Seibert JS Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent (Lawrenceville). 1983; 4:437-453
Esposito M, Grusovin MG, Felice P The efficacy of horizontal and vertical bone augmentation procedures for dental implants - a Cochrane systematic review. Eur J Oral Implantol. 2009; 2:167-184
Sanz-Sanchez I, Sanz-Martin I, Ortiz-Vigon A Complications in bone-grafting procedures: classification and management. Periodontol 2000. 2022; 88:86-102 https://doi.org/10.1111/prd.12413
Benic GI, Hammerle CH Horizontal bone augmentation by means of guided bone regeneration. Periodontol 2000. 2014; 66:13-40 https://doi.org/10.1111/prd.12039
Briguglio F, Falcomata D, Marconcini S The use of titanium mesh in guided bone regeneration: a systematic review. Int J Dent. 2019; https://doi.org/10.1155/2019/9065423
Fontana F, Maschera E, Rocchietta I, Simion M Clinical classification of complications in guided bone regeneration procedures by means of a nonresorbable membrane. Int J Periodontics Restorative Dent. 2011; 31:265-273
Lim G, Lin GH, Monje A Wound healing complications following guided bone regeneration for ridge augmentation: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2018; 33:41-50 https://doi.org/10.11607/jomi.5581
Vergara JA, Quinones CR, Nasjleti CE, Caffesse RG Vascular response to guided tissue regeneration procedures using nonresorbable and bioabsorbable membranes in dogs. J Periodontol. 1997; 68:217-224 https://doi.org/10.1902/jop.1997.68.3.217
Chao YC, Chang PC, Fu JH Surgical site assessment for soft tissue management in ridge augmentation procedures. Int J Periodontics Restorative Dent. 2015; 35:e75-83 https://doi.org/10.11607/prd.2097
Machtei EE The effect of membrane exposure on the outcome of regenerative procedures in humans: a meta-analysis. J Periodontol. 2001; 72:512-516 https://doi.org/10.1902/jop.2001.72.4.512
Misch CM Comparison of intraoral donor sites for onlay grafting prior to implant placement. Int J Oral Maxillofac Implants. 1997; 12:767-776
Monje A, Monje F, Suarez F Vertical and horizontal ridge augmentation of a severely resorbed ridge in the anterior maxilla. Clinical Advances in Periodontics. 2013; 3:230-236 https://doi.org/10.1902/cap.2012.120068
Simion M, Baldoni M, Zaffe D Jawbone enlargement using immediate implant placement associated with a split-crest technique and guided tissue regeneration. Int J Periodontics Restorative Dent. 1992; 12:462-473
Chiapasco M, Romeo E, Vogel G Vertical distraction osteogenesis of edentulous ridges for improvement of oral implant positioning: a clinical report of preliminary results. Int J Oral Maxillofac Implants. 2001; 16:43-51
Thoma DS, Bienz SP, Figuero E Efficacy of lateral bone augmentation performed simultaneously with dental implant placement: A systematic review and meta-analysis. J Clin Periodontol. 2019; 46:(Suppl 21)257-276 https://doi.org/10.1111/jcpe.13050
Fugazzotto PA Maintenance of soft tissue closure following guided bone regeneration: technical considerations and report of 723 cases. J Periodontol. 1999; 70:1085-1097 https://doi.org/10.1902/jop.1999.70.9.1085
Hur Y, Bui MN, Griffin TJ, Ogata Y Modified periosteal releasing incision for flap advancement: a practical technique for tensionless closure. Clin Adv Periodontics. 2015; 5:229-234 https://doi.org/10.1902/cap.2014.140009
Langer B, Langer L Overlapped flap: a surgical modification for implant fixture installation. Int J Periodontics Restorative Dent. 1990; 10:208-215
Park JC, Kim CS, Choi SH Flap extension attained by vertical and periosteal-releasing incisions: a prospective cohort study. Clin Oral Implants Res. 2012; 23:993-998 https://doi.org/10.1111/j.1600-0501.2011.02244.x
Burkhardt R, Preiss A, Joss A, Lang NP Influence of suture tension to the tearing characteristics of the soft tissues: an in vitro experiment. Clin Oral Implants Res. 2008; 19:314-319 https://doi.org/10.1111/j.1600-0501.2007.01352.x
Leong DJ, Oh TJ, Benavides E Comparison between sandwich bone augmentation and allogenic block graft for vertical ridge augmentation in the posterior mandible. Implant Dent. 2015; 24:4-12 https://doi.org/10.1097/ID.0000000000000180
Marsidi N, Vermeulen SAM, Horeman T, Genders RE Measuring forces in suture techniques for wound closure. J Surg Res. 2020; 255:135-143 https://doi.org/10.1016/j.jss.2020.05.033
