Fanourakis G, Mitsea A Orthodontic treatment of a patient with dentin dysplasia type I and bilateral maxillary canine impaction: case presentation and a family-based genetic analysis. Children. 2021; https://doi.org/10.3390/children8060519
Rowley R, Hill FJ, Winter GB. An investigation of the association between anterior open-bite and amelogenesis imperfecta. Am J Orthod. 1982; 81:229-235
Weinmann JP, Svoboda JF, Woods RW. Hereditary Disturbances of Enamel Formation and Calcification. J Am Dent Assoc. 1945; 32:397-418
Alachioti X, Dimopoulou E, Vlasakidou A, Athanasiou A. Amelogenesis imperfecta and anterior open bite: Etiological, classification, clinical and management interrelationships. J Orthod Sci. 2014; 3:1-6
Benson PE, Alexander-Abt J, Cotter S Resin-modified glass ionomer cement vs composite for orthodontic bonding: a multicenter, single-blind, randomized controlled trial. Am J Orthod Dentofac Orthop. 2019; 155:10-18
Dental decisions made during childhood and adolescence can have long-term implications. The orthodontic–paediatric interface ensures that children are assessed and managed by the right people, in the right place, at the right time. This two-part series offers general dental practitioners (GDPs) and specialists an update on common joint orthodontic–paediatric problems in the mixed dentition alongside practical considerations to resolve them. The second article focuses on: interceptive orthodontics, crossbites, unerupted central incisors, ectopic and impacted canines, and enamel and dentine disorders.
CPD/Clinical Relevance: This series will enable GDPs to recognize and manage common problems in primary care.
Article
The successful management of a developing malocclusion is dependent upon a healthy, tripartite relationship between general dental practitioner (GDP), orthodontist and paediatric dentist. A brief orthodontic examination should form a routine part of a dental examination once a child reaches their sixth birthday, to monitor the eruption of the first permanent molars and permanent incisors, and facilitate the recognition of a developing malocclusion. This can facilitate timely referral to secondary care for assessment and/or interceptive treatment, which may help simplify, streamline or cease the need for future complex orthodontic management in some cases.1 Close collaboration between primary and secondary care teams ensures the successful outcome of long-term orthodontic plans. There needs to be a close synergy between all members to ensure a patient is seen by the right person, in the right place, at the right time.
This article complements the first in the series and further expands on joint orthodontic–paediatric problems in the mixed dentition so that GDPs are able to identify common problems, recognize abnormal dental development and refer at the appropriate time.
Interceptive orthodontics
Class II
Class II relationships often present with increased overjets, lower lip traps and habits. Interception of habits has been described in Part 1 of this series.2 In these cases, the use of a mouthguard should be emphasized to reduce the risk of dental trauma.
A Cochrane review in 2018 identified some benefit for interceptive early treatment of a Class II relationship, in terms of reducing the incidence of new incisal trauma.3 Additionally, early treatment is sometimes indicated if bullying is a particular concern. Seehra and colleagues have previously described how bullying was significantly associated with a Class II division 1 malocclusion and an increased overjet and overbite.4 Referral to orthodontics at the optimal time can enable functional appliance treatment to be commenced if indicated. Retention of a twin block appliance is often gained using Adam's cribs on the upper and lower first premolars and molars. For this reason, the eruption of these teeth is generally preferred before starting functional treatment. However, where indicated, modifications can be made, particularly in cases of hypodontia and traumatic loss of teeth (Figure 1). Despite the aforementioned indications, early treatment can be challenging in terms of both maintaining cooperation and retaining the sagittal correction achieved following functional appliance treatment until fixed appliances can be bonded. Early treatment of Class II malocclusions can be associated with increased overall treatment time and cost. It has also been associated with less optimal occlusal outcomes.5 Therefore, delaying the start of this treatment to coincide with the anticipated peak in the adolescent growth spurt is often preferred, allowing for a smooth transition between functional and fixed treatment (Figure 2).
Figure 1.
