Hurme VO. Ranges of normalcy in the eruption of permanent teeth. J Dent Child. 1949; 16:11-15
Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 1988; 10:283-295
Thilander B, Jakobsson SO. Local factors in impaction of maxillary canines. Acta Odontol Scand. 1968; 26:145-168
Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992; 101:159-171
McSherry PF. The ectopic maxillary canine: a review. Br J Orthod. 1998; 25:209-216
Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005; 128:418-423
Patel D, Taylor NG. Are patients with impacted canines referred too late?. Br Dent J. 2016; 221:561-564
Moyers RE, van der Linden Riolo ML, McNamara JA.Ann Arbor: Center for Human Growth and Development, University of Michigan; 1976
Coulter J, Richardson A. Normal eruption of the maxillary canine quantified in three dimensions. Eur J Orthod. 1997; 19:171-183
Becker A, Chaushu S. Etiology of maxillary canine impaction: a review. Am J Orthod Dentofacial Orthop. 2015; 148:557-567
Power SM, Short MB. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favourable eruption. Br J Orthod. 1993; 20:215-223
Jacoby H. The etiology of maxillary canine impactions. Am J Orthod. 1983; 84:125-132
Becker A. In defense of the guidance theory of palatal canine displacement. Angle Orthod. 1995; 65:95-98
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:249-256
Lai CS, Bornstein MM, Mock L Impacted maxillary canines and root resorptions of neighbouring teeth: a radiographic analysis using cone-beam computed tomography. Eur J Orthod. 2013; 35:529-538
Alemam AA, Abu Alhaija ES, Mortaja K, AlTawachi A. Incisor root resorption associated with palatally displaced maxillary canines: analysis and prediction using discriminant function analysis. Am J Orthod Dentofacial Orthop. 2020; 157:80-90
Ngo CTT, Fishman LS, Rossouw PE Correlation between panoramic radiography and cone-beam computed tomography in assessing maxillary impacted canines. Angle Orthod. 2018; 88:384-389
Chaushu S, Kaczor-Urbanowicz K, Zadurska M, Becker A. Predisposing factors for severe incisor root resorption associated with impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2015; 147:52-60
Sosars P, Jakobsone G, Neimane L, Mukans M. Comparative analysis of panoramic radiography and cone-beam computed tomography in treatment planning of palatally displaced canines. Am J Orthod Dentofacial Orthop. 2020; 157:719-727
Parkin N, Furness S, Shah A Extraction of primary (baby) teeth for unerupted palatally displaced permanent canine teeth in children. Cochrane Database Syst Rev. 2012; 12
Baccetti T, Leonardi M, Armi P. A randomized clinical study of two interceptive approaches to palatally displaced canines. Eur J Orthod. 2008; 30:381-385
Leonardi M, Armi P, Franchi L, Baccetti T. Two interceptive approaches to palatally displaced canines: a prospective longitudinal study. Angle Orthod. 2004; 74:581-586
Baccetti T, Mucedero M, Leonardi M, Cozza P. Interceptive treatment of palatal impaction of maxillary canines with rapid maxillary expansion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2009; 136:657-661
Baccetti T, Sigler LM, McNamara JA An RCT on treatment of palatally displaced canines with RME and/or a transpalatal arch. Eur J Orthod. 2011; 33:601-607
Armi P, Cozza P, Baccetti T. Effect of RME and headgear treatment on the eruption of palatally displaced canines: a randomized clinical study. Angle Orthod. 2011; 81:370-374
Bazargani F, Magnuson A, Lennartsson B. Effect of interceptive extraction of deciduous canine on palatally displaced maxillary canine: a prospective randomized controlled study. Angle Orthod. 2014; 84:3-10
Naoumova J, Kjellberg H. The use of panoramic radiographs to decide when interceptive extraction is beneficial in children with palatally displaced canines based on a randomized clinical trial. Eur J Orthod. 2018; 40:565-574
Naoumova J, Kurol J, Kjellberg H. Extraction of the deciduous canine as an interceptive treatment in children with palatal displaced canines – part I: shall we extract the deciduous canine or not?. Eur J Orthod. 2015; 37:209-218
Naoumova J, Kürol J, Kjellberg H. Extraction of the deciduous canine as an interceptive treatment in children with palatally displaced canines – part II: possible predictors of success and cut-off points for a spontaneous eruption. Eur J Orthod. 2015; 37:219-229
Interceptive Management of Palatally Displaced Canines: Evidence-based Clinical Guidelines Aslam Alkadhimi John Ahn Susan Power Dental Update 2025 49:3, 239-245.
