Ericson S, Kurol J. Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur J Orthod. 1986; 8:133-140 https://doi.org/10.1093/ejo/8.3.133
Dachi SF, Howell FV. A survey of 3,874 routine full-mouth radiographs. II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol. 1961; 14:1165-1169 https://doi.org/10.1016/0030-4220(61)90204-3
Mossey PA, Campbell HM, Luffingham JK. The palatal canine and the adjacent lateral incisor: a study of a west of Scotland population. Br J Orthod. 1994; 21:169-174 https://doi.org/10.1179/bjo.21.2.169
Brin I, Becker A, Shalhav M. Position of the maxillary permanent canine in relation to anomalous or missing lateral incisors: a population study. Eur J Orthod. 1986; 8:12-16 https://doi.org/10.1093/ejo/8.1.12
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:249-156
Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005; 128:418-423 https://doi.org/10.1016/j.ajodo.2004.04.033
Stivaros N, Mandall NA. Radiographic factors affecting the management of impacted upper permanent canines. J Orthod. 2000; 27:169-173 https://doi.org/10.1093/ortho/27.2.169
Ericson S, Kurol J. Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. A clinical and radiographic analysis of predisposing factors. Am J Orthod Dentofacial Orthop. 1988; 94:503-513 https://doi.org/10.1016/0889-5406(88)90008-x
Liu DG, Zhang WL, Zhang ZY Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:91-98 https://doi.org/10.1016/j.tripleo.2007.01.030
Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987; 91:483-492 https://doi.org/10.1016/0889-5406(87)90005-9
This orthodontic case report highlights the unpredictable behaviour of ectopic maxillary permanent canines. An 11-year-old male patient had bilateral ectopic maxillary canine teeth that were in high positions and initially left in situ and monitored. During orthodontic treatment, there was rapid spontaneous eruption of both teeth with resulting resorption to an adjacent lateral incisor. This case report details the clinical findings and progress of treatment and management. A review of the literature reinforces the importance of maintaining regular radiographic review to assess for migration of ectopic teeth, and to ensure appropriate treatment planning and assessment of potential complications.
CPD/Clinical Relevance: This report highlights the need for regular radiographic review of impacted canines in younger patients.
Article
Maxillary impacted canines have a high developmental position and long path of eruption, with canine impaction and non-eruption being a common problem. The incidence of impacted canines is well reported in the literature at between 1% and 3% of the population.1,2 Impaction is more common in females, with a ratio of 7:3, with 8% of cases being reported as bilateral impactions.3,4 The majority of the literature states that impacted canines are most commonly found to be palatally positioned, with reports varying between 41% and 85%.1 The presence of a lateral incisor seems to be important for eruption guidance of the canine, with a higher incidence of canine impaction when the lateral incisor is absent or diminuitive.5 Canine impaction is also more common with Class 2 division 2 malocclusions.3,6 It is important to establish the location of impacted maxillary canines as part of the orthodontic assessment and treatment planning process, as well as the presence of any associated pathology. The position of the impacted canine will determine the prognosis for, and complexity of, alignment.5
Complications of impacted maxillary permanent canines are well reported in the literature and include resorption and damage to adjacent structures, as well as cystic change.7 The most relevant complication to this case report is the resorption of the adjacent lateral incisor root. Root resorption of these teeth is most likely to occur between the ages of 11 and 12 years, making it an important age range for clinical supervision.8 One study9 suggests that 12.5% of impacted maxillary canines can cause root resorption of adjacent incisors when assessed with conventional radiographic imaging. A higher incidence of lateral incisor resorption can be detected with 3D imaging (cone beam CT), with a suggested resorption rate of between 27% and 67%, and up to 11–23% of central incisors.10 It is therefore important to assess the presence and extent of resorption when orthodontic treatment planning, especially when orthodontic extractions are required as part of the plan.
In view of the potential for resorption and pathology in relation to impacted canine teeth, it is therefore sensible to monitor these teeth if the treatment plan involves leaving them in situ. This case report highlights the importance of this approach, and the potential for complications in situations even when they may have seemed unlikely at initial assessment.
Case report
An 11-year-old male patient of European origin was referred by a specialist orthodontic practice to the hospital orthodontic service. The patient's main concern was in relation to the appearance of the gaps in his teeth. There was nothing of note in his medical history and he was a regular attender at his dentist.