Tal H, Kozlovsky A, Artzi Z Long-term bio-degradation of cross-linked and non-crosslinked collagen barriers in human guided bone regeneration. Clin Oral Implants Res. 2008; 19:295-302 https://doi.org/10.1111/j.1600-0501.2007.01424.x
Scheyer ET, McGuire MK Evaluation of premature membrane exposure and early healing in guided bone regeneration of periimplant dehiscence and fenestration defects with a slowly resorbing porcine collagen ribose cross-linked membrane: a consecutive case series. Clin Adv Periodontics. 2015; 5:165-170 https://doi.org/10.1902/cap.2014.130080
Mendoza-Azpur G, de la Fuente A, Chavez E Horizontal ridge augmentation with guided bone regeneration using particulate xenogenic bone substitutes with or without autogenous block grafts: A randomized controlled trial. Clin Implant Dent Relat Res. 2019; 21:521-530 https://doi.org/10.1111/cid.12740
Tay JRH, Lu XJ, Lai WMC, Fu JH Clinical and histological sequelae of surgical complications in horizontal guided bone regeneration: a systematic review and proposal for management. Int J Implant Dent. 2020; 6 https://doi.org/10.1186/s40729-020-00274-y
Verardi S, Simion M Management of the exposure of e-PTFE membranes in guided bone regeneration. Pract Proced Aesthet Dent. 2007; 19:111-117
Urban IA, Nagursky H, Lozada JL, Nagy K Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 25 patients. Int J Periodontics Restorative Dent. 2013; 33:299-307 https://doi.org/10.11607/prd.1407
Fu JH, Wang HL Horizontal bone augmentation: the decision tree. Int J Periodontics Restorative Dent. 2011; 31:429-436
Sakkas A, Wilde F, Heufelder M Autogenous bone grafts in oral implantology-is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int J Implant Dent. 2017; 3 https://doi.org/10.1186/s40729-017-0084-4
Clementini M, Morlupi A, Agrestini C, Ottria L Success rate of dental implants inserted in autologous bone graft regenerated areas: a systematic review. Oral Implantol (Rome). 2011; 4:3-10
Acocella A, Bertolai R, Colafranceschi M, Sacco R Clinical, histological and histomorphometric evaluation of the healing of mandibular ramus bone block grafts for alveolar ridge augmentation before implant placement. J Craniomaxillofac Surg. 2010; 38:222-230 https://doi.org/10.1016/j.jcms.2009.07.004
Pourabbas R, Nezafati S Clinical results of localized alveolar ridge augmentation with bone grafts harvested from symphysis in comparison with ramus. J Dent Res Dent Clin Dent Prospects. 2007; 1:7-12 https://doi.org/10.5681/joddd.2007.002
Zeltner M, Fluckiger LB, Hammerle CH Volumetric analysis of chin and mandibular retromolar region as donor sites for cortico-cancellous bone blocks. Clin Oral Implants Res. 2016; 27:999-1004 https://doi.org/10.1111/clr.12746
Cordaro L, Torsello F, Miuccio MT Mandibular bone harvesting for alveolar reconstruction and implant placement: subjective and objective cross-sectional evaluation of donor and recipient site up to 4 years. Clin Oral Implants Res. 2011; 22:1320-1326 https://doi.org/10.1111/j.1600-0501.2010.02115.x
De Stavola L, Tunkel J A new approach to maintenance of regenerated autogenous bone volume: delayed relining with xenograft and resorbable membrane. Int J Oral Maxillofac Implants. 2013; 28:1062-1067 https://doi.org/10.11607/jomi.2726
Urban IA, Nagursky H, Lozada JL Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: a prospective case series in 22 patients. Int J Oral Maxillofac Implants. 2011; 26:404-414
Aloy-Prosper A, Penarrocha-Oltra D, Penarrocha-Diago M, Penarrocha-Diago M The outcome of intraoral onlay block bone grafts on alveolar ridge augmentations: a systematic review. Med Oral Patol Oral Cir Bucal. 2015; 20:e251-258 https://doi.org/10.4317/medoral.20194
Wang J, Luo Y, Qu Y, Man Y Horizontal ridge augmentation in the anterior maxilla with in situ onlay bone grafting: a retrospective cohort study. Clin Oral Investig. 2022; 26:5893-5908 https://doi.org/10.1007/s00784-022-04547-1
Smeets R, Matthies L, Windisch P Horizontal augmentation techniques in the mandible: a systematic review. Int J Implant Dent. 2022; 8 https://doi.org/10.1186/s40729-022-00421-7
Considerations for the Management of Early Complications in Bone Regeneration: A Case Report Gonzalo Delgado Jonathan Meza‑Mauricio Erick Valdivia Andrea Vergara‑Buenaventura Dental Update 2025 51:9, 626-630.