The orthodontic alignment of palatally displaced canines (PDC) can be complex, with potential dental and soft tissue morbidity. Early diagnosis and provision of appropriate interceptive treatment has been shown to reduce the need for surgical exposure and extensive orthodontic treatment. This article reviews the current literature to gain insight into best available research evidence on all types of interceptive measures for the management of PDCs. Other perspectives of the PDC including development, aetiology and assessment are also be discussed.
CPD/Clinical Relevance: Interceptive management of PDCs by extracting primary predecessors requires an assessment of the determinant prognostic factors for treatment success and to avoid the removal of primary canines where improvement in PDC is unlikely or where retention of the primary tooth may be the preferred long-term option.
Article
The permanent maxillary canine erupts at a mean age of 10.5 years in girls and 11.5 years in boys, with individual variation of 3–4 years.1,2 The eruption of the maxillary canine should be considered late if it is not clinically visible by the age of 12.3 years in girls or 13.1 years in boys.3 If the maxillary canine is not palpable in the buccal sulcus by the age of 10–11 years, canine ectopia should be suspected and further investigations warranted.4
According to one classical study carried out by Ericson and Kurol,4 maxillary canines are positioned palatal to the dental arch in 85% of the cases and buccal in only 15% of the cases.4 The term palatally displaced canine (PDC), historically refers to a ‘developmental dislocation with genetic predisposition of the canine towards the palatal region,’5 although this definition is not entirely accurate given that the aetiology is thought to be multifactorial in nature (interplay between genetic and environmental factors), which will be discussed further.
Palatal displacement of the maxillary canine most often leads to its impaction, and in some cases, can lead to sequelae such as root resorption of the permanent incisors and/or formation of dentigerous cysts.6,7 Root resorption of the lateral incisors is not uncommon. It has been reported that 66.7% of the lateral incisors and 11.1% of central incisors had root resorption associated with PDCs.8
To reduce the incidence of these potential sequelae, early diagnosis of palatal displacement is necessary and, if diagnosed early, the PDC can be managed with appropriate interceptive measures. Unfortunately, not all patients with PDC are referred or managed early and this can reduce the success rate of any attempted interception, and increases the risks of the aforementioned sequelae. Patel and Taylor showed that 76% of patients were referred late (>12 years, mean age of 14.1 years) for the management of ectopic maxillary canines when compared to the recommendation made by the Royal College of Surgeons of England where the ideal age for interceptive intervention is between 10 and 13 years.9,10 The general dental practitioner (GDP) is well placed to diagnose PDCs early and manage appropriately (in the form of interceptive management or refer to the orthodontist for management). With early or timely diagnosis and interception, and with interdisciplinary care from the GDP and the orthodontist, PDCs can be managed successfully.
Aims
The aims of the present article are to:
Present the literature regarding the determinant prognostic factors related to spontaneous eruption of PDCs;
Present a flowchart to assist the decision-making process in the interceptive management of PDCs.
Development of the permanent canine
Calcification of the permanent maxillary canine begins at approximately 4–5 months of age between the roots of the first primary molar. As the primary teeth erupt, the canine crypt migrates forward in the maxilla at a greater rate than that of the primary teeth themselves.11 The maxillary canines erupt approximately at the age of 11–12 years, earlier in females than males.12
Key Points
The maxillary canine has the longest path of eruption. From the age of 5 to 15 years, the maxillary canine travels approximately 22 mm in the three planes. This is thought to be one of the reasons why some canines become palatally displaced.
