Burford D, Noar JH. The causes, diagnosis and treatment of anterior open bite. Dent Update. 2003; 30:235-241
Proffit WR, Fields HW.St Louis: CV Mosby; 2000
Chui San Teresa NG, Wong R. Orthodontic treatment of Anterior Open Bite. Int J Paed Dent. 2008; 18:78-73
Ferguson JW. The assessment and treatment of Anterior Open Bite. Dent Update. 1995; 22:163-168
Young-Chel Park, Han-Ah Lee, Nak Chun Choi Open bite correction by intrusion of posterior teeth with miniscrews. Angle Orthodontist. 2008; 78:(4)699-710
Sakai Y, Kuroda S. Skeletal Class 3 open bite treatment using implant anchorage. Angle Orthodontist. 2008; 78:(1)157-166
Anterior open bite has a multi-factorial aetiology comprising: genetically inherited skeletal pattern, soft tissue effect and digit-sucking habits. To formulate an appropriate treatment plan, accurate diagnosis is essential. Simple open bites may sometimes resolve completely during the transition from mixed to permanent dentition, if the digit-sucking habit is broken. More significant open bites, however, sometimes extending right back to the terminal molars, rarely resolve spontaneously and will often require complex orthodontic treatment, involving active molar intrusion or even major orthognathic surgery. Unfortunately, surgery has associated risks attached, including pain, swelling, bruising, altered nerve sensation and, occasionally, permanent anaesthesia, as well as involving significant costs, as with any major surgical procedure under general anaesthesia.
The introduction of Temporary Anchorage Devices (TADs) has expanded the possibilities of orthodontic treatment, beyond traditional limitations of tooth movement. Molar intrusion can be successfully carried out without the need for major surgical intervention, thus avoiding all the attendant risks and disadvantages. This paper provides an overview of anterior open bite and uses an illustrative case where open bite was successfully treated with a combination of fixed appliance therapy and TADs.
Clinical Relevance: Anterior open bite is commonly seen in general practice. A knowledge of the possible aetiological factors and their potential management should be understood by general dental practitioners. The increased popularity of TADS allows a new and less invasive approach to management of these cases.
Article
Anterior open bite (AOB) is defined as no vertical overlap of the incisors, when buccal segment teeth are in occlusion.1 This malocclusion has a multifactorial aetiology, including the inherited skeletal pattern and soft tissue influences, as well as digit-sucking habits, which can contribute enormously to an open bite (Figure 1). The incidence of anterior open bite varies with age and ethnic group. In the UK, reported incidence in children is 2–4%, reducing from age 9 years to early teens. The reduction is due to normal occlusal development and neural maturation, which means the child stops digit-sucking habits and establishes a normal swallowing pattern. Incidence has been reported as increasing in mid-teens to late vertical growth.2
Figure 1. Asymmetric anterior open bite due to persistent thumb-sucking habit.
Correcting this aspect of the malocclusion can be very challenging. Orthodontists and dentists need to be able to diagnose the problem accurately before they can formulate an appropriate treatment plan.
Aetiology
Skeletal
When the vertical component of facial growth is disproportionally greater than the horizontal component, an increase in the Frankfort-mandibular planes angle (FMPA) occurs leading to so-called ‘long face syndrome’. AOB arises as labial teeth eruption cannot compensate for the increase in interocclusal distance. The resultant open bite will usually be symmetrical and, in the most extreme situations, only posterior molars will be in occlusion (Figure 2). Patients presenting with AOB are diagnosed both clinically and cephalometrically and close attention should be paid to the relative positions of the skeletal and dental structures.
Figure 2. Severe open bite from second molars forwards.
A patient with a skeletal open bite may exhibit some, or all, of the following cephalometric features (Figure 3):
Figure 3. Skeletal features of posterior growth rotation: antegonial notching, recessive chin, reduced inter-incisal angle and increased lower facial height.
Swallowing requires an effective anterior oral seal. Children with significant lip incompetence can only achieve this by protruding their tongue to a forward position to create this seal. If the tongue is kept forward it will cover the incisors, thus reducing their eruption or, indeed, causing intrusion, leading to a reversed curve of Spee in the lower arch or an increased curve in the upper arch. In this situation, AOB correction may not be stable owing to existing soft tissue/tongue habits, which will not necessarily change, despite a change in the occlusion.
It has been shown, however, that 80% of children who have tongue thrust and AOB at 8 years show improvement without therapy, just by normal development, by age 12.2
Habits
Digit-sucking may physically impede vertical development of the incisors by the associated finger acting as a physical barrier. Persistence of this habit may cause tilting of the maxillary plane to increase the open bite further. The result of digit-sucking is often an asymmetric open bite with associated posterior crossbite. The latter occurs as a result of increased cheek pressure and lowered tongue position, inducing tooth movement and narrowing of the arch (Figure 4). The incidence of digit-sucking as a cause of AOB decreases as children get older:
Figure 4. Narrow upper arch due to increased cheek pressures and lowered tongue position.
30% – 1 year;
12% – 9 years; and
5% – 12 years.
Children who digit-suck for more than 6 hours per day can often develop a significant malocclusion.3
Cessation of the sucking may allow an open bite to close naturally, although this could take years. If habits persist after growth has finished, the open bite will often remain.
An endogeneous or primary tongue thrust is a rare condition that is difficult to distinguish from an adaptive tongue thrust. The only way of diagnosing this with absolute certainty is when the AOB re-occurs after successful treatment, allowing the provision October 2011 of an anterior oral seal. If the relapse does occur, then the tongue thrust is generally classified as endogenous rather than adaptive, which is of course a contra-indication to any further orthodontic treatment. There is nothing that can successfully remove the cause of this particular feature of the malocclusion.
