Escoda Francolí J, Almendros Marqués N, Berini Aytés L, Gay Escoda C Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2008; 13:E438-443
McCrea SJ Nasopalatine duct cyst, a delayed complication to successful dental implant placement: diagnosis and surgical management. J Oral Implantol. 2014; 40:189-195 https://doi.org/10.1563/AAID-JOI-D-12-00011
Shylaja S, Balaji K, Krishna A Nasopalatine duct cyst: report of a case with review of literature. Indian J Otolaryngol Head Neck Surg. 2013; 65:385-388 https://doi.org/10.1007/s12070-011-0242-6
AlQahtani M, AlDossari A, Nasser A Nasopalatine duct cyst: a diagnostic dilemma. Dent Oral Craniofacial Res. 2018; 4:1-6
This case report describes the presentation of a nasopalatine duct cyst in a 27-year-old orthodontic patient. The patient presented with pain in the anterior hard palate and a Class II division 2 occlusion with a complete overbite. The cyst was discovered upon further radiographic investigation. Following discussion at a joint orthognathic clinic, the decision was made to leave the cyst under active monitoring and review the patient clinically and radiographically after 12 months.
CPD/Clinical Relevance:
Nasopalatine duct cysts are common, therefore awareness of their clinical and radiographic features and treatment options is essential.
Article
Accounting for approximately 1% of all maxillary cysts, nasopalatine duct cysts (NPDCs) are the most common type of epithelial lined non-odontogenic cystic lesion of the oral cavity.1 Arising from the midline of the anterior palate, it is believed their origin is from the embryonic remnants of the nasopalatine duct, which ordinarily undergoes progressive degeneration.2 They mostly occur between the fourth and sixth decades of life and are more frequent in males than females (3:1).3
While the aetiology of NPDCs remains unknown, factors attributed to the cause of these cysts include local trauma to the area during mastication, ill-fitting prosthesis, bacterial infection, spontaneous proliferation, and blockage of glandular tissue.1
NPDCs are usually asymptomatic, typically being discovered as an incidental finding on a radiograph or during routine examination.4 If a patient does present with symptoms, the most common is swelling of the anterior palate at the incisive papilla. Other reported symptoms include intermittent pain, itching or a burning sensation of the anterior palate which is likely due to compression of the nasopalatine nerve.1,4,5 Resorption of overlying bone can result in a fluctuant swelling with a blue appearance, a foul taste may be reported if there is associated mucoid discharge.4
Radiographically, lesions are well-defined radiolucencies with a rounded or heart-shaped appearance (owing to superimposition of the nasal spine) and centered apically to the midline of the upper central incisors.1
Differential diagnoses for NPDCs include peri-apical pathosis or a radicular cyst. Owing to their radiographic appearance, NPDCs can often be misinterpreted as a peri-apical lesion, and it is not uncommon to see evidence of unnecessary endodontic intervention of these teeth.6 It is therefore paramount that further investigations are undertaken to exclude a lesion of peri-apical origin through the use of percussion and sensibility testing. This will allow for correct treatment planning and prevention of unnecessary treatment on a potentially vital tooth.5
Case report
History
A 27-year-old male was seen in the orthodontic department of a local hospital following referral from a general dental practitioner (GDP). The referral was for the assessment of a traumatic overbite with evidence of soft tissue trauma. On presentation, the patient's main concern was pain of the anterior hard palate region for the previous 1–2 years when clenching his teeth. His GDP had taken bitewing and peri-apical radiographs and provided him with a soft occlusal splint.
Medically, the patient had autism and difficulties with physical contact. His medication included fluoxetine, and he did not have any known drug allergies. He smoked 10–15 roll-ups per day and consumed around 10 units of alcohol per week.
Extra-oral assessment
Extra-oral examination revealed a Class II skeletal pattern with a slightly reduced Frankfort mandibular plane angle and a decreased lower anterior face height. There was a bilateral click of the temporomandibular joint (TMJ) and the patient reported previous episodes of locking of the TMJ on eating. Maximum mouth opening was 47 mm and there was no deviation of the mandible on opening.