(a–f) Early treatment of Class II division 1 malocclusion using a functional appliance. In this case, an early treatment approach was chosen owing to the increased risk of further trauma (patient had had multiple accidents culminating in avulsion of UR1). (g–l) Despite successful initial correction of the overjet, there was significant relapse while awaiting the eruption of the permanent dentition.Figure 2.
(a–f) Conventional timing of functional appliance treatment to reduce an increased overjet. The patient was treated during their adolescent growth spurt after sufficient permanent teeth had erupted. (d–f) Twin block appliance. (g–i) Placement of fixed appliances for alignment and occlusal detailing following successful overjet reduction using a twin block. (j–l) The final outcome at debond.
Class III
Class III malocclusions can be challenging to manage orthodontically because of the influence of growth. Patients may present with features of a Class III malocclusion at an early stage, for example an anterior crossbite associated with a displacement. This could also result in hard and soft tissue damage, such as attrition and recession. Interceptive treatment for Class III cases is sometimes useful to reduce the need and complexity for later treatment, but also reduce the risk of further damage to the hard and soft tissues.
Identifying the aetiology is important in the management of these cases. These patients may be monitored until their growth potential has slowed sufficiently to determine whether the patient can be treated orthodontically or if this needs to be combined with orthognathic surgery to achieve an ideal outcome. Where interceptive management is indicated, the use of a sectional, 2x4 upper fixed appliance can be used to correct an anterior crossbite (Figure 3). Alternatively, an upper removable appliance with posterior bite planes and either an anterior spring or screw could be used, although treatment has been shown to be slower and more expensive with this method (Figure 4).6,7 A sufficient overbite is important to aid in stability of the correction in these interceptive cases.
Figure 3. III interceptive treatment. (a–c) Class III incisor relationship and left-sided posterior crossbite. Significant recession affecting LR1. Caries is noted on the URC. (d–f) UFA to correct anterior and lateral crossbites simultaneously. (g–i) Awaiting eruption of rest of permanent dentition before phase II treatment to address crowding. There had been some improvement in the recession affecting LR1 following resolution of the anterior crossbite.Figure 4.
(a–c) Class III interceptive treatment. Patient in mixed dentition with increased overbite and ability to bite edge-to-edge. (d–f) Class III interceptive treatment. URA with Z springs to procline upper central incisors and posterior bite planes to disengage occlusion. (g–i) Anterior crossbite correction is ‘self-retained’ by the positive overbite. Awaiting eruption of permanent dentition before considering need for a definitive course of orthodontic treatment.
‘Growth modification’ treatments can also be used in this cohort of patients. In a multicentre randomized controlled trial (RCT), the use of protraction facemask treatment in patients aged 7–9 years old, was shown to reduce the later subjective need for orthognathic treatment compared to untreated controls.8 For patients of this cohort, with a skeletal class III pattern owing to maxillary hypoplasia, it is worth GDPs considering referral to a local specialist orthodontist.
Crossbites
Crossbites can present anteriorly and/or posteriorly, owing to a discrepancy of the antero-posterior or transverse dimensions, respectively. As discussed previously, crossbites can result in recession and tooth surface loss. The aetiology could result from a combination of skeletal, soft tissue and dental factors. Additionally, persistent habits, such as digit sucking, can result in the development of posterior crossbites.9 Early diagnosis and management can aid in preventing unintended consequences, which can persist into the full permanent dentition. Lombardo described the prevalence of posterior crossbites in children in Europe as approximately 4%.10
The interceptive management of anterior crossbites has been discussed previously in the management of Class III malocclusions. In terms of posterior crossbites, the factors that need to be considered when choosing between interventions include the extent of expansion required, the presence of sufficient teeth for appliance retention, the presence of a displacement, patient age, anticipated patient cooperation, oral hygiene and the likely stability of the correction.