Airway obstruction/mouth-breathing
Prolonged mouth-breathing due to increased tonsillar or adenoidal obstruction may be a contributory factor towards malocclusion, but it is not thought to be the main aetiological factor. Adenoidectomy or tonsillectomy should not be recommended to prevent malocclusion and should only be done for specific medical reasons.4
Indications for treatment
Aesthetic or functional aspects are the underlying reasons why patients seek treatment for their AOB. The inability to incise food efficiently or lisping and speech difficulties are common cause for complaint.5 Closure of AOB may help with eating problems, however, there is little evidence to show that treatment helps speech.6
The index of orthodontic treatment need (IOTN) has been formulated to measure the needs of patients for orthodontic treatment. Only patients with an AOB > 4 mm (IOTN 4) are felt to have a great need for treatment, on oral health grounds.
AOB: management and treatment modalities
The patients' age, their specific concerns and, of course, the aetiology of the condition will determine the appropriate treatment for the AOB. Sucking habits that persist as permanent incisors erupt should be initially gently discouraged. Simple advice about the negative effect of the habit or a daily reward incentive may break the habit. Other measures involving parents are placing a plaster on the digit or an application of nail varnish/Stop ‘n Grow (Boots.co.uk) may be sufficient to aid in discouraging the habit.
If the above methods are unsuccessful, one can resort to fitting an appliance that will remind the patient to discontinue the habit. An acrylic plate fitted with an anterior bite plane and labial bow (which allows parents to notice if it is being worn), will act as a sucking deterrent. Fixed appliances can also be used incorporating a ‘hay-rake’ that will deter the habit, as well as expanding the upper arch, if needed.
Timing for managing sucking habits
Primary dentition
‘No treatment’ is thought to be indicated. If AOB is dummy-related, then consider provision of an ‘orthodontic dummy’. Reassure parents that the AOB should resolve when the habit stops.
Early to mixed dentition
Advise parents to encourage their children to give up the habit using simple aide-memoir or a daily reward.
Late mixed dentition
If a simple advice has not worked, a deterrent appliance such as a ‘Hay-rake’ can be fitted. If orthodontic expansion of the upper arch is also needed, this can be determined by a specialist.
Permanent dentition
Spontaneous correction of AOB is unlikely. Referral to an orthodontic specialist is indicated.
Approaches to management/treatment of AOB
Early diagnosis of the aetiology of an AOB will allow interceptive treatment to be instigated with the aim of avoiding more complicated treatment later on. Certain AOB presentations can be quite mild and cause no particular problems to the patient. In such cases, the malocclusion can be accepted and treatment only undertaken to rectify crowding and to align the arches. This is especially the case if soft tissue forces are thought to be implicated as they will affect the final outcome (significant lip incompetence or endogeneous tongue thrust).
Orthodontic treatment/camouflage
If growth and soft tissue factors are favourable, an orthodontic solution to the AOB can be considered. A careful assessment of the skeletal pattern is essential, as well as considering the feasibility of tooth movement and potential for post-treatment relapse.
Extrusion of incisors to close an AOB is generally thought to be inadvisable as the relapse potential is high, after appliance removal. Treatment should therefore be aimed at molar intrusion in an attempt to control the vertical development. In milder malocclusions, use of high pull headgear to bands on molar teeth alone may be sufficient to close minor AOBs. Intrusion of buccal segment teeth can also be attempted with high pull headgear, to a removable appliance for which the palatal soft tissues have been ‘blocked out’ on the model and buccal capping covers all the buccal segment teeth. The intrusive force to the removable appliance is therefore transmitted directly to the teeth and is not resisted by the vault of the palate. This type of appliance is called a maxillary intrusion splint.
In more marked AOB, combined with a Class II skeletal discrepancy, a functional appliance such as a twin block, with the upper block designed like a ‘maxillary intrusion splint’ with the addition of high pull headgear, can be used. This will attempt restraint of maxillary growth both vertically and horizontally. Excellent patient co-operation is essential for any chance of success and favourable facial growth is also required. After the functional phase, fixed appliances are invariably used to complete arch alignment, together with necessary extractions.1
AOB can be closed using fixed appliances and vertical inter-maxillary elastics to extrude anterior teeth. This can be combined with a trans-palatal arch (TPA) and high pull headgear to limit vertical development of maxillary teeth. The TPA is used in an attempt to stop buccal flaring of first molars, which would extrude the palatal cusps, leading to further ‘propping open’ of the bite.
Vertical pull chincup therapy has been used to attempt to limit vertical jaw growth. However, chincup therapy has been shown to have poor compliance and may cause condylar damage.2
Surgery
Certain patients present with such severe AOB and other malocclusions, that they cannot be treated by orthodontics alone. Such cases require orthognathic surgery to correct the dento-facial deformities fully. Normally, such surgery will not be carried out until growth has ceased.