Intra-oral assessment
Intra-orally the soft tissues looked healthy on examination; however, there were no visible indentations on the anterior hard palate relating to the lower incisors or evidence of palatal trauma. At the time of the assessment, the patient did not report any intra-oral pain on clenching his teeth. Oral hygiene was poor and required generalized improvement. He had a moderately restored dentition with evidence of attrition and erosion. Dental caries was identified interproximally on the upper right and upper left central incisors, and the lower right canine. The upper anterior teeth were tested to Endo Frost spray and electric pulp testing, all responding positively to both tests. The lower right and left second molars were absent. A basic periodontal examination score of 3s was given in all sextants other than the lower anteriors, which had a score of 2.
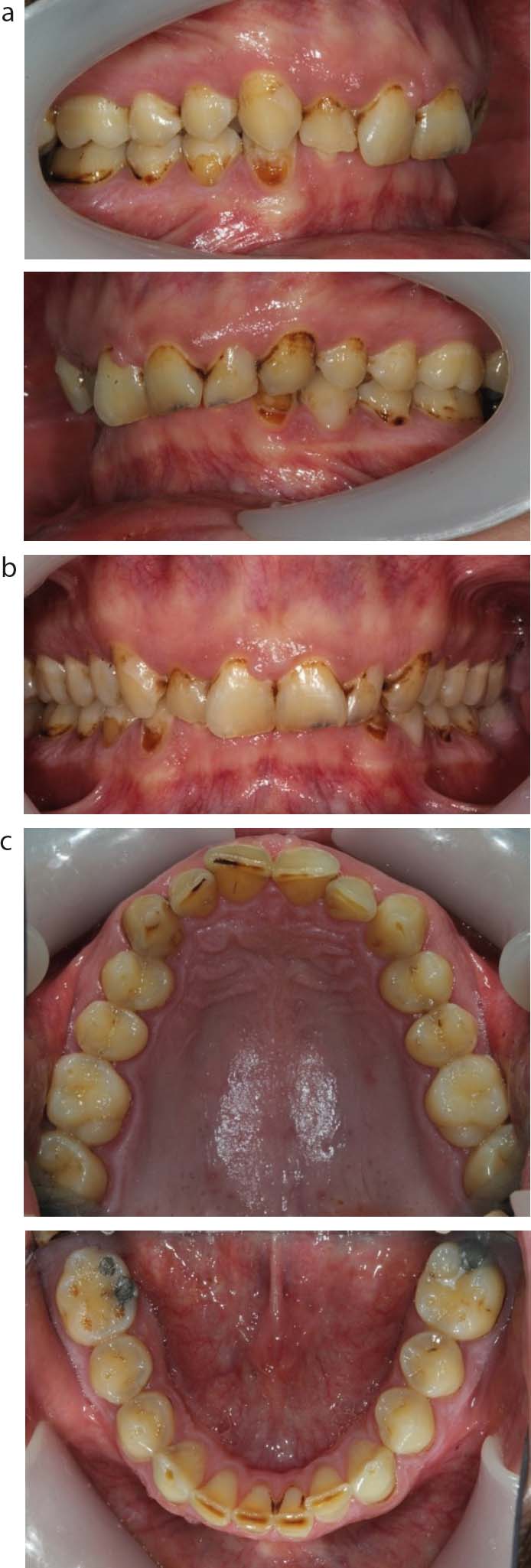
The patient had a Class II division 2 malocclusion with a 4-mm overjet and complete overbite (Figure 1). The upper labial segment was retroclined with mild crowding. The lower labial segment was also retroclined with a slightly increased curve of Spee and mild crowding.
Figure 1. Intra-oral lateral views showing a Class II division 2 occlusion. (b) Frontal view with a deep anterior overbite with the maxillary incisors covering 100% of the crowns of the mandibular incisors. (c) Occlusal views showing evidence of tooth surface loss and mild crowding of the upper and lower labial segments.
An Index of Orthodontic Treatment Need (IOTN) score of 3f was given for a deep overbite on palatal tissues, but without evidence of trauma. Orthodontic intervention would not be currently indicated owing to the patient's periodontal condition and the presence of caries.
Radiographic assessment
An orthopantomogram was taken to aid examination and diagnosis. This revealed a discrete well-defined radiolucency between the roots of the upper central incisors (Figure 2). Maxillary standard occlusal and peri-apical radiographs were taken of the upper anterior portion of the maxilla. These demonstrated a midline radiolucency with a well-defined and corticated lateral margin overlying the apical third of the root of the upper right central incisor. There was no sign of root resorption or displacement of the roots, and the periodontal ligament (PDL) space was even, with an intact lamina dura.