Aetiology
Numerous investigations have been carried out over the decades to identify aetiological factors in the development of PDCs; however, the exact aetiology remains unknown. Any alteration in the local environment of the permanent maxillary canine by hard tissues, soft tissues or other developmental abnormalities can cause impaction of the tooth.13 Multiple factors have been implicated including dento-alveolar disproportion (tooth size–arch length discrepancy), prolonged retention of the primary canine, trauma, long path of eruption, root dilaceration, abnormal position of the tooth bud and/or ankyloses.14 Jacoby reported that 85% of PDCs had sufficient space for eruption, but failed to erupt, indicating other factors contribute towards the maxillary canine becoming palatally impacted.15 There have been two accepted, yet widely debated, theories explaining the aetiology of PDCs. The guidance theory, which suggests that the eruption of the maxillary canine is guided by the labio-distal surface of the lateral incisor root.16 Thus, abnormally formed (peg-shaped) or developmentally absent lateral incisors are contributing variables to the causation of PDCs. On the other hand, the genetic theory suggests that there is no cause- and-effect relationship between impaction of the canines and environmental factors, rather the occurrence of PDCs is likely to be a consequence of possible polygenic inheritance.17 This theory was based on the observation that PDCs were generally accompanied by other dental anomalies such as hypodontia and microdontia, bilateral occurrence, familial tendency, female predilection and population differences.17
Key Points
Palatal displacement of permanent maxillary canines is caused by a complex multifactorial interplay between genetic and environmental factors.
Assessment
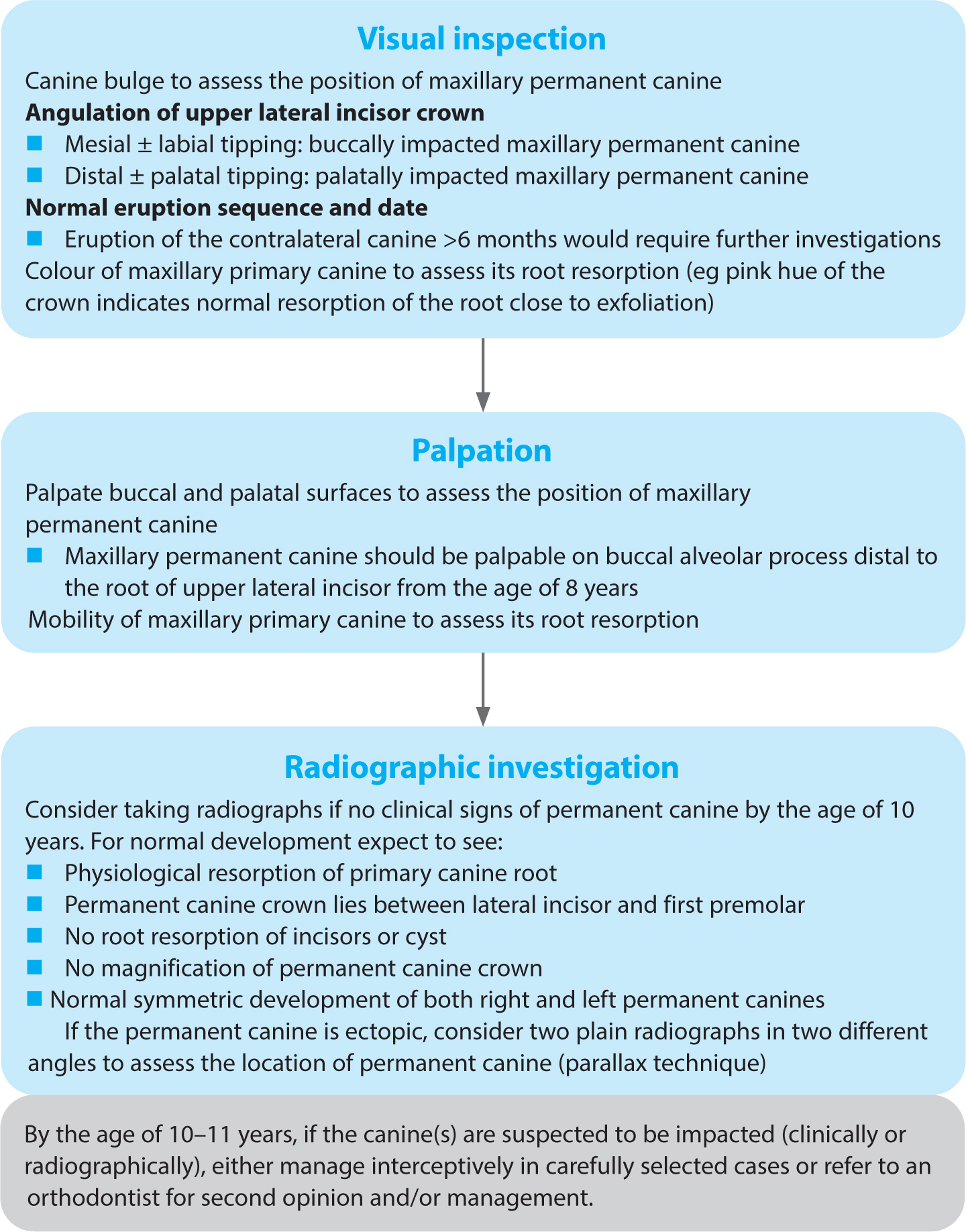
Assessment of permanent maxillary canine development should be carried out clinically, followed by radiographs if indicated (Figure 1). Clinical assessment should involve both visual inspection and digital palpation. Digital palpation of the buccal surface of the alveolar process, just distal to the lateral incisor should be performed from the age of 8 years onwards. By the age of 10−11 years, a normally positioned canine is usually palpable buccal to the deciduous predecessor. Plain film radiographs are indicated when there is asymmetric eruption between right and left canines, when the canines are not palpable in the normal position by the age of 10–11 years or when the lateral incisor is late erupting (Figure 1). Radiographic assessment should ideally include the application of parallax, using two plain film radiographs at different angles to identify the buccal/palatal position of the permanent canine (although localization of the canine is usually done by the orthodontist). The orthodontist may then consider, in carefully selected cases, taking a cone beam computed tomograph (CBCT) to ascertain whether any incisor root resorption has occurred. The advent of CBCT has led to the recognition that a higher percentage of PDCs cause incisor root resorption than previously seen from plain films.18,19,20,21,22 The interpretation of CBCT is outside the scope of this article and the reader is directed to appropriate relevant literature.
