Moyers RE., 4th edn. Chicago: Yearbook Medical Publishers Inc; 1988
Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthoped. 1992; 101:159-171
Johnston WD. Treatment of palatally impacted canine teeth. Am J Orthod. 1969; 56:(6)589-596
Dewel BF. The upper cuspid: its development and impaction. Angle Orthod. 1949; 19:79-90
McSherry PF. The ectopic maxillary canine: a review. Br J Orthod. 1998; 25:209-216
Hägg U, Taranger J. Timing of tooth emergence. A prospective longitudinal study of Swedish urban children from birth to 18 years. Swed Dent J. 1986; 10:(5)195-206
Ericson S, Kurol J. Longitudinal study and analysis of clinical supervision of maxillary canine eruption. Community Dent Oral Epidemiol. 1986; 14:172-176
The management of the palatally ectopic maxillary canine. The Royal College of Surgeons of England, Faculty of Dental Surgery Clinical Guidelines. 2004. www.rcseng.ac.uk
Becker A, Smith P, Behar R. The incidence of anomalous lateral incisors in relation to palatally displaced cuspids. Angle Orthod. 1981; 51:24-29
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:(4)249-256
Jacoby H. The etiology of maxillary canine impaction. Am J Orthod. 1983; 84:125-132
Becker A, Chaushu S. Dental age in maxillary canine ectopia. Am J Orthod Dentofacial Orthop. 2000; 117:(6)657-662
Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987; 91:483-492
Ericson S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod. 2000; 70:415-423
Ericson S, Kurol J. Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. Am J Orthod Dentofacial Orthop. 1988; 94:503-513
Becker A, Chaushu S. Success rate and duration of orthodontic treatment for adult patients with palatally impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2003; 124:(5)509-514
Ericson S, Kurol J. Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur J Orthod. 1986; 8:(3)133-140
Jacobs SG. Radiographic localization of unerupted maxillary anterior teeth using the vertical tube shift technique: the history and application of the method with some case reports. Am J Orthod Dentofacial Orthop. 1999; 116:(4)415-423
Preda L, La Fianza A, Di Maggio EM, Dore R, Schifino MR, Campani R, Segù C, Sfondrini MF. The use of spiral computed tomography in the localization of impacted maxillary canines. Dentomaxillofac Radiol. 1997; 26:(4)236-241
Becker A, Shpack N, Shteyer A. Attachment bonding to impacted teeth at the time of surgical exposure. Eur J Orthod. 1996; 18:457-463
Pearson MH, Robinson SN, Reed R, Birnie DJ, Zaki GA. Management of palatally impacted canines: the findings of a collaborative study. Eur J Orthod. 1997; 19:511-515
Van Noort R., 3rd edn. Oxford: Mosby Elsevier; 2007
Parkin N, Benson PE, Thind B, Shah A. Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth. Cochrane Database of Systematic Reviews. 2008; (4) https://doi.org/10.1002/14651858.CD006966.pub2
McDonald F, Yap WL. The surgical exposure and application of direct traction of unerupted teeth. Am J Orthod. 1982; 89:331-340
Ectopic eruption with impaction of maxillary permanent canine teeth is a frequently encountered clinical problem. Surgical exposure and attachment of a gold chain to impacted maxillary canines is often required in order to bring them into the dental arch and to allow good alignment. The principle of radiographic parallax is employed to determine whether the impacted canine is placed buccal or palatal to adjacent teeth. Good flap design allows adequate access to the impacted tooth. Bone removal should be adequate to free the impacted crown to its greatest circumference. An orthodontic eyelet with a gold chain is then bonded to the crown of the impacted tooth. Use of a good bonding technique will minimize chances of bond failure necessitating a second surgical procedure. Atraumatic surgical procedure will allow minimal postoperative complications and a rapid recovery.
Clinical Relevance: This article describes a surgical technique to expose impacted maxillary canines and attach gold chains, to facilitate orthodontic alignment into the dental arch. The principle of radiographic parallax to determine the bucco-palatal position of impacted canines is also discussed.
