Glick M, Williams DM, Kleinman DV A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. Br Dent J. 2016; 221:792-793 https://doi.org/10.1038/sj.bdj.2016.953
Grainger RM. Orthodontic treatment priority index. Vital Health Stat 2. 1967; (25)1-49
Hassan R, Rahimah A. Occlusion, malocclusion and method of measurements-an overview. Arch Orofac Sci. 2007; 2:3-9
Marya C. A Textbook of Public Health Dentistry.New Delhi, India: JP Medical Ltd; 2011
Angle EH. Classification of malocclusion. Dental Cosmos. 1899; 41:248-357
Gravely JF, Johnson DB. Angle's classification of malocclusion: an assessment of reliability. Br J Orthod. 1974; 1:79-86 https://doi.org/10.1179/bjo.1.3.79
British Standard Glossary of Dental Terms BS4492.London: BSI; 1983
Ballar D CF, Wayman JB. A report on a survey of the orthodontic requirements of 310 army apprentices. Dent Pract Dent Rec. 1965; 15:221-226
Williams AC, Stephens CD. A modification to the incisor classification of malocclusion. Br J Orthod. 1992; 19:127-130 https://doi.org/10.1179/bjo.19.2.127
Du SQ, Rinchuse DJ, Zullo TG, Rinchuse DJ. Reliability of three methods of occlusion classification. Am J Orthod Dentofacial Orthop. 1998; 113:463-70 https://doi.org/10.1016/s0889-5406(98)80019-x
Brin I, Weinberger T, Ben-Chorin E. Classification of occlusion reconsidered. Eur J Orthod. 2000; 22:169-174 https://doi.org/10.1093/ejo/22.2.169
Jones CM, Woods K, O'Brien K Index of Orthodontic Treatment Need, its use in a dental epidemiology survey calibration exercise. Community Dent Health. 1996; 13:208-210
Burden DJ, Pine CM, Burnside G. Modified IOTN: an orthodontic treatment need index for use in oral health surveys. Community Dent Oral Epidemiol. 2001; 29:220-225 https://doi.org/10.1034/j.1600-0528.2001.290308.x
Evans R, Shaw W. Preliminary evaluation of an illustrated scale for rating dental attractiveness. Eur J Orthod. 1987; 9:314-318 https://doi.org/10.1093/ejo/9.4.314
Linder-Aronson S. Orthodontics in the Swedish Public Dental Health Service. Trans Eur Orthod Soc. 1974; 233-240
Camilleri S, Mulligan K. The prevalence of malocclusion in Maltese schoolchildren as measured by the Index of Orthodontic Treatment Need. Malta Med J. 2007; 19:9-24
Cooper S, Mandall NA, DiBiase D, Shaw WC. The reliability of the Index of Orthodontic Treatment Need over time. J Orthod. 2000; 27:47-53 https://doi.org/10.1093/ortho/27.1.47
Beglin FM, Firestone AR, Vig KW A comparison of the reliability and validity of 3 occlusal indexes of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2001; 120:240-246 https://doi.org/10.1067/mod.2001.116401
Bollen AM, Cunha-Cruz J, Bakko DW The effects of orthodontic therapy on periodontal health: a systematic review of controlled evidence. J Am Dent Assoc. 2008; 139:413-422 https://doi.org/10.14219/jada.archive.2008.0184
Singh P. Adult orthodontic patients in primary care and their motivation for seeking treatment. Orthod Update. 2016; 9:69-72
Williams AC, Shah H, Sandy JR, Travess HC. Patients' motivations for treatment and their experiences of orthodontic preparation for orthognathic surgery. J Orthod. 2005; 32:191-202 https://doi.org/10.1179/146531205225021096
Cons NC, Kohout FJ, Jenny J. DAI – the dental aesthetic index.: College of Dentistry, University of Iowa; 1986
Richmond S, Daniels CP. International comparisons of professional assessments in orthodontics: Part 1 – Treatment need. Am J Orthod Dentofacial Orthop. 1998; 113:180-185 https://doi.org/10.1016/s0889-5406(98)70290-2
Richmond S, Shaw WC, Roberts CT, Andrews M. The PAR Index (Peer Assessment Rating): methods to determine outcome of orthodontic treatment in terms of improvement and standards. Eur J Orthod. 1992; 14:180-187 https://doi.org/10.1093/ejo/14.3.180
Ramanathan C. Evaluation of the stability after orthodontic treatment using PAR index. Acta Medica (Hradec Kralove). 2006; 49:209-213 https://doi.org/10.14712/18059694.2017.134
Hamdan AM, Rock WP. An appraisal of the Peer Assessment Rating (PAR) Index and a suggested new weighting system. Eur J Orthod. 1999; 21:181-192 https://doi.org/10.1093/ejo/21.2.181
An orthodontic index is a rating or categorizing system that assigns a numeric score or alphanumeric label to a person's occlusion. Indexing of malocclusions and their correction is important in epidemiology, diagnosis, communication between clinicians as well as with their patients, and assessing treatment outcome. Many useful indices have been put forward, but no one method appears to be equally suitable for the use of epidemiologists, public health programme planners and clinicians. This article describes the common clinical orthodontic indices and classifications used in the UK.