In some cases, a crossbite can self-correct as the permanent teeth erupt.11 If the aetiology of the crossbite involves a habit such as thumb sucking, early cessation of the habit is vital and will often result in some spontaneous correction. In 2021, a Cochrane review highlighted that, for patients treated in the early mixed dentition, both removable appliances and quad helixes are beneficial for correcting posterior crossbites, although treatment with quad helix has been shown to have shorter treatment times.9 Rapid maxillary expansion (RME) appliances may also occasionally be considered in the mixed dentition. Other methods, such as incorporation of expansion screws into a functional appliance, archwire expansion, cross-elastics, self-ligating brackets and expansion arches can be used to correct posterior crossbites in the permanent dentition.12
Unerupted central incisors
The developing dentition should be regularly monitored for correct sequence of eruption. Delayed eruption of a permanent maxillary incisor tooth should be considered when the contralateral tooth erupted over 6 months ago, the mandibular incisors erupted over 1 year ago, or there is a deviation from the normal sequence of eruption. The authors would recommend early referral to an orthodontist, or paediatric dentist in this situation.
The aetiology of such cases can often be associated with dental factors. For example, supernumeraries in the premaxillary region have been found in 2.6% of a referred UK population, which subsequently were found to be associated with the failed eruption of 42% of maxillary central incisors.13 Tuberculate and odontome types of supernumerary teeth are the most likely to prevent incisor eruption.13,14
Furthermore, trauma to the deciduous incisors may result in dilaceration of the crown or root of the permanent central incisors and subsequently affect the eruption of these teeth.
Additionally, early loss of primary teeth, prolonged retention of primary teeth and crowding in the upper anterior segment may all prevent eruption of the incisor. Gingival fibromatosis, scar tissue or pathology, such as cysts, tumours or infection, can result in a physical obstruction to eruption of central incisors and should also be considered where no other obvious cause can be identified.
A multidisciplinary approach to these cases is imperative (Figure 5). Recently updated guidance by the Royal College of Surgeons of England highlights the need to consider several factors, including the space requirement to address the underlying malocclusion, patient age, medical history and likely compliance levels, as well as the eruptive potential of the impacted incisor.14
Figure 5.
(a–e) Significant impaction of UR1 and UL1 owing to the presence of two, unerupted supernumerary teeth. (f–h) Removal of URC, URA, ULA, ULC and both unerupted supernumeraries, and orthodontic traction to gold chains bonded to UR1 and UL1, demonstrating the use of piggyback mechanics to provide vertical anchorage support while erupting UR1 and UL1. (i–m) Occlusal outcome at debond.
When alignment of the incisor is favourable, removal of any obstructions, such as supernumeraries and retained deciduous teeth, in patients younger than 9 years of age, may allow for the spontaneous eruption of the unerupted tooth, providing there is sufficient space for the tooth. However, consideration should be always given to the method of removal of any obstruction(s), as combining the procedure with an exposure may be necessary to limit the number of general anaesthetic (GA) episodes.
In older children (i.e. over 9 years of age), the eruptive potential of the impacted incisor may be reduced and therefore gold chain placement may be indicated to enable orthodontic alignment of the tooth.
Dilacerated teeth need to be carefully assessed, in some cases using cone beam computed tomography (CBCT), to reduce the risk of alignment resulting in fenestration through the cortical plate and subsequent devitalization.
As well as removing any obstructions, it is important to create sufficient space for the impacted incisor.15 Fixed appliances are most commonly used for this purpose, and can also be used for subsequent alignment of the exposed central incisor. One potential limitation of using a fixed appliance in the mixed dentition is that large unsupported sections of archwires can pose risks if they are fractured. Alternative approaches, including the use of upper removable appliances and magnets have been described by Parker and colleagues; however, it is often more pragmatic to incorporate any firm primary teeth into the fixed appliance.16 In some cases, alignment of the unerupted central incisor is unfavourable. In this situation, surgical removal of the impacted incisor may be necessary, and both short-term and long-term replacement options need to be carefully considered at the outset. If the optimal plan is determined to be long-term replacement of the incisor, then maintaining space for this tooth in the short term, for example by use of a removable appliance with a prosthetic tooth and stainless-steel stops (in case of fracture), should also be considered to prevent further space loss and an upper dental centreline shift.