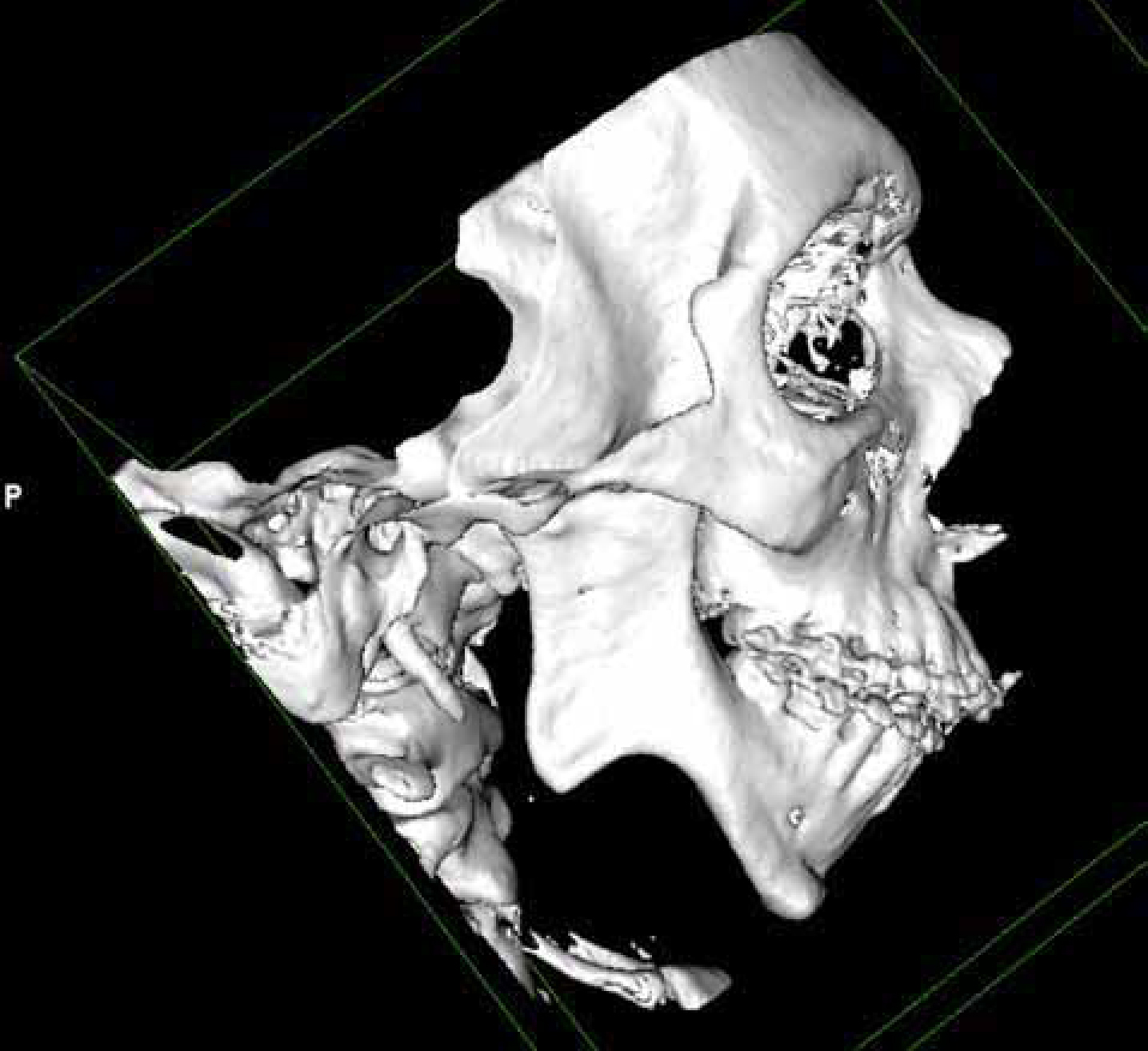
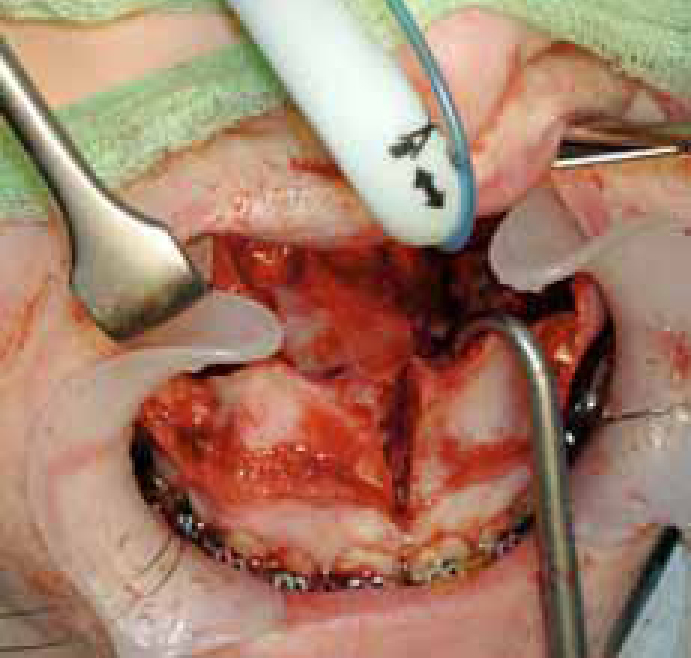
The treatment may take up to 2–3 years to complete. Extractions followed by a course of pre-surgical orthodontics, orthognathic surgery and post-surgical orthodontics is the usual sequence in the management of such patients. The orthognathic surgical procedure is mainly a Le Fort type 1 osteotomy with posterior maxillary impaction (Figure 5). An incision is made in the upper buccal sulcus to allow bone cuts to free the maxilla, which is still attached to palatal tissue providing the crucial blood supply. Posterior maxillary bone is removed, allowing the maxilla to be moved up posteriorly and the mandible to rotate, therefore closing the AOB.
Figure 5. Le Fort 1 down fracture prior to posterior maxillary impaction.
Unfortunately, surgical intervention carries risks of pain, swelling, total anaesthesia or altered sensation, nausea, vomiting, reduced movement and relapse potential, as well as the attendant risks of having a general anaesthetic. Surgical intervention may, however, allow the AOB to be fully corrected, assuming the diagnosis was correct and the orthodontics carried out to a high standard. Post-treatment stability is thought to be superior to a non-surgical option.