CPD/Clinical Relevance: Readers can gain an insight into the advantages and disadvantages of the commonly used orthodontic indices and classifications in the UK.
Article
The delivery and acceptability of orthodontic treatment is increasing as it becomes more popular. To aid this, indexing of the malocclusion, and its subsequent correction, is important in epidemiology, assessment and diagnosis, and communication between clinicians as well as their patients. This article looks at the common clinical orthodontic indices and classifications used in UK.
Definition
Orthodontic indices are used to describe a rating or classification system that assigns a (alpha)numeric label to a person's (mal)occlusion.1
Salzmann2 thought of malocclusion as occlusal traits that interfered with the wellbeing of the patient: adversely affecting their function or dentofacial aesthetics. This still resonates within the World Dental Federation's definition of oral health,3 which reflects the physiological, social and psychological attributes that are essential to one's oral health-related quality of life.
Need for indices
The first qualitative indices were used in the 1950s for epidemiological purposes. These methods were subjective and broad, but gave a generally easy description and understanding of the malocclusion. From 1950s onwards, further qualitative indices were developed to rank or score the severity of the malocclusion to help prioritize and determine access to care.
Many useful and interesting indices have been put forward, but no one method appears to be equally suitable for the needs of epidemiologists, public health programme planners and clinicians.4,5 An ideal index has a number of requirements (Tables 1 and 2).6
Epidemiological
Determine the prevalence and incidence of occlusal anomalies
Economic health care resource planning (financially and in terms of manpower)
For academic research
Clinical assessment
Prioritization of orthodontic treatment provision within healthcare systems
Prevalence of malocclusion in the local population
Local demand for treatment
Services may be subsidised by the government/provided by insurance companies
Inter-disciplinary communication
Patient referral
Informed consent
Severity of malocclusion
Difficulty of treating the malocclusion
Monitoring/promoting standards
1.
Reliable (Reproducible)
The index should be able to measure consistently at different times
Reliability of an occlusal index means that the same results are yielded by repeated measurements from the same examiner or different examiners
2.
Valid
The index should measure what it was intended to measure
Validity of an index requires that it accurately measures what it intends to measure, not only at that point in time, but throughout dental development.3
The validity of an index of orthodontic need is established by comparing the results of applying the rules of that index with the opinion of orthodontic specialists to assess the severity of treatment need
3.
Sensitive
The index should be able to detect small changes
4.
Acceptable
The index should be acceptable to the profession and the public
5.
Objective
The index should require minimal judgement
6.
Quick and simple
The index should be easy to remember and apply
7.
Quantifiable
Statistical analyses can be carried out on the results from index use
8.
Low cost
Types of indices
Indices can be classified into five groups based upon their purpose.1
Diagnostic;
Epidemiological;
Treatment need;
Treatment outcome; and
Treatment complexity.
Table 3 shows the most commonly used indices in the UK.
Diagnostic (classification)
Treatment need
Treatment outcome/success
Angle's classification
Index of Treatment Need (IOTN)
Peer assessment rating (PAR)
Incisor classification
Index of Orthodontic Functional Need (IOFTN)
Diagnostic classifications
Angle's classification 1899
Angle's system7 is one of the oldest and most well-known indices employed by the majority of clinicians worldwide. This is because it is simple to use, easy to understand and quick to undertake. It was initially devised as a prescription for treatment rather than for diagnostic purposes by clearly conveying the nature of the malpositioned teeth that required correction.