In situations where alignment is deemed to be unfavourable, or when incisors fail to erupt with orthodontic traction (potentially due to ankylosis), considerations for the long-term replacement of the incisor need to be taken. Orthodontically, this may require treatment to optimize the space available for a prosthetic replacement. Occasionally, it may be more appropriate to work towards camouflaging the adjacent lateral incisor as a central incisor, dependant on the rest of the malocclusion. Involvement of the restorative team at the outset is also of great importance in cases where the incisor must be removed to ensure optimal long-term outcomes.
Palatally displaced canines (PDCs)
As with unerupted central incisors, a patient's dental development should be closely monitored for eruption of the permanent canines. Maxillary permanent canine teeth are the most likely to become impacted (after third permanent molars).17 Canines that are palatally displaced and fail to erupt into the mouth, are found in 1–3% of the population.18,19 There are two main theories with regards to the aetiology of this: the genetic theory, described by Peck; and the guidance theory, described by Becker.20,21
As permanent canines develop, they move from a palatal position to a more buccal one, ordinarily being palpable from approximately the age of 10 years old in the buccal sulcus. This is often accompanied by progressive mobility of the deciduous canines. If these signs are not detected, further investigation into the position of the canines should be considered. Failure to diagnose displaced canines early could result in significant resorption of adjacent teeth or may complicate future orthodontic treatment.
The findings of a recent RCT suggest that interceptive extraction of a deciduous canine can aid spontaneous eruption of the permanent canine in situations where the tooth has mild-to-moderate displacement and there is minimal maxillary arch crowding.22 However, a recent Cochrane review stated that the evidence base is ‘uncertain’ in this area.23 The present authors would like to emphasize the importance of early referral of these patients to an orthodontist because careful assessment of the severity of displacement is required before committing to extraction of the primary canine.23 Consideration for interceptive extraction of the deciduous canine should only be taken if the patient is 10–13 years old, with less than 2-mm crowding in the maxillary arch, and the canine is in a favourable position (i.e. in sector 2–3 with an alpha angle less than 21°).24,25 It would also be imperative to discuss the potential need for exposure and alignment if the interceptive treatment was unsuccessful with the patient and their parent(s). Double extraction, where the deciduous maxillary canine and deciduous maxillary first molars has also been suggested in the literature, although the aforementioned Cochrane systematic review found no evidence that this increases the likelihood that palatally displaced canines will erupt at 18 months, compared to a single extraction of the deciduous maxillary canine.23