Figure 1. Assessment of permanent canine development.
Key Points
For cases with identified risks (eg root resorption of incisors or cystic formation around the PDC), CBCT may be indicated. However, if indicated, a CBCT is best prescribed by the orthodontist with the responsibility for subsequent management.
Predictors of root resorption from plain film radiographs may be used to decide if a CBCT is indicated; however, the evidence is equivocal in that regard.
Management options
Once a diagnosis of PDC is made, there are five general treatment options:10
Interceptive treatment by extraction of the primary canine (and space creation, if required)
Surgical exposure and orthodontic alignment;
Surgical removal of the PDC;
Transplantation;
No active treatment/leave and observe.
This article focuses on the first option, interceptive management of PDCs in all its forms, with the aim of exploring the recent developments in the literature.
Interceptive management
One interceptive measure, suggested to prevent impaction of the permanent canine, is to extract the primary canine in patients aged 10–13 years, provided that there is enough space for the permanent canine.4 This theory arose from a prospective case series following a consecutive group of children aged 10–13 years, with extraction of the primary canine. There was, however, no control group. They found that following the extraction of the primary canine, 78% of the PDCs reverted to a normal path of eruption after 6–12 months of monitoring. Based on this study, the Royal College of Surgeons in England published guidelines in 1997 supporting interceptive extraction of the primary canine to encourage the eruption of PDC in a more normal pathway. These clinical guidelines have been updated.10
A 2012 Cochrane review concluded that ‘there was currently no evidence of the effects of extraction of primary canine teeth in 10–13-year-old children with one or two palatally displaced permanent canine teeth’.23 The review included two randomized controlled trials.24,25 These two RCTs included approximately 128 children, with more than 150 PDCs. The reviewers pointed out that data presented in the trial reports were either incomplete or inconsistent. Both RCTs were judged to be at high risk of bias and both trials had serious deficiencies in the way they were designed, conducted and reported. This Cochrane review has recently been withdrawn and a new protocol published in 2018 to update the review.