Authors
GonzaloDelgado
Postgraduate student, Department of Periodontology, School of Dentistry, Universidad Peruana de Ciencias Aplicadas, Lima, Peru.
This case report evaluates the possible reasons for early complications after guided bone regeneration, as well as options for their management. A thorough evaluation prior to surgery will help determine appropriate planning. Each clinician should be aware of the goals and possible limitations of the treatment to be performed to ensure optimal patient care. The management of the membrane, early exposure and contamination with a second bone augmentation surgery provided a sufficient amount of bone to place a dental implant in a correct three-dimensional position.
CPD/Clinical Relevance: The correct approach for the management of the complications for regenerative bone therapy is highlighted.
Article
Bone graft techniques are surgical procedures to promote new bone formation. They are widely used to treat periodontal defects and atrophic bone ridges.1,2 Among the different interventions, the most commonly used are those based on guided regeneration using a bone graft or substitutes with a barrier membrane.3
Guided bone regeneration (GBR) has been shown to be a predictable technique for increasing the volume and quality of lost bone, allowing the posterior placement of dental implants.4,5 However, some biological principles (PASS principle, i.e. primary wound closure, angiogenesis, space maintenance and stability of the blood clot) should be considered.6 Some potential complications, such as infection, soft tissue complications, inflammation, delayed healing and pain, can occur during the healing process.7,8 Wound healing complications after bone grafting procedures are one of the main concerns for clinicians.8 One of the most frequent is membrane exposure, mainly when non-resorbable membranes are used. This may force the operator to remove it with the possible compromise of bone regeneration.5 It has been reported that when there is soft tissue dehiscence and membrane exposure, bone formation can be up to six times less than in nonexposed areas.9
The success of the procedure relies on various factors, including proper surgical technique, the selection of appropriate graft materials and barrier membranes, and patient compliance.8