Another method discussed in the literature includes the creation of space to improve the eruption of the canine (Figure 6).26 Various methods of space creation have been investigated for this purpose, including the use of headgear, RME, quad helices and upper fixed appliances.27–31
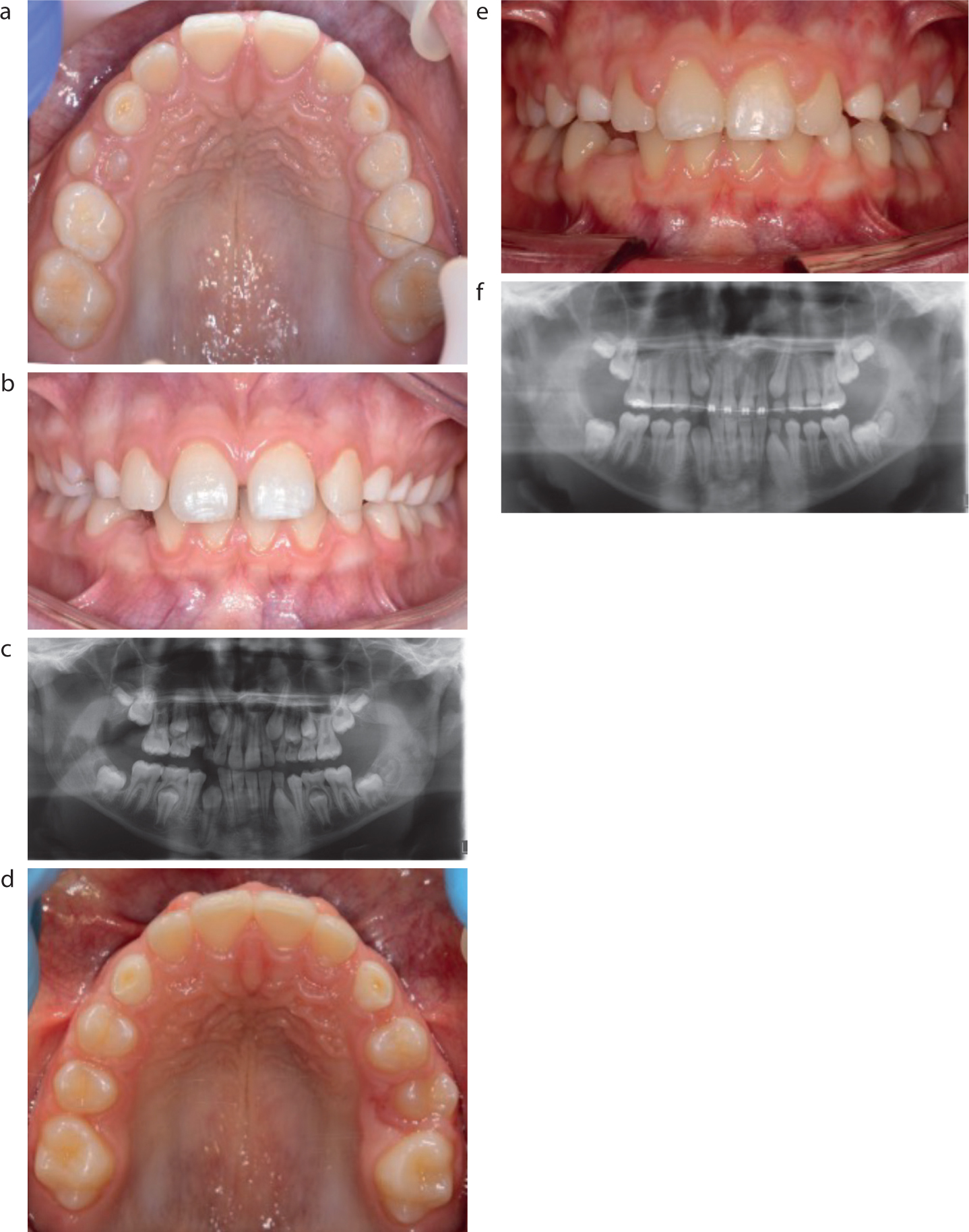
Figure 6.
(a–c) An 11 year old with palatally displaced upper permanent canines (c) UR3 lies in sector 3; UL3 lies in sector 2. (d–f) Following interceptive treatment using an upper fixed appliance to redistribute spacing in the upper arch, there was some spontaneous improvement in the mesial position of the upper permanent canines. (f) UR3 and UL3 now lie in sector 1 and are close to eruption.
For more severely displaced canines, which are unfavourable for alignment, consideration should be given to incorporating removal of the displaced permanent canine into the overall extraction pattern for the patient's malocclusion. This may involve the camouflage of the first premolar as the canine tooth. If the permanent canine requires exposure (open or closed), consideration needs to be given to patient cooperation, motivation, age, severity of displacement and the existing malocclusion.
Enamel and dentine disorders
Disorders and abnormalities of dentine and enamel have been linked to a diverse range of interactive influences, from genetic factors (inherited as mutations in genes themselves, or as a feature of a familial condition), to environmental changes and systemic insults during enamel formation such as infections, radiation and metabolic conditions.32
With increasing numbers of patients now receiving orthodontic treatment, the number of those being treated with atypical tooth surfaces is also likely to increase. This includes enamel conditions such as amelogenesis imperfecta (AI), molar–incisor hypomineralization (MIH) and fluorosis, as well as dentine conditions such as dentinogenesis imperfecta (DI) and dentine dysplasia (DD).33 It is important that all members of the dental team have working knowledge of, and are able to distinguish between, the various types of enamel and dentine disorders, because this will affect the management options proposed. Localized and chronological enamel defects may be present on teeth due to a variety of factors: trauma or localized infection related to the primary predecessor, severe or chronic childhood conditions such as vitamin D deficiency, coeliac disease, liver and kidney diseases. These typically present as either hypoplastic or hypomineralized defects.34
As opposed to molar–incisor hypomineralization (MIH), described in Part 1 of this series,2 dental fluorosis can cause generalized hypomineralization of the enamel that results in subsequent brown discolouration and post-eruptive breakdown, both anteriorly and posteriorly (Figure 7). Teeth affected by dental fluorosis may display a spectrum of discolouration from opaque whiteness to pitted surfaces that are stained yellow–dark brown. A detailed fluoride history and family history is important to distinguish between dental fluorosis and other enamel defects, such as AI.