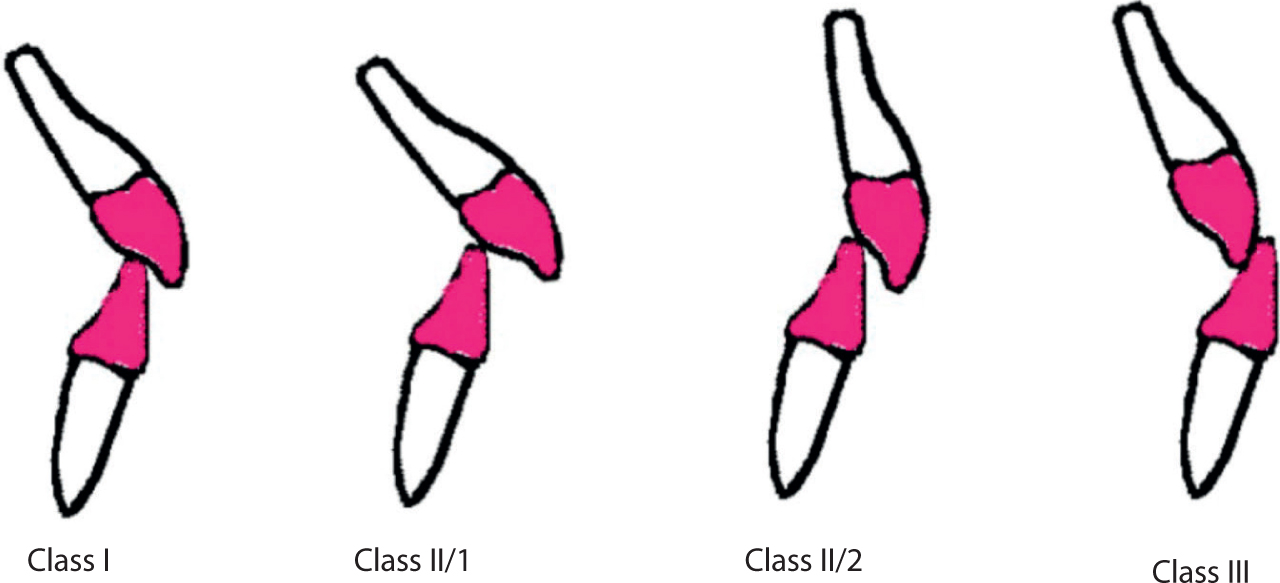
The classification, as we use it today, describes the relationship of the lower first permanent molars relative to the upper first permanent molars in the antero-posterior plane (Table 4 and Figure 1).7 Angle had also stressed the importance of looking at the positions of the other teeth and facial lines as part of his planning,7 but this is much less commonly used (Table 5).
Class I (neutrocclusion)
Mesiobuccal cusps of U6 occlude with buccal groove of L6
Class II (distocclusion/post-normal)
Mesiobuccal cusp of U6 at least one cusp width mesial to Class I
Division 1
Mandible retruded and maxillary incisors protruded
Division 2
Mandible retruded and maxillary incisors retruded
Class II subdivision
Class I on one side, Class II on the other side
Class Ill (mesiocclusion/pre-normal)
Mesiobuccal cusp of U6 is at least one cusp width distal to Class I
Class III subdivision
Class I on one side, Class III on the other side
Figure 1. Diagrammatic presentation of Angle's molar classification.
Class I
Neutrocclusion
Relative position of the dental arches, mesio-distally, normal, with malocclusions usually confined to the anterior teeth
Class II
Distocclusion/post-normal
Retrusion of the lower jaw, with distal occlusion of the lower teeth
Division 1
(a) Narrow upper arch, with lengthened and prominent upper incisors; lack of nasal and lip function. Mouth breathers
(b) Same as (a), but with only one lateral half of the arch involved, the other being normal. Mouth breathers
Division 2
(a) Slight narrowing of the upper arch; bunching of the upper incisors, with overlapping and lingual inclination; normal lip and nasal function
(b) Same as (a), but with only one lateral half of the arch involved, the other being normal; normal lip and mouth function
Class Ill
Mesiocclusion/pre-normal)
(a) Protrusion of the lower jaw, with mesial occlusion of the lower teeth; lower incisors and cuspids inclined lingually
(b) Same as (a), but with only one lateral half of the arch involved, the other being normal
Critics have argued that the Angle's molar classification system is too simple and potentially inaccurate when describing malocclusions. The classification confines malocclusions to discrete variables, when they are in fact not: leading to variable reliability between different operators, especially in Class II division 2 malocclusions.8 Modifications have been suggested to improve reliability by introducing numerical quantification (½ unit, or millimetres) and by even changing the tooth to a premolar instead of the first permanent molar.9 These modifications have been proven to be more reliable, but have not been widely accepted.