Article
Ectopic eruption and impaction of maxillary permanent canine teeth is a frequently encountered clinical problem. The maxillary canine is second only to the lower third molar in frequency of impaction.1 The prevalence of impaction or ectopic eruption of the permanent maxillary canine has been reported to range from 0.92% to 2.2%, of which 8% are bilateral impactions. Maxillary canine impactions are twice as common in females (1.17%) as in males (0.51%).2 About one-third of impacted maxillary canines are positioned labially or within the alveolus, and two-thirds are located palatally. A palatally impacted maxillary canine is the most common impaction encountered by orthodontists.3
Development of upper and lower canines commences between 4 and 5 months of age. Maxillary canines have the longest period of development, as well as the longest and most tortuous path of eruption.4 These are the last teeth with a deciduous predecessor in the upper arch to erupt and therefore the most susceptible to environmental influences, such as crowding.5 On average, the maxillary canines erupt at 11–12 years of age and mandibular canines erupt at 9–10 years of age.6
The majority of normally erupting maxillary canines should be palpable in buccal sulcus by the age of 10–11 years.7 On clinical examination, if maxillary canines are not palpable in the buccal sulcus by the age of 10–11 years, or if an asymmetrical eruption pattern is noticed on palpation, canine ectopia should be suspected. Maxillary canines erupting after 12 years of age in girls and 13 years in boys may be considered late and these patients should be referred for specialist advice.8
Aetiology of impacted maxillary canines
The aetiology of palatally displaced maxillary canines has been suggested as polygenic and mutifactorial. Becker et al9 suggested that the distal aspect of the lateral incisor root guides the permanent canine to erupt into its correct position, hence leading to the ‘Eruption Guidance’ theory.
Because of the very high and palatal initial position, plus the extremely long path of eruption, local factors may interfere with the normal path of eruption, such as:
Congenitally missing lateral incisors;
Peg-shaped or diminutive lateral incisors;
Supernumerary teeth;