Figure 2. Maxillary occlusal radiograph displaying a radiolucency between the roots of the maxillary central incisors. (b) Peri-apical radiograph displaying a well-defined round radiolucency overlying the roots of the maxillary central incisors. (c) Lateral cephalogram radiograph showing a Class II skeletal pattern. (d) Orthopantomogram radiograph showing a mildly restored permanent dentition and a visible radiolucency between the maxillary central incisors.
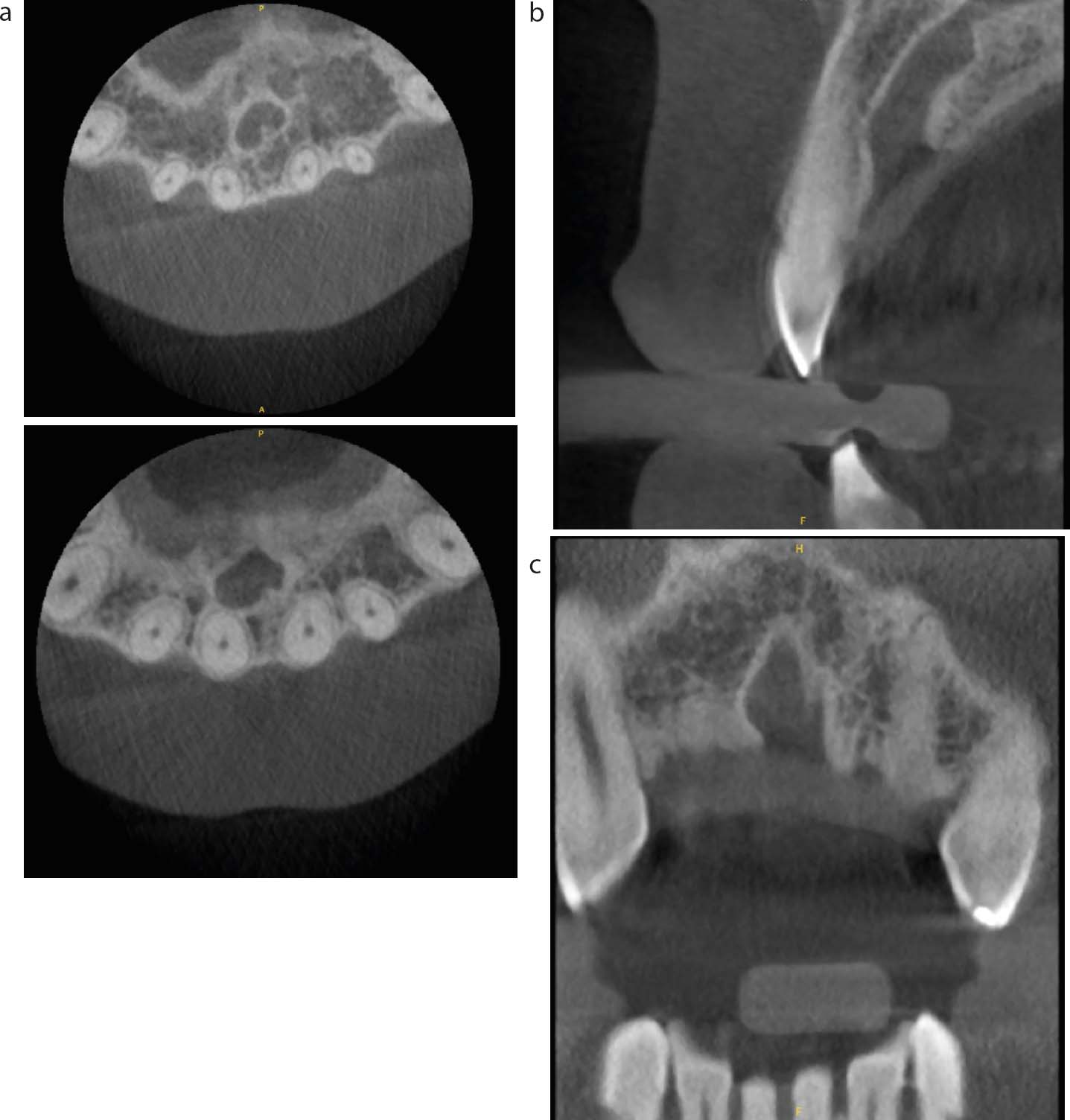
A cone beam computed tomography (CBCT) scan was carried out to aid in the diagnosis of the radiolucent lesion shown on the plain film radiographs. This was reported by a radiologist specializing in the maxillofacial region. The CBCT exhibited widening of the incisive canal towards the alveolar crest, with a maximum dimension of 7 mm (Figure 3). No root resorption or displacement was seen in the roots of the adjacent upper central incisors. The PDL space of both upper central incisors was intact and not communicating with the radiolucency or the incisive canal. The imaging findings were in keeping with a NPDC.