Angle had thought that the key to occlusion was that the upper permanent first molars (and canines) always erupted in a stable (fixed) position and controlled the position of the other teeth. However, it is now known that this is not the case owing to factors, such as early loss of second deciduous molars, congenitally missing premolars (hypodontia), and other local factors.
British Standards Institute classification of malocclusion (BS4492 1982)
The British Standards Institute's (BSI) classification10 is based upon Ballard and Wayman's work. They analysed the orthodontic requirements of 310 army apprentices,11 and this has now superseded Angle's classification in the UK for describing a malocclusion. In this, four categories describe the manner in which the lower incisor edges occlude with the upper incisor cingulum plateau, rendering an occlusion Class I, Class II division I, Class II division 2 and Class III (Table 6 and Figure 2).10
Class I
The lower incisor edges preclude with or lie immediately below the cingulum plateau (middle part of the palatal surface) of the upper central incisors.
Class II
The lower edges lie posterior to the cingulum plateau of the upper incisors.
Division 1
There is an increase in overjet and the upper central incisors have average inclination or are proclined.
Division 2
There is an increase in overjet (usually minimal) and the upper central incisors are retroclined.
Class IlI
The lower incisor edges lie anterior to the cingulum plateau of the upper incisors. The overjet is reduced or reversed.
Figure 2. Diagrammatic presentation of British Standards Institute incisor classification.
As with Angle's classification, Williams and Stephens12 found inter-operator disagreement, and therefore unreliability, using the BSI classification. This was particularly notable in Class II incisal relationships. They recommended that the classification be extended to include a Class II intermediate group, where ‘the lower incisor edges lie posterior to the cingulum plateau of the upper central incisors. The upper incisors are upright or slightly retroclined and the overjet lies between 5 and 7 mm’.
Attempts to increase the reproducibility of a diagnostic index have been made, for example, Du et al13 and Brin et al14 found that Katz's classification was the most reproducible above the BSI and Angle's classifications, respectively. In Katz Class I, The most anterior upper premolar fits exactly into the embrasure created by the distal contact of the most anterior lower premolar.9 However, since this index still deals with only one aspect of malocclusion, with sole focus on the buccal segment, there is still a degree of unreliability.
The Index of Orthodontic Treatment Need (IOTN)15 is one of the most widely used indices around the world to rank malocclusions. It has been routinely used in the National Health Service (NHS) since 2006. The index was developed to determine the eligibility for orthodontic treatment and therefore prioritize care and referrals for those with the highest ‘need’. The index is quick and easy to use as a single worst feature is chosen; it can be used chairside or on dental casts; used in inter-disciplinary communication; the index can be modified for use in epidemiological studies16,17 and quantitative data can be yielded for analysis.
There are two components to the index: the dental health component (DHC) and the aesthetic component (AC). The AC was initially developed by Evans and Shaw in 198718 and was based on lay peoples' judgement of 1000 photos of 12 year old occlusions on a scale of 1 (most attractive teeth) to 10 (least attractive teeth). The photo that was the closest match to the patient's occlusion receives that score. A score of 6 or above implies a need for orthodontic treatment.
The DHC is based upon Linder-Aronson's work for the Swedish Public Dental Health Service from 1974.19 The malocclusion is grouped into five categories where 1 indicates no ‘need’ for orthodontic treatment and 5 indicates a ‘very great’ need for treatment.20 A specific ruler can be used to help assess the DHC score. The categories are further subdivided using letters that describe the feature of the malocclusion that has been scored in a given order of importance: ‘MOCDO’ (missing teeth, overjet, crossbite, displacement of contact points and overbite; Table 7).