The advent of mini-implants or TADs has expanded orthodontic treatment possibilities beyond traditional tooth movements. Molar intrusion can be successfully carried out with the help of these implants, thus avoiding the need for major surgical intervention. Application of TADS has simplified treatment of AOB, offering an efficient and an atraumatic alternative.
TADs, in contrast to extra-oral traction, offer the advantage that patient co-operation is much less critical. There are also no undesirable reciprocal forces with the tooth movement. With absolute intrusion of posterior teeth, it is possible to allow the mandible to auto-rotate, therefore closing the open bite and reducing anterior facial height. Other advantages of TADs include:
Relative cheapness;
Easy to insert;
Relatively atraumatic and stable; and
Make it possible to apply a force immediately after insertion.
Molar intrusion with the use of TADs and elastomeric chains attached to miniscrews can apply a force of 150–200 g per tooth.
Success rates of 70 to 80% have been reported in the use of TADs.8 Titanium self-drilling, self-tapping screws with no reliance on osseo-integration are widely used, owing to their ease of placement and removal. The neck of the implant protrudes through the mucosa, allowing springs or elastics to attach and provide the appropriate force. Assessment of bone quality, local root anatomy, access and gingival health is a vital prerequisite. TADs can be placed with light local anaesthesia following a rinse with 0.2% chlorohexidine. TADs can be placed accurately with both hand and engine drivers and most of the companies recommend immediate loading. The self-tapping screws can be removed easily by simply unscrewing them without the need for anaesthesia. Complications may arise if screws become loose or break and further placement may be required in an alternative area. Root damage can occur following inaccurate placement, however, the cementum covers the traumatized area within a few weeks. Mucosal irritation occurs when the TADs are not placed within the attached gingivae. NICE guidance is for every clinician involved in placing TADs and should be involved in the national audit project run by the British Orthodontic Society (BOS). This will, hopefully, add substantially to the evidence base surrounding the use of TADs.8
Case report involving TADs
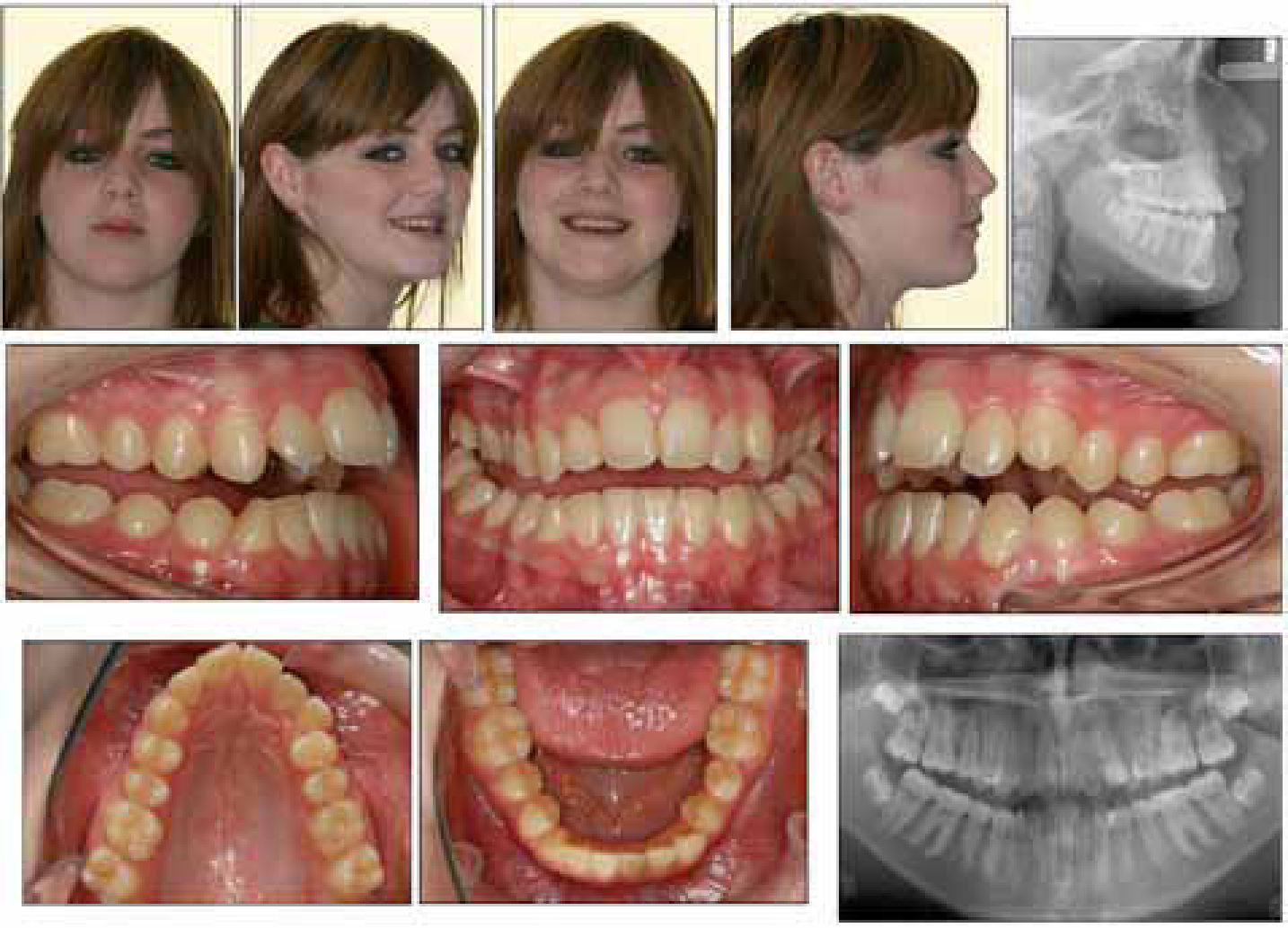
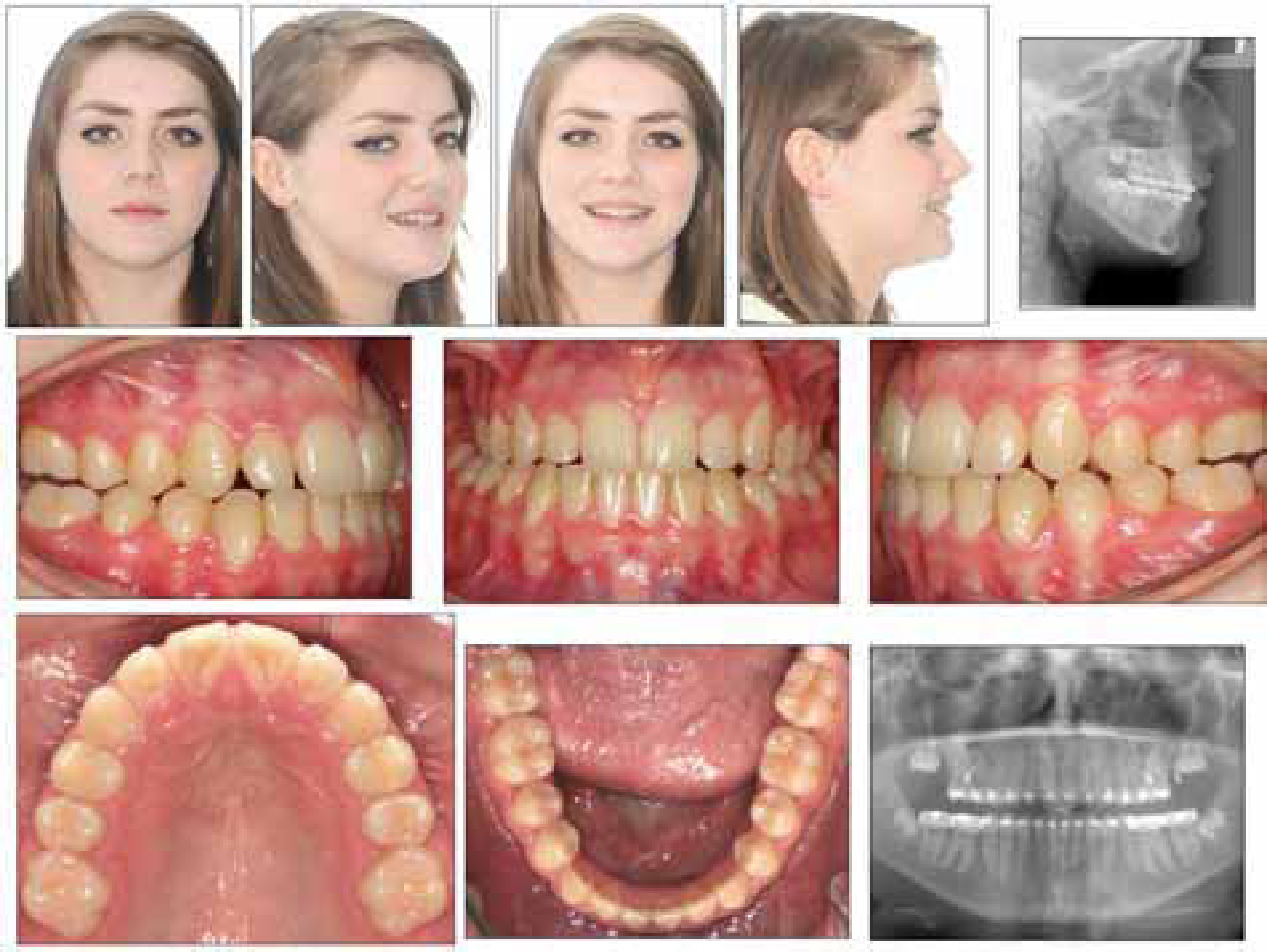
The patient presented in the permanent dentition aged 12 with a history of persistent thumb-sucking. She had a Class I skeletal pattern with an increased MMPA. She had very mild crowding in the upper and lower labial segments but with a complete open bite forward of the second molars (Figure 6).
Figure 6. Significant anterior open bite.