Figure 3. Axial sections of a CBCT scan of the anterior maxilla showing the heart shape appearance of the NPDC. (b) Sagittal section showing widening of the incisive canal towards the alveolar crest. (c) Coronal section displaying a radiolucent area in the midline of the anterior palate between the two upper central incisors.
Treatment
Based on clinical and radiographic findings the primary diagnosis was NPDC; however, differential diagnoses included radicular cyst and central giant cell granuloma. The patient was seen on a nurse-led oral hygiene clinic where his diet was assessed and modifications suggested, records (intra-and extra-oral images and a 3D intra-oral scan) were taken. The patient's GDP had commenced treatment regarding the patient's carious lesions, with appropriate periodontal and oral hygiene and dietary advice. The patient was provided with an upper removable appliance to wear at night and when symptomatic, with a flat anterior bite plane slightly relieved in the mid-palatal area.
The findings were discussed with the oral and maxillofacial consultants. The patient was then seen at a monthly joint orthodontic–maxillofacial clinic for treatment planning. After clinical review and discussion with the patient and maxillofacial consultant, the patient and team elected to leave the NPDC in situ for clinical monitoring with a further review after 12 months. At this time, further clinical evaluation and another CBCT scan would be undertaken to see whether there had been any increase in the size of the cyst and treatment options could be reviewed. Should the cyst continue to increase in size, or the symptoms fail to resolve, surgical excision would then be further considered. The patient was encouraged to contact the department should symptoms fail to resolve during that period.
Discussion
This case demonstrates the findings of a NPDC. While there was no clinically visible intra-oral swelling, the patient presented with a history of pain in the anterior hard palate region for the previous 1–2 years.
Radiographic investigations are imperative in the diagnosis of NPDCs. Usually occlusal or peri-apical radiographs are advised, in addition to an orthopantomogram. CBCT scans allow the structures to be visualized with great detail and are very useful in forming a tentative diagnosis.5 For this patient, a midline radiolucency was seen between the roots of the upper central incisors, which is a wellrecognized feature of NPDCs.
It has been proposed that NPDCs can be caused by local trauma to the anterior palate, such as mastication or an ill-sitting prosthesis. However, there is little in the literature surrounding the occurrence of NPDCs in patients with an orthodontic malocclusion, such as a deep traumatic overbite.
This case is particularly interesting clinically owing to the age of the patient at presentation. He presented with a NPDC in his third decade of life, which is earlier than described in the literature where NPDCs are most commonly reported in the fourth–sixth decades. While the patient's deep overbite may have been a contributory factor in the development of the cyst, equally it may also have made the patient aware of its presence at an earlier stage.
Treatment of symptomatic NPDCs most commonly involves complete surgical enucleation of the lesion, usually via a palatal approach under a general anaesthetic. For asymptomatic lesions, treatment is not usually recommended, as in this case. However, cysts larger than 2 cm in diameter may be progressive, and treatment is therefore necessary.7 Recurrence rates have been shown to vary between 0% and 11%.3,8
However there are no recognized criteria to enable determination of which cysts are most likely to re-occur.9
Conclusion
While the occurrence of NPDCs is relatively low, clinicians should be aware their clinical and radiographic presentation and management. Patients who present with a radiolucency of the anterior maxilla should undergo a thorough assessment of the vitality of the teeth and further radiographs should be taken to allow for differential diagnoses to be made. This is particularly important to prevent the unnecessary treatment of vital teeth, and enable appropriate treatment planning and management. This case report reinforces the importance of practitioners being aware of NPDCs, their clinical and radiographic features, differential diagnoses, and treatment options.