Tooth transpositions; or
Any other mechanical determinants that can all lead to canine ectopia.
A 2½-fold increase in the incidence of palatally displaced canine adjacent to the sites of missing lateral incisors or short-rooted lateral incisors has been reported.9
A multifactorial polygenic aetiology for a palatally displaced canine has also been suggested by Peck et al,10 on the basis of five individual categories:
Occurrence of other dental anomalies with palatally displaced canines, eg hypodontia and microdontia;
Bilateral occurrence of palatally displaced canines;
Sex difference in the occurrence of palatally displaced canines;
Familial occurrence of palatally displaced canines;
Population differences in the occurrence of palatally displaced canines.
Jacoby11 in his study found that 83% of buccally displaced canines were associated with crowding, whereas 85% of palatally impacted canines had sufficient space for eruption in the dental arch. Various other aetiological factors for impaction of maxillary canines have been suggested, such as displacement of the crypt, long path of eruption, impeded eruption due to a supernumerary tooth or an odontome and retained deciduous canine. An association between a palatally displaced canine and a late-developing dentition has also been found by Becker and Chaushu.12
Sequelae of canine ectopia
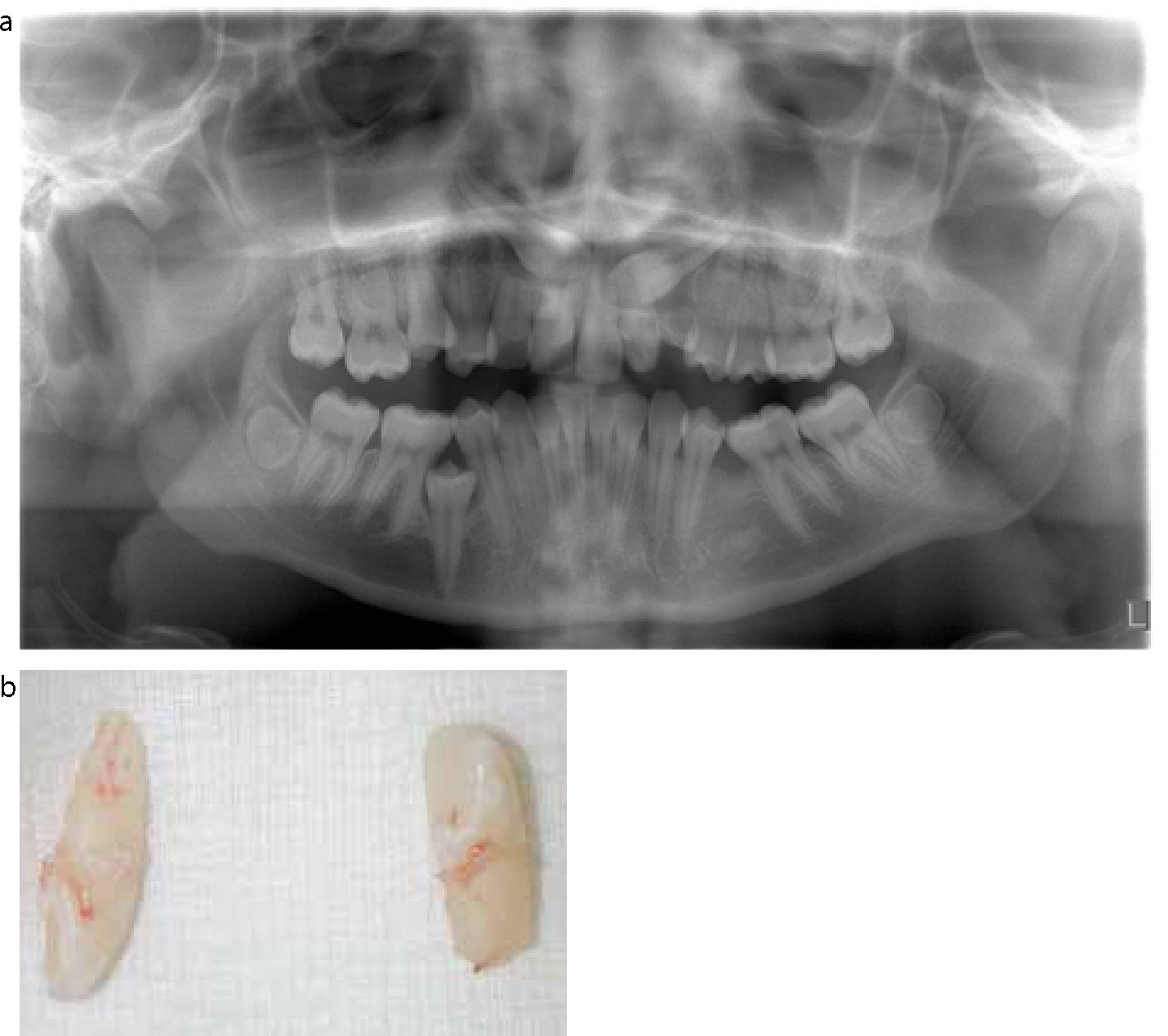
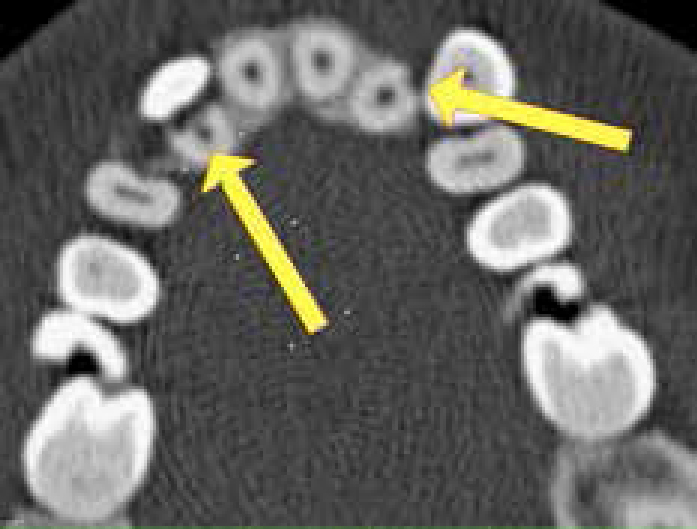
Maxillary canine impaction has been associated with many aesthetic, functional and orthodontic problems. The main risk appears to be root resorption of adjacent permanent incisors (Figure 1). Ericson and Kurol,13 from their study using intra-oral and panoramic radiographs, have reported that as many as 0.7% of children aged 10–13 years, with ectopic permanent maxillary canines, are likely to demonstrate evidence of root resorption of adjacent permanent incisors. However, in a CT study by the same authors, root resorption has been detected in up to 48% of incisors adjacent to ectopic maxillary canines14 (Figure 2). It has been suggested that root resorption of incisors by palatally ectopic canines rarely starts after 14 years of age15 and it occurs most frequently between 11 and 12 years.16
Figure 1.