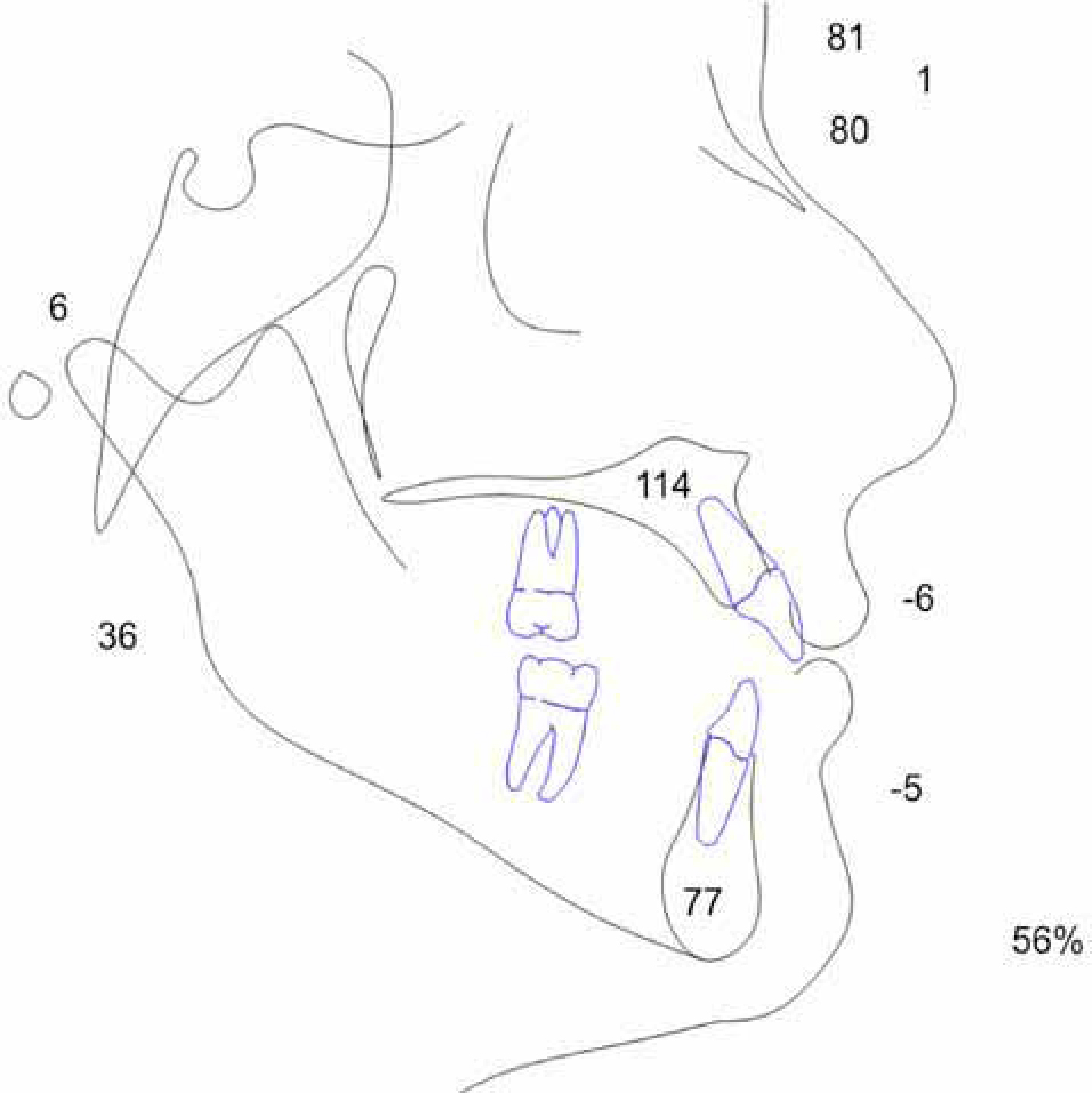
The cephalometric tracing showed a Class I base with increased MMPA of 36 degrees and increased lower facial height. The upper incisors were proclined and lower incisors retroclined (Figure 7).
Figure 7. Cephalometrics confirm a skeletal open bite.
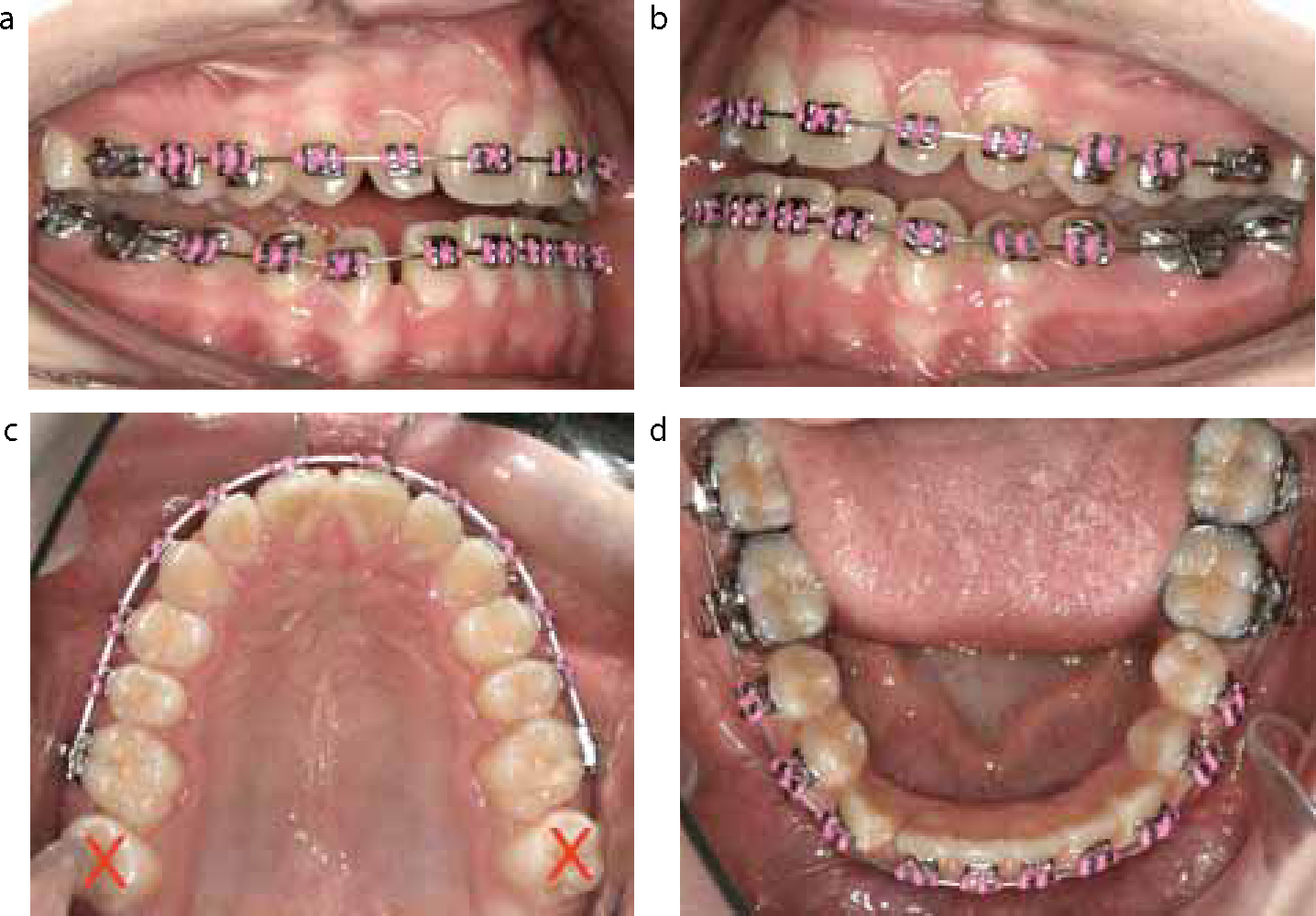
Treatment was provided with upper and lower straightwire appliances and a decision was made to extract the upper second molars (Figure 8a–d). In addition, TADs were placed buccally, to allow NiTi springs to provide an intrusive force to the posterior part of the arch. The NiTi springs had a triangular attachment on either end, which fitted perfectly over the head of the TAD. Additional TADs were also inserted palatally to allow powerchain to be stretched over the occlusal surface of the molar teeth between the buccal and the palatal TADs, to supplement the intrusive force (Figure 9a–d). The powerchain was replaced each visit and the NiTi coils can be just left in place if secure.
Figure 8.
(a–d) Decision made to extract upper second molars.Figure 9.
(a–d) TADs placed buccally and palatally to allow molar intrusion.
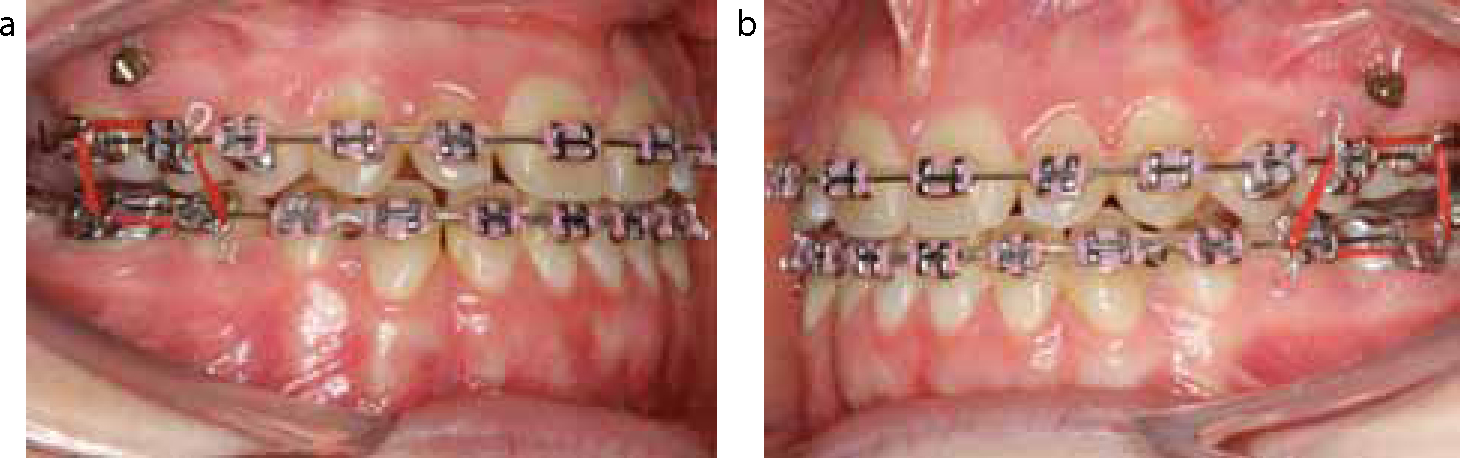
Towards the end of treatment, box elastics were used to improve the interdigitation in the buccal segments (Figure 10a, b). At the end of treatment, the patient had a normal overbite and overjet and good interdigitation of the buccal segments (Figure 11). The total treatment time was 26 months.
Figure 10. (a, b) Box elastics used in the final stages.Figure 11. A good result after 26 months of treatment.
Discussion
There are many ways to provide correction of an AOB, from gentle encouragement to desist from the deleterious habit, through removable or fixed appliances with headgear support, using recently introduced TADs or very invasive orthognathic surgery. Each method will have proponents and detractors and it is a matter of deciding which technique is most appropriate for the clinical situation that presents itself.
It could be argued that, in this particular case, removal of the upper second molars alone could have led to closure of the open bite. This will of course be true to a certain extent, as these were the only teeth in occlusion on initial presentation. In this particular case, the specific advantage offered by the use of TADs of the slight overcorrection of the posterior teeth is certainly beneficial, as anterior open bites are particularly liable to relapse. It was the combination of the choice of extraction and the intrusive effects of the mechanics that led to success. When using the TADs, it is also useful to place one TAD distally, one mesially and one palatal to the upper first molar as, should one of the TADs fail, there is still ample opportunity to provide an intrusive force to the back part of the arch on both sides. Certainly, the many case reports available in the literature indicate that the TAD technique should be at least considered as a possible alternative to more conventional approaches.