This report discusses the management of wound healing complications after a GBR procedure. Furthermore, the authors provide insights into how to reduce the risk of such complications in future cases, providing some recommendations.
Case report
A 33-year-old female patient with no medical history attended the periodontal service of the Centro Universitario de Salud of the Universidad Peruana de Ciencias Aplicadas (CUS-UPC) for bad odour after a GBR procedure in the anterosuperior sector.
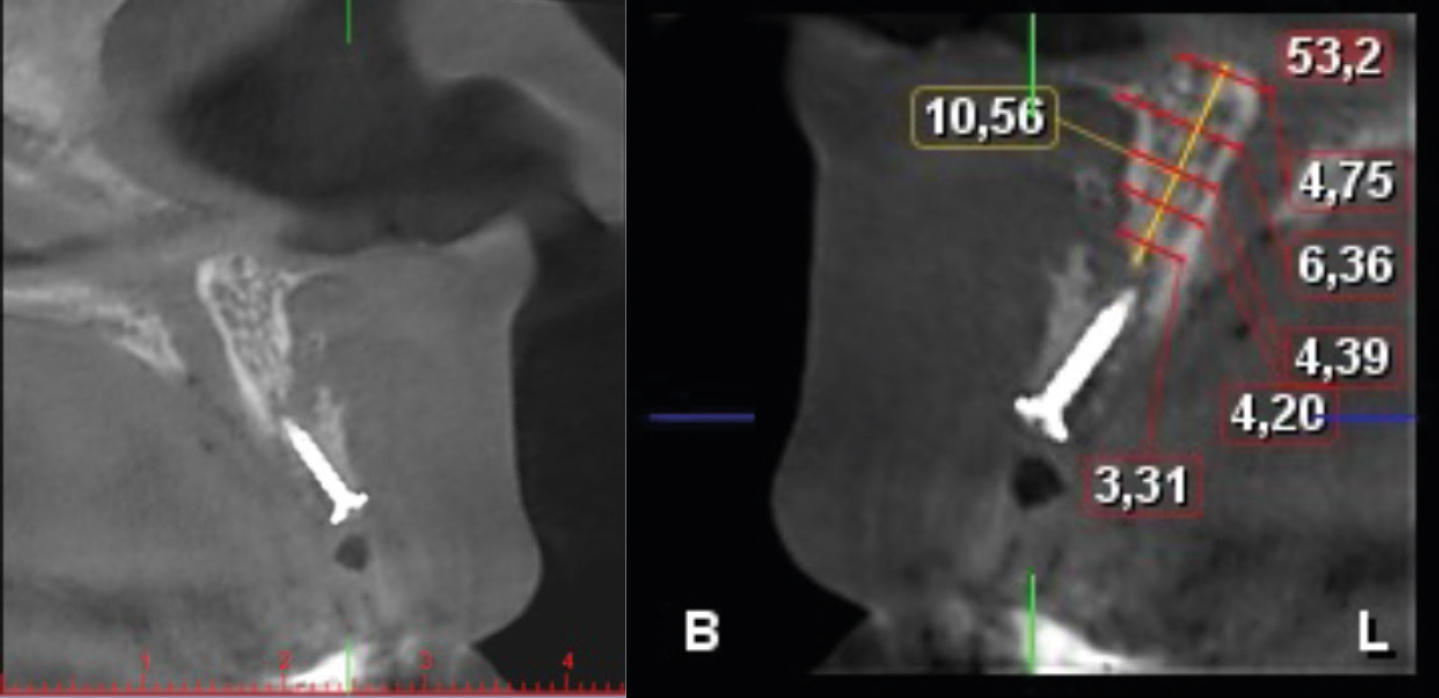
On clinical examination, the patient reported pain in the surgical area and the presence of slight wound dehiscence was observed with membrane exposure 2 weeks after a GBR procedure at UR1 (Figure 1). CT scan examination showed previous bone reconstruction with bone deficiency (Figure 2). After explaining the case considerations to the patient, and obtaining the patient's written consent, a disinfection protocol was performed with iodopovidone and 0.9% saline solution. Antibiotics (75 mg amoxicillin plus 125 mg clavulanic acid twice daily for 10 days) were prescribed along with a 0.12% chlorhexidine gluconate rinse twice daily for 14 days. The patient underwent periodic check-ups every week.
Figure 1. Slight dehiscence of the wound with exposure of the membrane at UR1.Figure 2. CT scan showing previous osseous treatment, but with horizontal and vertical deficiency of the alveolar ridge.
After 1 month of follow up, the patient reported an absence of pain. However, a control CT scan confirmed considerable volume loss at the surgical site. After analysing the case, the width of the ridge did not allow for the adequate three-dimensional placement of dental implants. Thus, it was decided to re-enter the surgical site and perform an intra-oral autogenous block graft to obtain sufficient horizontal and vertical volume for the future placement of an implant (Figure 3).
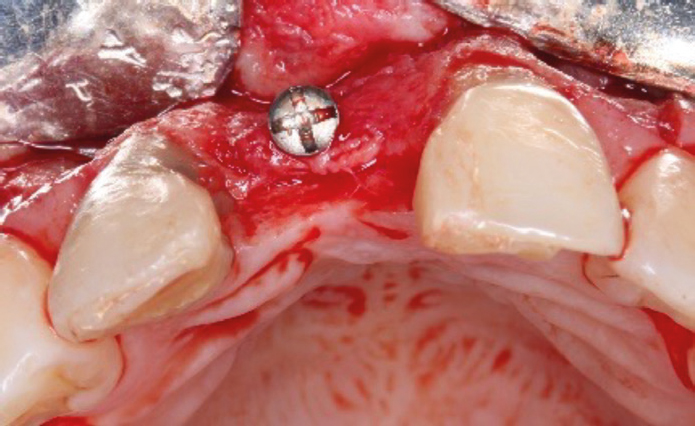
Figure 3. The clinical situation prior to the new bone augmentation surgery. Extensive vertical loss can be observed.
Local anaesthesia was performed (1% lidocaine with 1: 80,000 epinephrine) and Intra-sulcular incisions were made from teeth UR2 to LR2 with papilla preservation technique to raise a mucoperiosteal flap.