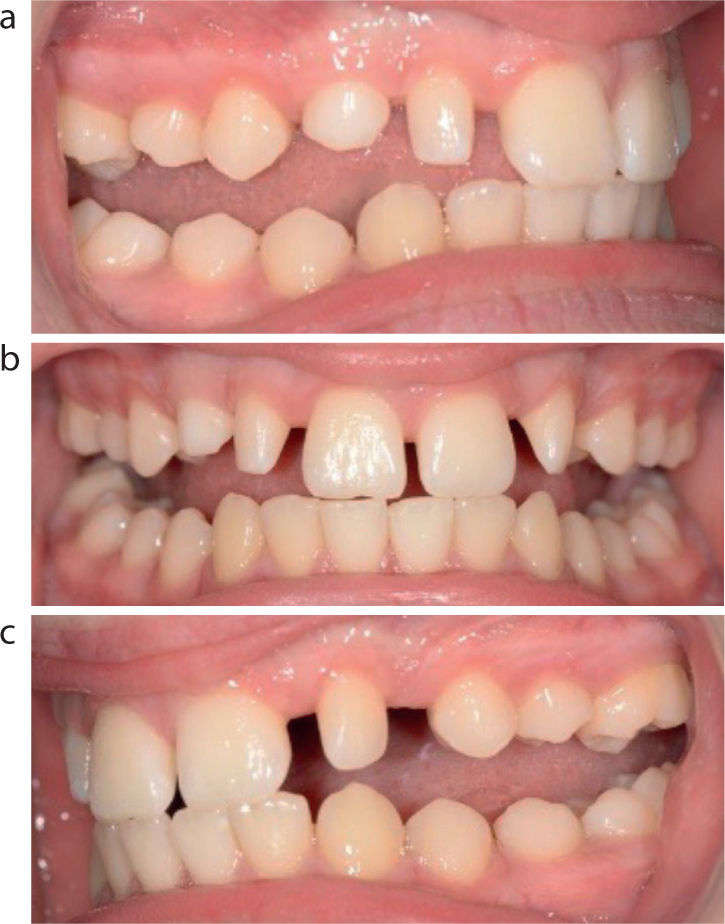
On clinical assessment he presented with a Class II division 1 incisor relationship on a Class II skeletal pattern with average vertical proportions. Clinically, the upper permanent canines remained unerupted and he had a retained upper right deciduous canine. The lower arch was noted to be well aligned with spacing evident in the upper incisor region, with slightly diminutive upper lateral incisors. In occlusion, he had an increased overjet recorded clinically at 11 mm and a complete overbite recorded at 90% (Figure 1).
Figure 1. Pre-assessment photographs.
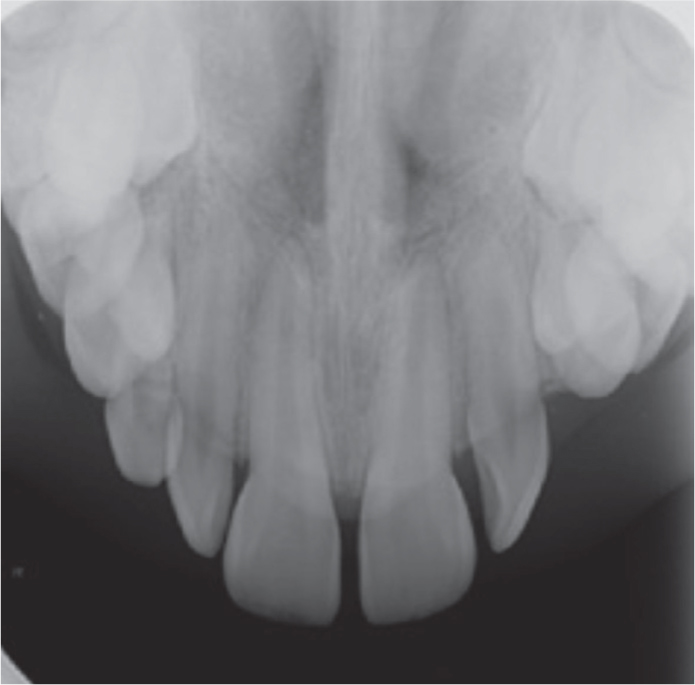
Radiographic assessment with an orthopantomograph confirmed the presence of all permanent teeth except the lower third molars (Figure 2). Both upper permanent canines were ectopic and in high horizontal positions apical to the erupted upper anterior teeth. Vertical parallax using an upper anterior occlusal view confirmed they were buccally positioned (Figure 3).
The patient was subsequently reviewed jointly with surgical colleagues from the oral and maxillofacial (OMFS) department regarding the ectopic upper permanent canine teeth. In view of the high position of the ectopic canine teeth, they were not favourable for surgical exposure and orthodontic alignment. Therefore, the options of leaving the teeth with monitoring, as well as surgical removal, were discussed with the patient, including the associated risks/benefits of both options. Following this discussion, the patient opted to leave the upper canines in situ, with a further review with the surgical team after 12 months. To manage the patient's Class 2 malocclusion, it was agreed to begin orthodontic treatment with a twin-block functional appliance prior to re-assessment and progression to fixed appliance treatment.