Other methods that can be used (along with the extraction of the primary canine) as interceptive measures include rapid maxillary expansion (RME) to gain space by expanding the maxillary arch and/or preventing the mesialization of upper permanent molars by using cervical pull head gear (HG).24,25,26 Several randomized trials have investigated the effect of interceptive measures, two of which were included in the aforementioned Cochrane review.24,25 These trials suggested that interceptive measures including extraction of the primary canine, cervical pull HG, RME and trans palatal arch (TPA) can help in preventing impaction of the permanent canine, thus reducing the need for surgical management and lengthy orthodontic treatment.24,25,26,27,28,29,30,31,32
Determinant prognostic factors
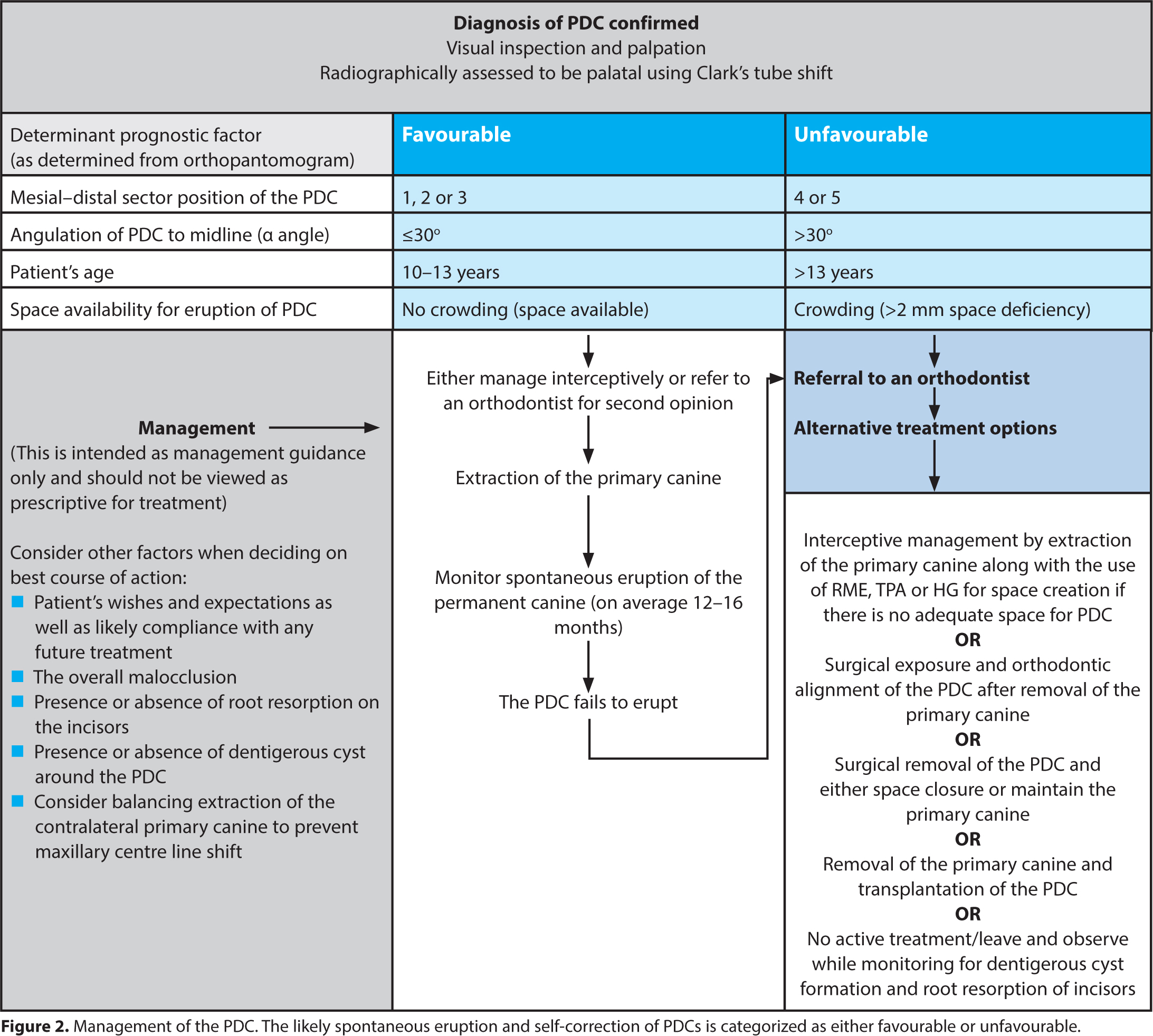
Multiple factors have been cited in the literature as influencing the eruption and self-correction of PDCs. The determinant factors discussed in this article are based on the included RCTs only providing the highest level of evidence,24,25,26,27,28,29,30,31,32 and used to construct a clinical decision tree (Figure 2). This decision tree may be used by orthodontists and general dental practitioners.