(a, b) Root resorption of lateral incisors caused by bilateral ectopic canines.Figure 2. CT scan showing resorbed root of lateral incisor due to the ectopic canine.
Ankylosis of ectopic maxillary canines is also an associated risk and is shown to be more common in older subjects more than 30 years of age,17 although true ankylosis of ectopic canine is still a rare occurrence. Other potential problems associated with impacted canines include:
Space loss due to migration of neighbouring teeth;
Limited deciduous canine prognosis with eventual tooth loss;
Complexity of definitive orthodontics;
Ultimate restorative challenges;
Interference with alignment of other teeth; and, finally
Possible cyst formation.
Localization of an impacted canine
A clinical and radiographic examination is required to investigate the presence and position of the impacted canine and any associated pathology. If the maxillary canine is non-palpable in buccal sulcus by the age of 10–11 years, or if palpation indicates an asymmetrical eruption pattern, the possibility of canine ectopia should be suspected and a comprehensive assessment of malocclusion and location of impacted canine should be carried out.8 Absence of a canine bulge is not always indicative of impaction. Radiographic examination to determine the eruption path of a maxillary canine prior to the age of 10 years is of little major benefit.18 A palatal bulge in the upper canine region is a strong indication of a palatally displaced canine.
After 11–12 years of age, the retained deciduous canines should always be examined for mobility. If firm, this indicates either delayed dental development or failure of root resorption by the permanent canines. Mobility, migration, discoloration or loss of vitality of adjacent incisors can occur due to pressure from the crown of an ectopic canine. Tipping of lateral incisors can result from pressure exerted on its root by the crown of an erupting/ectopic canine.
Radiographic examination
Radiographic assessment of the position of an impacted maxillary canine is usually carried out by taking two radiographs from clearly different positions and applying the principle of radiographic parallax, first introduced by Clark in 1910.
The technique was described in detail as follows:19
‘In radiographic terms parallax (image/tube-shift) is the apparent displacement of an image, relative to the image of a reference object, caused by an actual change in the angulation of the x-rays. The reference object is normally the root of an adjacent tooth. The image of the tooth that is farther away from the x-ray tube moves in the same direction as the tube, and the image of the tooth that is closer to the x-ray tube moves in the opposite direction to the tube. A tube shift may be carried out in either the horizontal or the vertical plane’.
The best way for the clinician to remember this effect is to use the acronym SLOB = Same Lingual, Opposite Buccal.
Horizontal parallax
This can be carried out by taking the following combination of radiographs:
Anterior occlusal and periapical film with significant and easily identifiable horizontal tube-shift;
Two periapical films with significant and easily identifiable tube-shift;
Two occlusal radiographs.
Jacobs19 recommended taking two occlusal radiographs, as greater tube movement is possible when compared to two periapical radiographs and the radiation dose from two occlusal radiographs is comparable with that from two periapicals, however, the direction of the radiation is towards the patient's gonads, which is considered unacceptable whilst there are alternatives.
Vertical parallax
This can be carried out by taking the following combination of radiographs:
Periapical and OPT. However, the angular difference between these two radiographs is small, ranging from -7° to 23°, so vertical parallax is less useful.19
Anterior occlusal and OPT. This is the commonly used method for localization of an impacted canine. As an OPT is often taken as an initial radiograph, then one additional exposure, the occlusal radiograph, is taken to identify the canine position with confidence.
With this combination of radiographic examination, if the impacted canine tooth moves apical in relation to the adjacent tooth root on the occlusal radiograph, the position of the impacted teeth is palatal, as can be clearly seen in Figure 3 a and b. This is invaluable information for the surgeons when planning their flaps for canine exposure and bonding.