4h: less extensive hypodontia requiring orthodontic treatment for pre-restorative or space closure
Overjet
5a: OJ >9mm5m: ROJ >3.5 mm + masticatory and speech difficulties
4a: OJ 6.1–9 mm4b: ROJ >3.5 mm with no masticatory and speech difficulties
3a: OJ 3.6–6 mm; incompetent lips3b: ROJ 1.1–3.5 mm
2a: OJ 3.6–6 mm; competent lips2b: ROJ 0.1–1 mm
Crossbite
4c: x-bites + >2 mm discrepancy between RCP and ICP4l: posterior lingual x-bite
3c: x-bite; 1.1–2 mm discrepancy between RCP and ICP
2c: x-bite with up to 1 mm discrepancy between ICP and RCP
Displacement of contact point
4d: contact point displacement > 4mm4t: partially erupted teeth, tipped and impacted against adjacent teeth4x: supplemental teeth
3d: contact point displacement 2.1–4 mm
2d: contact point displacement 1.1–2 mm
Minor irregularity
Overbite (including open bite)
4e: lateral or anterior open bite > 4 mm4f: increased + complete OB + gingival or palatal trauma
3e: lateral or anterior open bite 2.1–4 mm3f: increased + complete OB with no gingival trauma
2e: lateral or anterior open bite 1.1–2 mm2f: increased OB >3.5 mm and no gingival contact
Studies have found that both the DHC and AC have high reproducibility, with the former having an inter-clinician kappa score of above 0.80 and the latter of above 0.72.21,22
Despite the reliability of the IOTN, the index has its own drawbacks and obviates features of malocclusion, such as spacing. The DHC component of the IOTN also reflects some of our previous understanding regarding the health risks of a malocclusion, which are now only weakly correlated at best for most of the features of malocclusion: hypodontia can score a 4 or 5 on the DHC, with no evidence to suggest that this is associated with an oral health problem requiring orthodontics, and similarly little evidence exists connecting crowding to periodontal health issues.23
The desire for orthodontic treatment is primarily driven by the perception of the patient regarding their own dental or facial aesthetics.24,25 In the IOTN, the AC allows for this, but only through the frontal view of the occlusion in predominantly Class I/II malocclusions. Thus, it also has limitations through using mostly one incisal class, and not including a full smile or facial views. Additionally, there is ambivalent evidence regarding the psychological impact that the malocclusion and smile of a patient can have on self-esteem. For example, a patient with a moderate treatment need may be more psychologically impacted by their malocclusion than someone with a higher treatment need. This disadvantage has the risk of insensitivity and misjudgement of the needs of the individual patient. These additional nuances can be found in the Dental Aesthetic Index (DAI)26 and are described in Jenny and Cons,27 but this does makes the index more complicated and time consuming.
Some patients also have functional problems owing to their malocclusion, and this is especially true in orthognathic patients. Unfortunately, the IOTN does not completely take into account such issues, and so another index was developed to overcome this, the Index of Orthognathic Functional Treatment Need (IOFTN).28
Questions have arisen over the validity of the IOTN and whether it really does measure the ‘need’ for orthodontic treatment, as ‘need’ depends on many factors that may be subjective and varied between countries owing to the system of remuneration, or social norms.29,30 The IOTN, perhaps, needs re-evaluation to consider more recent findings related to malocclusion and oral/psychosocial wellbeing and to also take the patient's desire for treatment into account. After all, oral health is defined as being ‘multi-faceted and includes the ability to speak, smile, smell, taste, touch, chew, swallow and convey a range of emotions through facial expressions with confidence and without pain, discomfort and disease of the craniofacial complex’.3
Treatment success
Peer Assessment Rating (PAR)
The Peer Assessment Rating (PAR) was formulated over a series of meetings by 10 orthodontists before its publication.31 The PAR index is a quantitative and objective method for measuring malocclusion. In it, a weighted score is assigned to each of the occlusal traits that make up the malocclusion. The weighting of the scores is based on the severity of the trait and the perceived difficulty in correcting it. The sum of the scores then represents the degree to which the malocclusion deviates from the norm. A specific ruler showing the seven occlusal traits that PAR assesses is used, which makes scoring quick and easy to perform.