Figure 7. Dental fluorosis showing generalized hypomineralization of the enamel that results in subsequent brown discolouration and post-eruptive breakdown.
AI is a genetically inherited enamel defect, that is quite rare, affecting between 1 in 700 and 1 in 14,000 people and can presented as an isolated genetic defect or as part of a syndrome.34 Hypomineralized AI is subdivided into hypocalcified (typically with a distinct dark yellow colour), and hypomature (typically with white diffuse opacities and mottling). Hypomature AI may present similarly to fluorosis or even MIH on occasion, hence a good family and medical history is crucial in determining a definitive diagnosis.34 Hypoplastic AI tends to present as teeth with thin or absent enamel, alongside visible pits and grooves. Affected teeth display normal enamel colour to a more yellow/brown colour. Affected teeth pose issues with aesthetics, bonding, sensitivity and can have a severe impact on a patient's quality of life – management options are complex and often require specialist input and care.
Children with developmental dentine defects will usually present once the primary teeth begin to erupt and early referral to specialist paediatric dental services is advised. They are less common than developmental defects of enamel; however, clinical implications, especially in the primary dentition, tend to be more severe.34 Dentine defects are grouped into those that affect dentine tissues only and those that show bone involvement alongside the dentine defect: osteogenesis imperfecta-related DI, isolated DI (mild, moderate, severe) and radicular dentine dysplasia.35 Teeth may appear translucent, while some display shades of blue-grey or opalescent brown, and the crown tends to be more bulbous in form. Radiographically, they have a distinct small pulp chamber and small, narrow roots, with some showing complete obliteration of the pulp complex/root canal or even appear to be floating ‘rootless’ teeth – this can pose an issue owing to the potential adverse effects of orthodontic forces on short or malformed roots.35
Orthodontic considerations
Patients who present with enamel and dentine disorders can also present with delayed tooth eruption, delayed exfoliation of primary teeth, impactions and hypodontia. The teeth themselves may be abnormal in morphology and can be more susceptible to tooth wear, resulting in short clinical crown heights.
There is a suggestion in the literature that patients with AI may have a genetically determined anomaly within their craniofacial development that means they are more likely to present with an anterior open bite (AOB).36 Other theories are suggestive of a defective eruptive mechanism secondary to disturbances of the enamel epithelium, but the skeletal origin of the AOB appears to be favoured.37,38
Bonding can be challenging in cases where the enamel and dentine is defective. Patients with AI and DI are likely to have dentine hypersensitivity secondary to the loss of enamel. The use of etch can result in discomfort for these patients and therefore, self-etching primers have been advocated. Alternatively, resin-modified glass ionomer cements (RMGICs) have been suggested, with one RCT finding no difference in failure rate between composite and RMGIC.39 Given that multiple fixed appliance debonds in this patient cohort can increase treatment time and care burden, consideration to alternatives, such as clear aligners with a limited number of attachments, may be favoured in specific cases.33,40
Conclusions
This article further demonstrates the importance of fostering a strong partnership between primary and secondary care clinicians in the management of common orthodontic–paediatric problems. The clinical cases presented across this two-part series serve as a guide in the early recognition of developing malocclusions and their optimal management across a diverse range of presenting issues. Timely referral from GDPs, alongside collaborative working between orthodontists and paediatric dentists, facilitates the best chance to produce ideal clinical outcomes.