Figure 3. Vertical parallax to identify location of canine. (a) OPT shows tips of impacted canine teeth lie close to middle third of lateral incisor roots. (b) Tips of impacted canine teeth apparently move up, closer to apical third of lateral incisor roots, as the X-ray tube moves up. Tips move in the same direction as the tube therefore both the canines are palatal.
Other, less reliable, methods of locating impacted maxillary canine include:
‘Image Magnification’ ie a palatally displaced canine appears magnified on the OPT; and
‘Image Superimposition’ ie a palatally displaced canine appears superimposed on the root of adjacent incisors on the OPT.
Ericson and Kurol13 have reported that an OPT radiograph overestimates the angulation of the canines and underestimates the proximity of the impacted maxillary canine to the midline. These authors, in their study, also found that the positions of canines could be assessed with sufficient accuracy from the conventional periapical films in 92% of cases.
Computed tomography is, without doubt, the most precise method of radiographic localization. However, its relatively high radiation dose limits the indications for its use.20 Cone-beam computed tomography (CBCT) offers a lower dose alternative to conventional CT for the localization of ectopic canine teeth and its use is increasing for more complex cases (Figure 4).
Figure 4. A CBCT of a patient showing root resorption of lateral incisors caused by ectopically placed canine teeth.
Surgical exposure and bonding a gold chain attachment to impacted maxillary canine teeth is often required in order to bring the tooth into the dental arch and to allow subsequent alignment. A study conducted by Becker et al21 showed that bonding at the time of surgical exposure is superior to it being performed at a later date. Use of an eyelet attachment has a lower failure rate as compared to the use of a conventional orthodontic bracket. His study also showed that the palatal aspect of the canine offers the poorest bonding surface and also that pumicing the exposed tooth confers no advantage over immediate etching of exposed enamel. Another study by Pearson et al22 showed that a second surgical procedure may be required for up to 30% of cases, where the adhesive bond between the bracket and the tooth breaks down before or during orthodontic traction.
Surgical technique
In the UK, two techniques are routinely used to expose palatally displaced canines surgically.
The closed technique
This technique involves surgically exposing the crown of the impacted tooth and then etching the enamel and bonding an eyelet, to which is soldered a gold chain. The palatal flap is then replaced leaving the length of chain to exit the gingivae, the free end of which is sutured to the buccal mucosa. A few days after the surgery, gentle orthodontic traction can be applied to the tooth to start bringing it into its correct position within the dental arch. In the closed technique, the canine tooth is orthodontically moved into its correct position beneath the mucosa.
The open technique
This technique involves exposing a palatally displaced canine as before but instead of bonding a gold chain attachment to it at the time of surgery, the area of palatal mucosa which covers the crown of the tooth is cut out, to create a window, through which the crown is visible and the palatal flap is repositioned and sutured. A dressing pack is then used to cover the exposed area. This pack is removed in a few days and the canine is either allowed to erupt ‘naturally’ or, bonding a gold chain attachment to its crown, is carried out to allow gentle orthodontic traction to be commenced. In this technique, the canine tooth moves into its correct position above the mucosa. An advantage of this technique is that the orthodontist can bond the gold chain attachment to the crown of the canine, hopefully in the most favourable position.
In the UK, the surgical procedure of exposing a palatally impacted maxillary canine and bonding a gold chain is usually carried out under general anaesthesia. Even if general anaesthesia is used, a greater palatine nerve block, nasopalatine nerve block and local anaesthetic infiltration in the labial sulcus are recommended, as this will greatly reduce the chance of post-operative pain and discomfort (Figure 5). Local anaesthetic agents, such as lignocaine hydrochloride or longer-acting bupivacaine hydrochloride, with adrenalin as a vasoconstrictor, are commonly used.
Figure 5. Local infiltration of anaesthetic agent in the buccal sulcus.