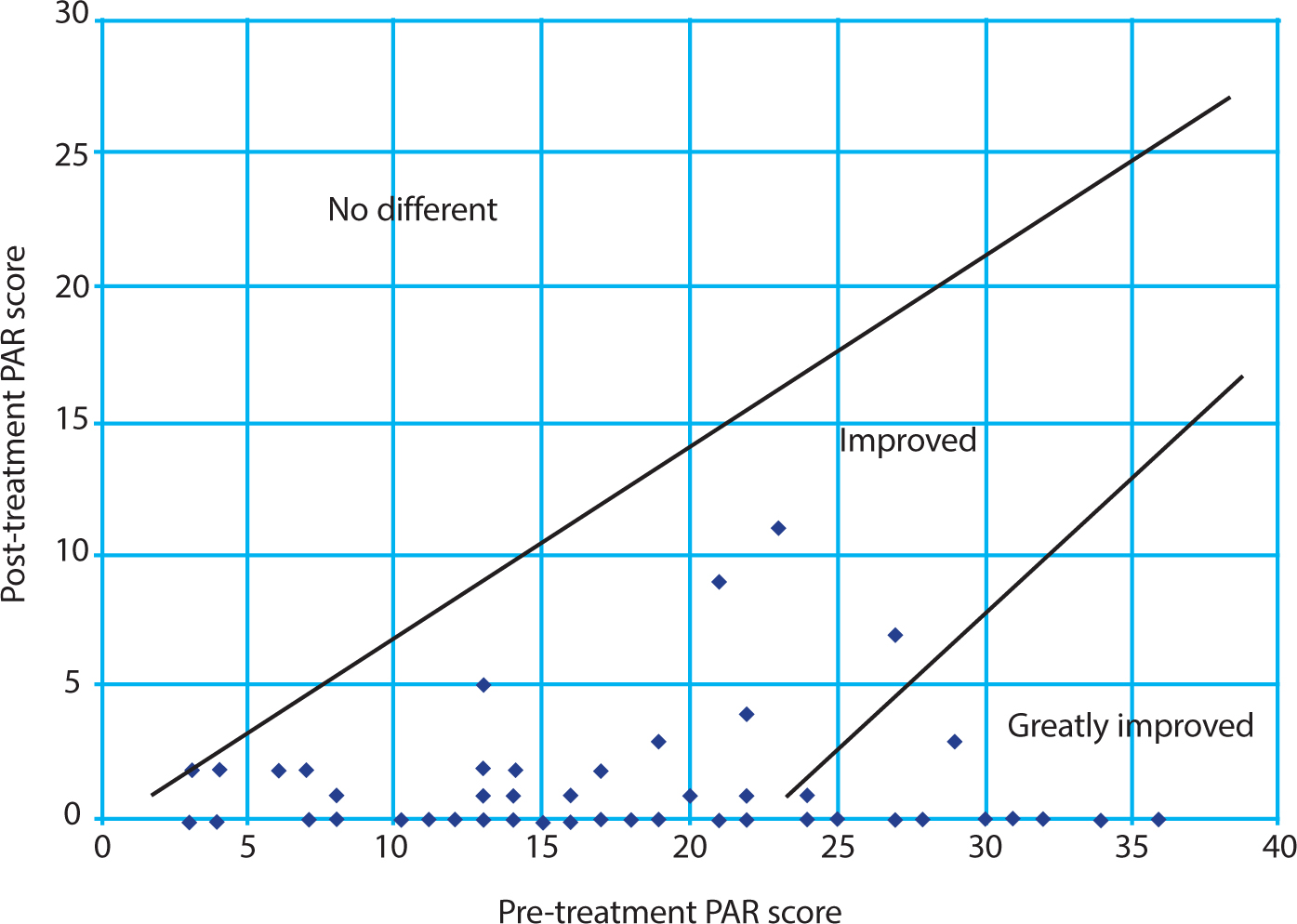
PAR scores are any easy tool that can be used to measure the efficacy of the clinical treatment. The difference between the post- and pre-treatment scores indicates the improvement (or not) as a result of orthodontic treatment. These PAR scores may be plotted on a graph to show the percentage of patients who are ‘worse or no different,’ ‘improved,’ or ‘greatly improved’ at the end of orthodontic treatment (Figure 3).
Figure 3. PAR graph.32
Of note, there are slight differences between the PAR developed in the UK and its modified version used in the USA. Hamdan and Rock33 criticized the index, stating that the PAR weighting appears generic and unrepresentative. The high weighting for overjet, for example, may disproportionately increase the PAR score, while the low weighting for overbite could mean that correcting functional issues, such as a traumatic overbite, is misrepresented in terms of treatment value.34 Much like the IOTN, this index does not consider treatment ‘need’ in its broadest terms: taking the patient's social/cultural background into account as well as the patient's own perceived need for treatment.
Conclusion
The purpose of diagnostic indices is to provide a descriptive method of classifying malocclusions so that clinicians can communicate with each other and an idea for the prescription of treatment can be envisaged. Each index or classification has its own advantages and disadvantages, furthermore it is not easy to achieve all the ideal characteristics. Additionally, with progress in different fields of orthodontics, our understanding of diagnosis and treatment planning has changed somewhat since the above indices and classifications were presented. In this age of evidence-based dentistry, are we really following what the evidence suggests? Do we need to change our diagnostic taxonomy, or does what we use have sufficient validity?