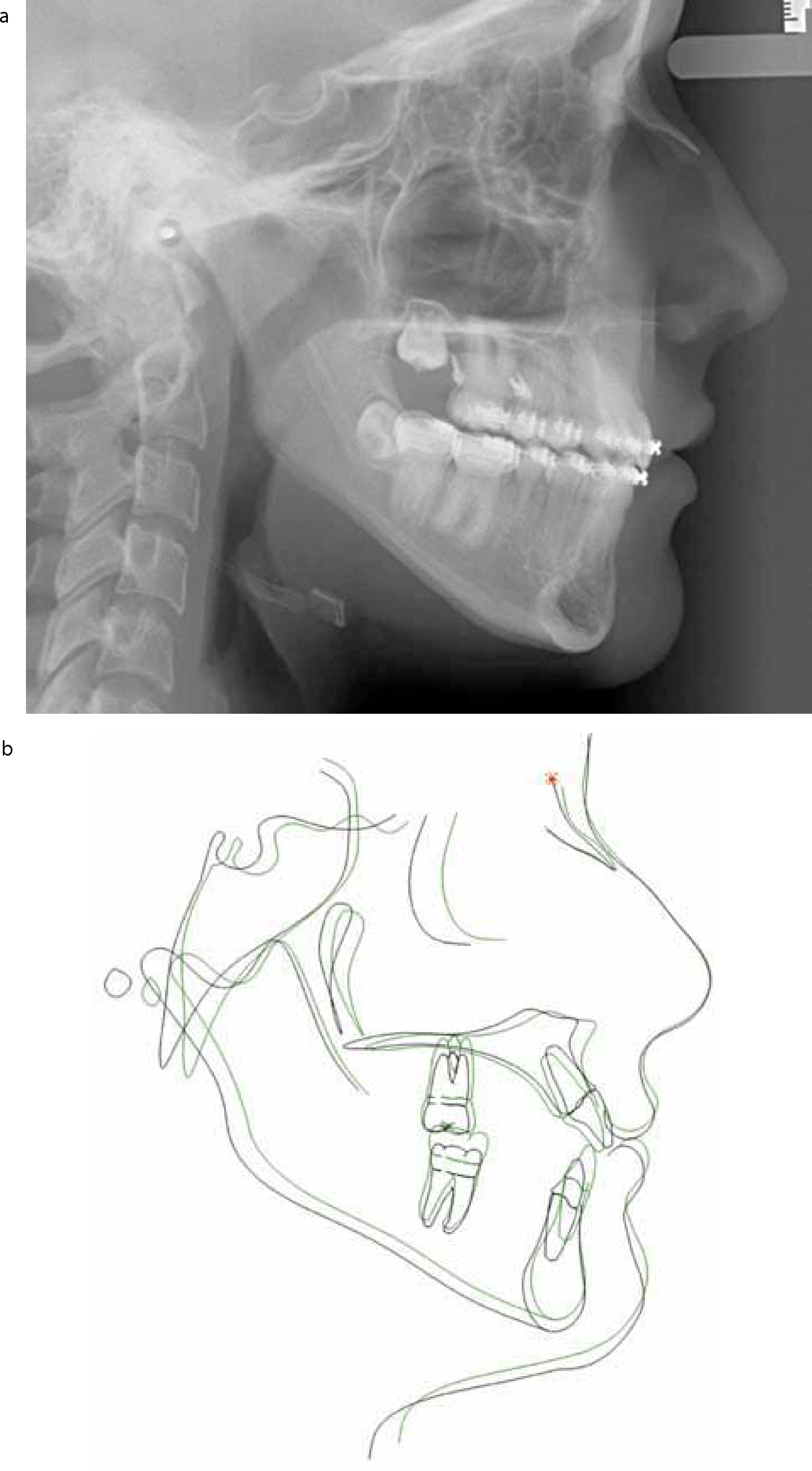
A lateral cephalometric radiograph was taken towards the end of treatment (Figure 12a) and the tracing was superimposed on the original tracing on SN at N (Figure 12b). It can clearly be seen that there was some extrusion of the upper and lower anterior teeth but, in addition, the mandible appears to have closed a small amount, which should have contributed to the success of treatment.
Figure 12.
(a) Near end of treatment cephalogram. (b) Black tracing – start of treatment, green tracing near end of treatment. Superimposition on SN @ N shows some closure of mandibular planes angle.
Retention of a corrected AOB is also a problem. Often, orthodontic treatment is completed before the rate of facial growth has slowed down and maxillary vertical growth can be one of the last aspects to cease. There are also many other factors that can contribute to the high relapse rates for AOB, including:
Soft tissue factors;
Habit resumption; or
Inappropriate orthodontic and surgical management.
Prolonged retention is advisable during an active growing period, using headgear attached to a URA with a high pull direction of force. Alternatively, a retainer with passive bite blocks, which supposedly place intrusive forces on the posterior teeth, could be used. Retainer wear should be continued until facial growth has almost ceased and this is often well into late teens. With regard to post treatment for stability of molars intruded with TADs, a 30% relapse rate has been reported and therefore overcorrection is recommended to compensate for any relapse.7
Conclusion
AOB has multiple aetiologies and accurate diagnosis is key to appropriate treatment planning. Many open bites resolve before 12 years of age as a result of digit-sucking habits ceasing and maturation of swallowing pattern. There is always a risk of relapse, even following successful treatment, and this information must be given to the patients to ensure informed consent is obtained.
There are many reported cases and studies of successfully treated open bite using different treatment modalities. There has to date been no evidence-based evaluation of the best treatment options. However, with the introduction of TADs as an effective treatment modality, lengthy, traumatic and expensive surgery may be avoidable in carefully selected cases.