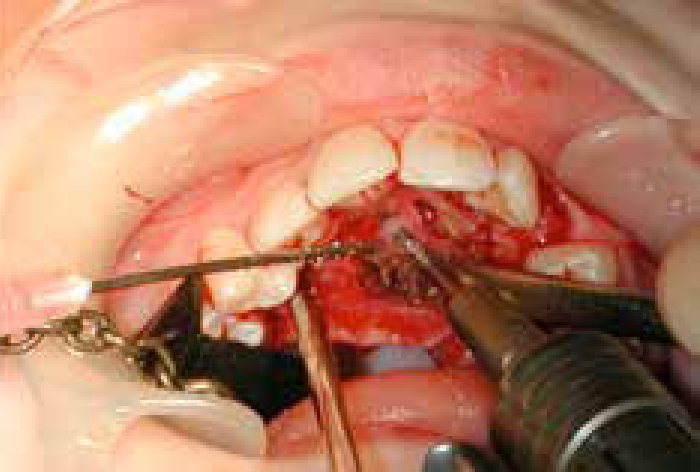
For unilateral impactions, the incision is commenced in the gingival crevice (Figure 6a) from mesial to first molar on the impacted side and is taken around the palatal gingival margin to the canine on the opposite side (Figure 6b and c). For bilateral canine impactions, the flap margin can be extended from first molar on one side of the arch to the first molar on the other side. A palatal flap is then raised by inserting the convex surface of a curved Warwick-James elevator in the inter-dental region and peeling back the gingival margin (Figure 7a and b). A Howarth's periosteal elevator can then be used to raise a full thickness mucoperiosteal flap, thus exposing the palatal bone (Figure 8a and b). The neurovascular bundle issuing from the incisive foramen is severed in this procedure but it rarely gives rise to clinically perceptible anaesthesia. Any bleeding that is difficult to arrest with pressure alone may require bipolar coagulation.
Figure 6.
(a) Incision is commenced in gingival crevice extending to the bone. (b, c) Crevicular incision continues around the palatal gingival margin.Figure 7.
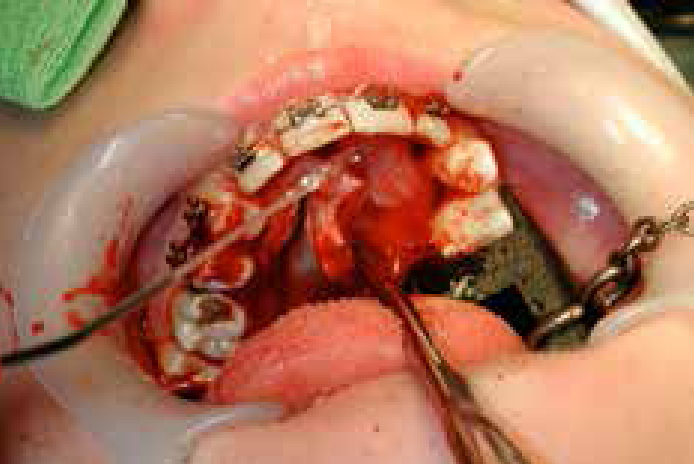
(a, b) Convex surface of a curved Warwick-James elevator is inserted in the inter-dental region to peel back the gingival margin.Figure 8.
(a, b) A Howarth's periosteal elevator is used to raise a full thickness mucoperiosteal flap thus exposing the palatal bone.