The patient made good progress with the twin block appliance and after 12 months, had achieved full reduction of overjet and overbite and correction of the buccal segment relationships to Class 1 (Figure 4). At this stage, the patient was reviewed again with surgical colleagues. An updated lateral cephalogram showed no significant change in the high ectopic positions of the canines (Figure 5) and, following further assessment and discussion, it was agreed that the upper permanent canines would continue to be left in situ and monitored. The patient was also reviewed by restorative specialists who arranged composite build ups of his slightly diminutive upper lateral incisors. The updated orthodontic plan was agreed with the patient to progress to upper and lower fixed appliances to achieve space closure of both arches following the loss of the upper right deciduous canine.
Figure 4. After functional appliance treatment.Figure 5. Lateral cephalogram at the end of functional appliance phase.
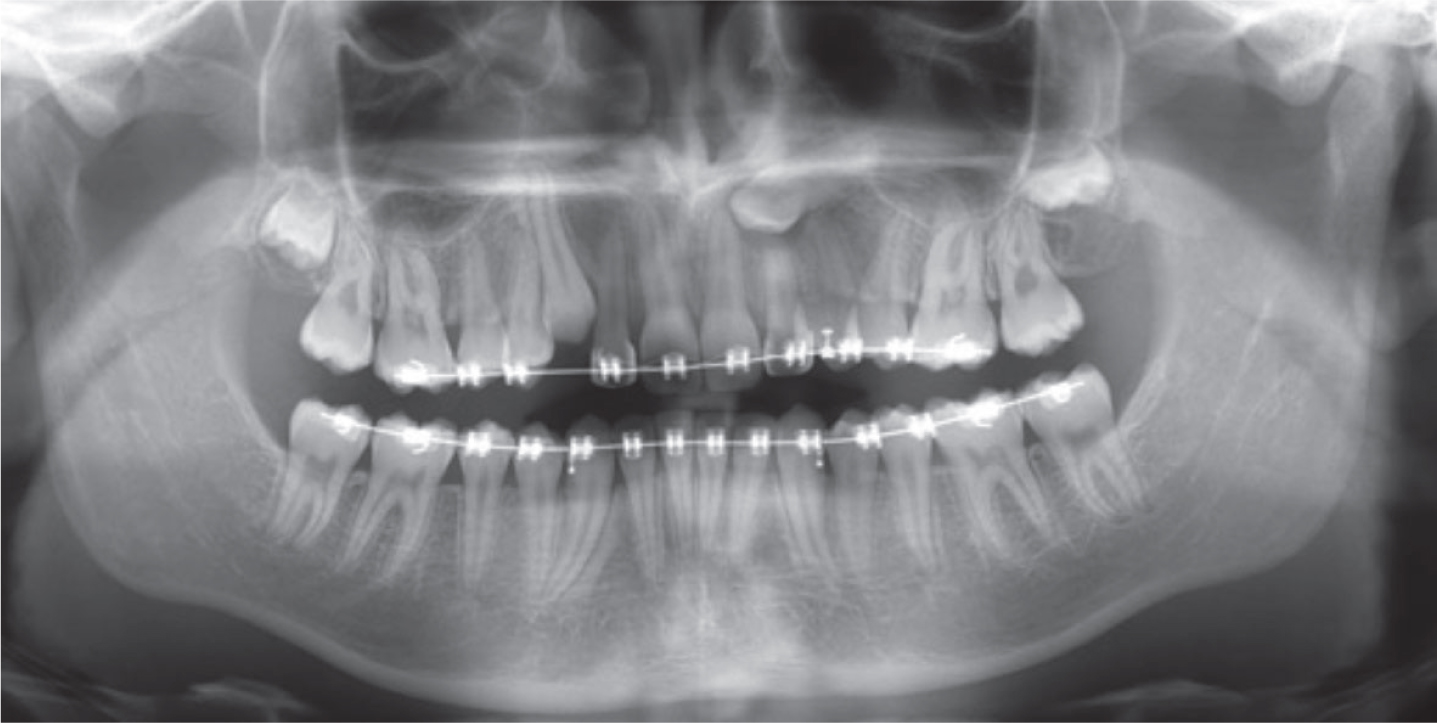
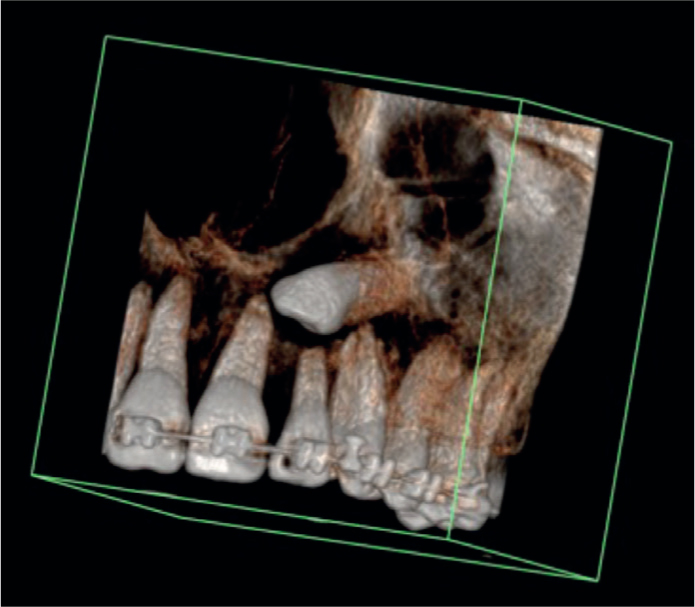
Approximately 13 months into fixed appliance therapy, a buccal bulge was seen clinically in the UR3 region. Updated radiographic assessment with an OPG (Figure 6) revealed migration of both upper permanent canines. The UR3 had uprighted and was in a good position for spontaneous eruption between the upper right lateral incisor and first premolar. The UL3 had also uprighted and moved occlusally, but remained impacted on the apical aspect of the upper left lateral and central incisors. Possible signs of root resorption were evident on the OPG, particularly affecting the UL2 (Figure 6). Cone beam 3D imaging confirmed root resorption of the apical third of the upper left lateral incisor and possible early resorption of the upper left central incisor (Figure 7).
Figure 6. Mid-treatment OPT showing migration of both upper canines.Figure 7. 3D CBCT confirming resorption at UL2.
The patient was reviewed with surgical colleagues and following discussion of options, it was agreed to surgically remove the upper left canine due to its poor position and potential for further resorption, and to expose and align the upper right canine in view of its favourable position. The patient subsequently had surgery carried out successfully, and a further 10 months of orthodontic treatment (Figure 8) before completion of treatment and the achievement of a satisfactory aesthetic and functional result (Figure 9). The patient was very happy with the outcome, and happy to accept that the upper centreline remained slightly displaced to his left. The option of considering a premolar extraction in the upper right quadrant was discussed during treatment to maintain arch symmetry, but was declined by the patient. A further radiograph was taken post-treatment to assess the apical resorption status of UL2 and for monitoring purposes (Figure 10).