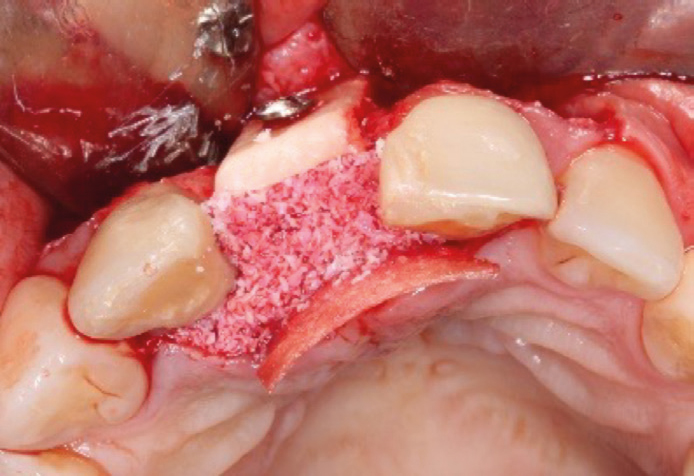
A vestibular incision technique was used to access the mandibular ramus and to obtain the autogenous block graft using a piezoelectric device. The block graft was adjusted over the recipient site with fixation screws to achieve close contact with the underlying host bone. Then, 0.5 cm3 of xenogenic particulate bone (The Graft, Purgo Biologics, Korea) was placed at the recipient site (Figure 4) and covered with a type I collagen membrane (20 × 30 mm, Neomem, Citagenix Inc, Canada) to guarantee greater vestibular-palatal volume in the area. Both flaps were closed using simple interrupted and sling sutures with blue nylon 5/0.
Figure 4. Occlusal view of the branch block graft fitted in the recipient site with fixation screws and subsequent placement of particulate bone.
Dexamethasone (4 mg/2 ml) and diclofenac (75 mg/3 ml) were prescribed for 3 days, and etoricoxib (120 mg) once a day if necessary, for pain control. The same antibiotic and oral antiseptic protocol was prescribed. Also, the patient was instructed to eat soft food, put cold packs on the area, and avoid exercise for 7 days.
The site was checked at 4 and 7 days post-procedure and there were no clinical signs of infection, and bone volume was preserved. The sutures were removed after 14 days.
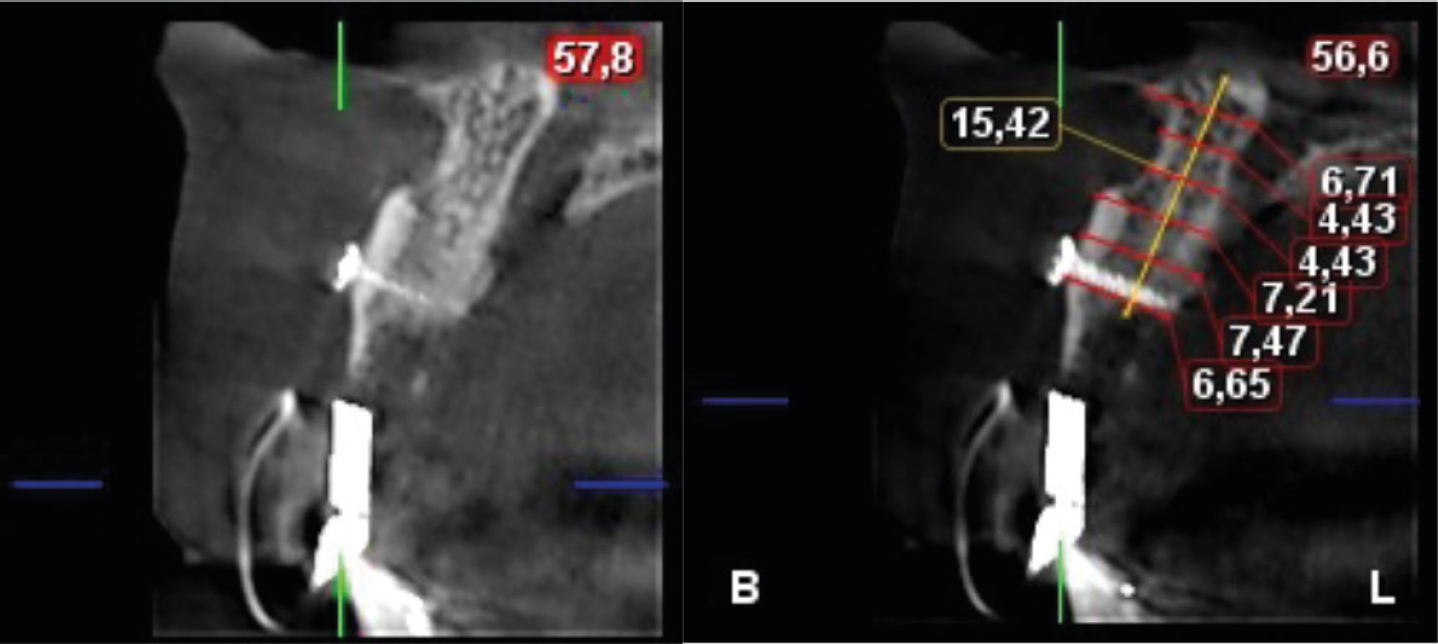
After 5 months, the bone augmentation of the area was evaluated by cone beam computed tomography and a gain of approximately 2.5 mm of bone was found horizontally. Placement of a dental implant could therefore be planned (Figure 5).