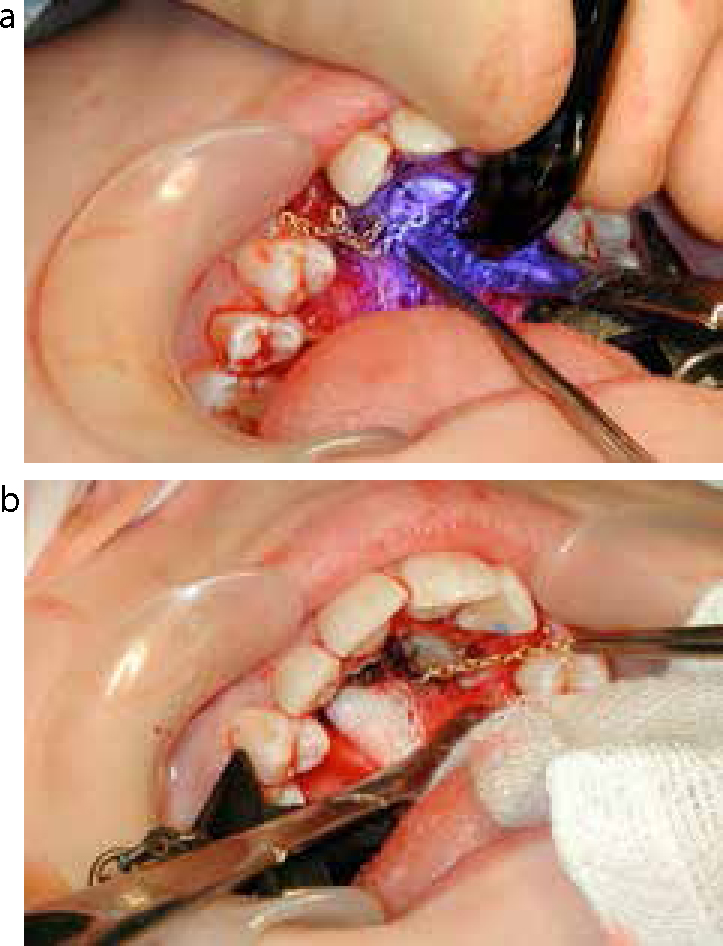
In the case of superficial impaction of a maxillary canine, the crown of the tooth may be visible once the mucoperiosteal flap has been raised. In cases where a thin plate of palatal bone covers the impacted canine, it can be easily chiselled away to expose the crown. Chisels can be used either by hand or, if the bone covering is thick, with a mallet (Figure 9). The bevelled side of the chisel is placed against the bone and is driven along at required depth to shave off successive wafers of the bone covering the impacted crown. A rosehead or fissure bur, in a surgical drill, is usually required to expose a crown fully, if covered by thick palatal bone. When using a drill to remove bone, it is important to ensure copious irrigation with sterile water in order to avoid any necrosis of bone due to the heat produced by high speed drilling (Figure 10). The amount of bone removal should be sufficient to free the crown down to its greatest circumference. Great care should be taken to ensure no damage is done to the impacted tooth crowns or roots of adjacent teeth (Figure 11).
Figure 9. A mallet and chisel used to remove, gently and carefully, palatal bone covering impacted crown.Figure 10. When using a drill to remove bone, it is important to ensure copious irrigation with sterile water.Figure 11. The exposed crown of palatally impacted canine.
Once the crown of the impacted canine is sufficiently exposed, a clean dry field is essential to bond a gold chain to the exposed crown successfully. A gold chain is attached to whatever enamel is most easily accessible on the canine crown. The orthodontic bracket can later be bonded to the labial aspect of the tooth once it is sufficiently erupted, following initial orthodontic traction.
Traditionally, once adequate moisture control was achieved, acid-etch with 33% buffered orthophosphoric acid was applied to the surface of exposed crown. An etch time of 20–30 sec is usually sufficient (Figure 12). It is important to ensure that the surface of the enamel is not rubbed during the etching process as the rubbing action will break all the enamel prisms that stick up from the surface and the crevices, and cracks for resin tag formation will be lost.23 Acid etching of enamel increases the surface roughness of the enamel and hence the bonding area. It also raises the surface energy of enamel by removing surface contaminants. This provides for a better wettability of the enamel by the adhesive. The etched tooth surface is then washed with sterile water, not saline, for at least 10 sec (Figure 13) and is thoroughly dried with a chip syringe (Figure 14). Dried etched enamel appears matt, white and frosty. An eyelet attached to a gold chain is now bonded to the etched enamel using a light-cure composite material (Figure 15a and b).
Figure 12. The exposed tooth surface is etched for 30 seconds.Figure 13. The etched tooth surface is then washed with sterile water, not saline, for at least 10 seconds.Figure 14. A chip syringe is used to ensure the enamel is dry and has a frosted appearance.Figure 15.
(a) An eyelet attached to a gold chain is bonded to the etched enamel using a light-cure composite material. (b) Pull gently on gold chain to check bond is firm.
More recently, self-etching primers (SEP) have become much more popular in orthodontics and it is now recommended that this is used by surgeons, as the second washing and drying phase is deemed unnecessary. Once the exposed crown is initially cleaned and dried, the SEP is applied and left in place for 15–20 seconds. The bracket base or eyelet can then be stuck to the canine crown. Not only is there a significant time saving, but the risk of crown contamination is also reduced.