The removal of a primary canine between the ages of 11 and 13 years can result in an improvement in the position of a palatally ectopic canine.11 Although in this case report, the canines were in a buccal position, the patient was within this suggested age range and loss of the upper right deciduous canine tooth may have accounted for the improvement of its position. Similar situations have been observed by Brown and Sandy who reported a case of a patient of similar age with canines in unfavourable positions, which also resulted in a surprising improvement of position.12 This builds further on what is suggested by Kindelan and Cook, that maxillary canines in unfavourable positions be monitored for a period of time radiographically to assess for changes in position.13
The British Orthodontic Society (BOS) radiographic guidelines does not recommend taking 3D imaging routinely when assessing impacted canines. Conventional imaging with an orthopantomograph is suggested, and a supplementary intra-oral view can be used to check the position with parallax and to assess for pathology including resorption.14
Following orthodontic assessment, if the canines are deemed to be in unfavourable positions for alignment, then option appraisal and discussion with the patient will include leaving these teeth in situ with periodic radiographic monitoring to check for developing pathology, such as resorption, or to consider surgical removal of these teeth to avoid the potential for future pathology. The BOS highlights and discusses these options in a patient information leaflet, with the recommendation of periodic follow up for those teeth left in situ.15 At present, there is no clear evidence-based guidance about the frequency of recommended follow up and radiographic monitoring of these impacted teeth.
This case study highlights the potential for spontaneous eruption of impacted canines and subsequent resorption of adjacent teeth over a relatively short time scale. It confirms that regular radiographic monitoring of canine teeth during their active eruption stage (dictated by dental age, but generally 11–14 years of age) is indicated, with this case report suggesting a 12-month time frame for repeat imaging in view of the rapid eruption potential. In older adult patients, if an ectopic tooth has no associated pathology, then regular repeat imaging is probably not indicated unless clinical signs or symptoms of pathology develop.
Conclusion
It is difficult to predict the behaviour of an impacted maxillary canine left in situ in a growing patient. The impacted tooth should therefore be carefully monitored by the orthodontist or supervising GDP, clinically and radiographically, to review for changes in position and to assess the impact on adjacent structures. The present case report suggests that repeating the radiographic assessment after 12 months in a growing patient would be justifiable given the potential for eruption of an impacted tooth over a relatively short time period and the risk of associated pathology.