Figure 5. CBCT scan after 5 months showing successful horizontal bone regeneration.
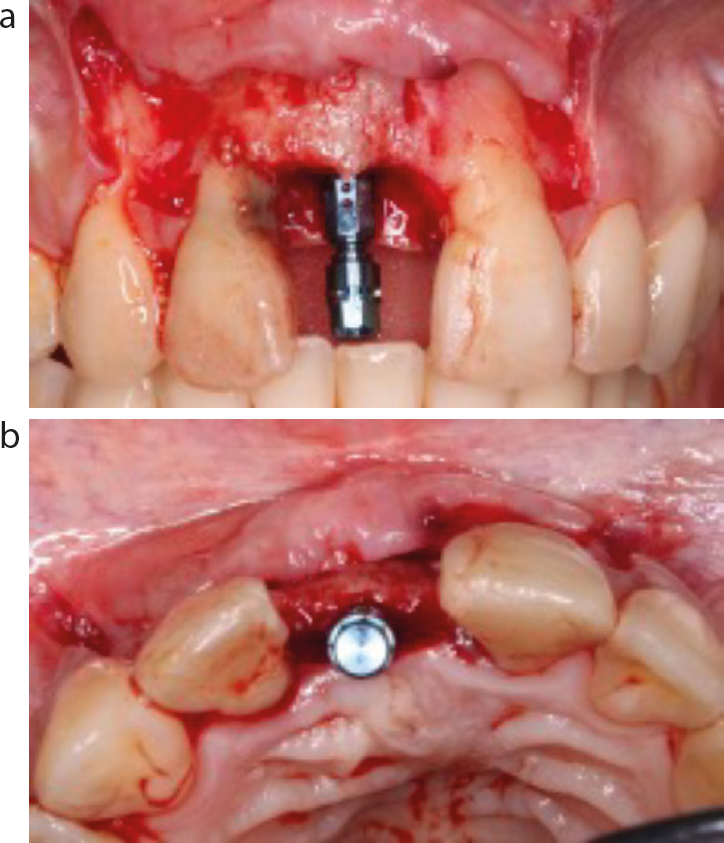
Surgical re-entry was performed using a mucoperiosteal flap elevation. The fixation screws were removed, and a dental implant (3.3 × 12 mm; SLActive, Straumann, Switzerland) was placed following the manufacturer's protocol with an initial stability of 35N (Figure 6). Then, a soft tissue graft from the tuberosity was placed in the zone and stabilized with horizontal mattress sutures with polyglycolic acid 6/0.
Figure 6. (a,b) Pictures showing the placement of a 3.3 × 12 mm implant.
Post-operative recommendations and medication protocols were the same as for the previous surgery.
Discussion
Several techniques have been proposed to increase bone in deficient ridges. GBR is the most commonly used technique, and involves the use of graft materials and a barrier.3 Other techniques include the use of an autogenous block bone graft,10,11 split ridge,12 and distraction osteogenesis.13 All techniques are effective, but complications can arise during the healing phase of treatment, generating undesirable results.8,14
This article presents an early complication of GBR for horizontal bone gain that had used particulate bone, which was subsequently treated with an autogenous en block graft for placement of a dental implant in the upper anterior area.