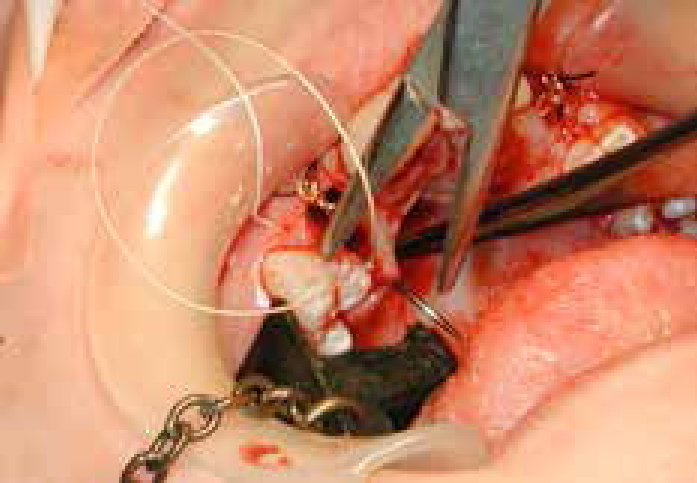
Once the gold chain is attached to the crown, its loose end can be sutured to mucosa in the depth of labial sulcus using a black silk suture in order to secure it, until the orthodontist reviews the patient. It is recommended for the surgeon to tie a really loose knot, 5–10 mm diameter, so it can be easily cut and the suture removed by an orthodontist, at a subsequent appointment (Figure 16a). It is exceedingly unhelpful if a tight knot is tied in the buccal sulcus, as these can be difficult and painful to cut at a later date (Figure 16b).
Figure 16.
(a) The other end of the gold chain is sutured to mucosa in the depth of labial sulcus by tying a loose knot of 5-10 mm diameter so it can be easily cut at a subsequent appointment. (b) A black silk suture tied much too tight for easy removal by the orthodontist!
The palatal mucoperiosteal flap is then replaced and sutured using 3.0 vicryl rapide sutures (Figure 17). Vertical mattress sutures can be used to minimize any chances of palatal haematoma formation. The gold chain attached to the tooth, tunnels subgingivally and comes out at the margin of flap, so it is easily accessible for the orthodontist, at a later date.
Figure 17. The palatal mucoperiosteal flap is replaced and sutured using 3.0 vicryl rapide sutures..
The orthodontist can review the patient in a couple of weeks' time and then gentle traction can begin to be applied to the impacted canine by including the gold chain into the fixed orthodontic appliance.
Discussion
The Cochrane review on open versus closed surgical exposure of canine teeth has revealed that, currently, there is no evidence to support one surgical technique over the other in terms of dental health, aesthetics, economics and patient factors.24 The decision on how to approach the clinical problem will therefore be made by the orthodontist and the surgeon, depending upon their beliefs. Whichever technique is chosen, care must be taken to maximize the chances of a favourable outcome. Adequate surgical access is always required in order to allow sufficient exposure of the crown of the impacted tooth and subsequent bonding of the gold chain attachment.
Care must be taken to leave the chain in an easily accessible position whereby the orthodontist can review and take over the case. If the chain has been correctly positioned, the direction of pull should be at the most favourable angle. In most circumstances, the chain will exit the crestal incision and will be subsequently included in the full upper fixed appliance, either directly or with a ‘piggyback’ archwire (Figure 18). With either the closed or open methods, larger quantities of bone removal at the time of surgery increase the chance of bone defects following orthodontic treatment.25 An atraumatic surgical procedure will increase chances of minimal postoperative complications and a rapid recovery. Use of good effective and efficient bonding technique, making use of the latest orthodontic materials, will reduce the chances of bond failure, necessitating a second surgical procedure.
Figure 18. A ‘piggyback’ archwire to pick up canines.
Conclusions
Use of a careful and meticulous surgical technique when dealing with impacted canines will greatly ease the subsequent work the orthodontist has to do, to maximize the chances of a favourable result for the patient.