Horizontal augmentation surgeries are considered easier to treat and tend to have a lower incidence of complications than vertical augmentation because they have a larger bone contact area for graft vascularization and containment.2 However, its success depends on four fundamental principles (primary closure, space maintenance, angiogenesis and wound stability) that must be followed during surgery and the healing phase.6 The soft tissue complication rate after GBR has been reported to range from 0% to 45%, which includes soft tissue dehiscence, acute infections and abscesses, and can occur during the first week or months after treatment.3,8
The surgeon's experience and skill in both planning the surgery, and the ability to achieve a tension-free primary closure is crucial in the success of regenerative procedures.15,17 To guarantee this, the clinician should evaluate the type and size of the bone defect, tissue biotype, incision design, amount of keratinized tissue, vestibular depth, and flap flexibility during planning.16
Primary wound closure can be achieved using a buccal split flap, which provides a greater amount of tissue in the vertical direction.18 The use of one vertical incision could allow 1.1 mm of flap advancement, two vertical incisions of a further 1 mm, and the use of a periosteal releasing incision could provide 5.5 mm more.19 Flap flexibility has been compromised in cases of shallow vestibule depth, limiting the approximation of the flap edges.16 On the other hand, the biotype and width of the keratinized tissue can determine the flap's resistance to tearing and tension during suturing.20 It has been shown that when the width of the keratinized tissue is less than 3 mm, the incidence of wound opening increases twofold.21 Concerning flap thickness, thicker flaps (≥1 mm) have been found to provide better mechanical strength than thin flaps.16,20 Another factor to consider is the mechanical properties of the sutures. Flap trauma can be reduced by choosing suture materials with smaller diameters.20,22
The present case describes a complication following GBR treatment where mucosal dehiscence occurred with membrane exposure and contamination. This early complication may compromise space maintenance and, therefore, GBR outcomes.23,24 Resorbable membrane exposure usually results in rapid resorption (as a result of enzymatic degradation and oral flora activity), with the possibility of secondary-intention epithelialization, uneventful healing and inadequate bone formation3,24 compared to membranes that remain submerged during healing.9,25 When a membrane is exposed, contamination can lead to post-surgical infections that require early removal of the barrier membrane. On the other hand, the use of non-resorbable rigid membranes has been associated with earlier exposure owing to the tendency of the membrabe to return to its original shape after adaptation at the site of the bone defect.16 Treatment of the area helps to minimize the negative effects. In cases of exposure and infection, removal of the membrane and the use of systemic antibiotic therapy is recommended.
The primary objective in the present case was to gain bone in the horizontal direction for future implant placement. However, the previous complication led to horizontal and vertical bone loss causing a more challenging surgery as a result of the large combined bone defect.
Autogenous bone grafts are considered a reliable option for the treatment of mild, moderate and severe bone defects,26 and are considered the gold standard for their osteogenesis, osteo-induction and osteoconduction properties.27,28 According to Plonka et al29 GBR has demonstrated an average vertical and horizontal bone augmentation of 3–5 mm (depending on donor site availability). Autogenous grafts have demonstrated predictability in atrophic ridge reconstructions prior to implant placement regardless of the donor and recipient site.28
In the present case report, the mandibular ramus was taken as the donor site. Although it has been reported that the amount of cortico-cancellous bone is superior when harvested from the chin area,30 several studies report that chin harvesting is associated with greater post-operative morbidity, and a greater number of complications.30,31,32 One of the main disadvantages of using an autogenous bone graft is the significant bone resorption during healing.33 Therefore, bovine bone particles were used together with to minimize this resorption.34
Success and survival rates of implants placed in resorbed edentulous ridges reconstructed with bone grafts are similar to those of implants placed in pristine bone.35 The mean bone gain after placement of an autologous block graft was 2.5 ± 1 mm horizontally, which is in agreement with the values reported in the literature.11,33,36,37 This second surgery provided a sufficient amount of bone in which to place a dental implant in a correct three-dimensional position.
Bone regeneration of large oral bone defects is a clinical challenge for the clinician. Even more so for those caused after an accident or a previous surgical complication. A complete evaluation of the soft tissues before surgery will help determine proper planning for desired healing. Although the literature has reported increased complications and morbidity, autologous block grafts remain a reliable option for treating horizontal bone defects. Each clinician must be aware of the goals and possible limitations of the treatment to be performed to ensure optimal patient care.