Figure 2. Management of the PDC. The likely spontaneous eruption and self-correction of PDCs is categorized as either favourable or unfavourable.
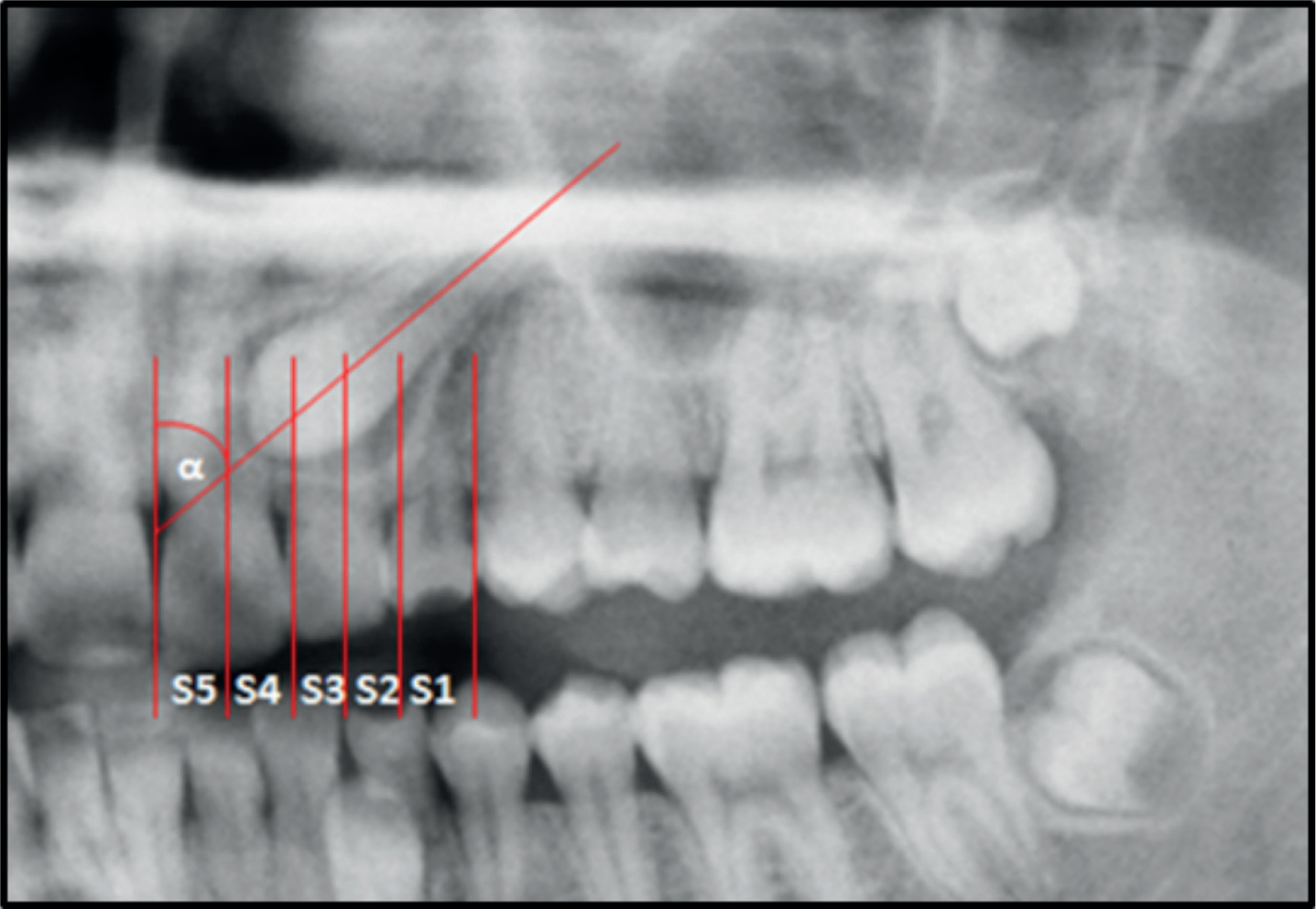
Mesial-distal sector positions
Canine sectors can be determined only from panoramic radiographs (Figure 3). Determining canine position in relation to sector is very important to determine the effect of interceptive management by extracting primary predecessors to allow spontaneous correction and eruption of PDC. There are five sectors in the horizontal plane as determined from panoramic radiographs (Figure 3). Following removal of the maxillary primary canines, Bazargani et al concluded that there was a tendency towards a weaker response of the PDCs in the mesial sectors (4 and 5) to interceptive extraction of the primary canine.29
Figure 3. Measurements made on the panoramic radiograph according to the method first described by Ericson and Kurol:4 α-angle, angle formed by the long axis of the canine and the midline; sector (S), the mesiodistal crown position of PDC in sectors 1–5. In this case, the UL3 is in S4 and α-angle is 48°, therefore, interceptive extraction of ULC alone is not recommended.
Naoumova et al suggested that if a PDC is located in sector 4 with an alpha angle >30 degrees, then surgical exposure is indicated. On the other hand, canines angulated less than 20 degrees to the midline and located in sector 2 can be monitored without prior interceptive extraction.32
Key points
PDCs in sectors 1, 2, and 3 would probably benefit from extraction of maxillary primary canines, whereas PDCs in sectors 4 or 5 are unlikely to improve, and should be referred to an orthodontist, without extracting primary canines, to start comprehensive treatment with fixed appliances. Avoiding extraction in cases where the PDC is located in sectors 4 or 5 is very important to avoid any space loss, which can complicate the future orthodontic treatment.
Canine angulation
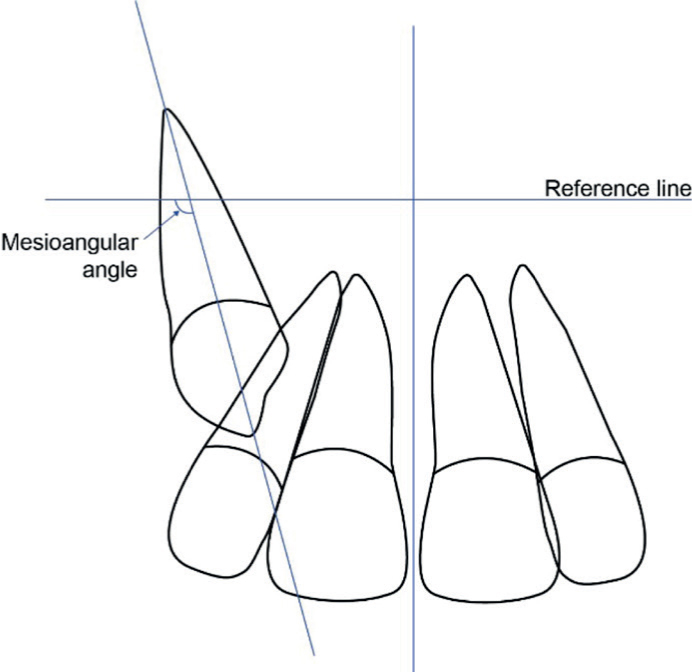
The second factor to determine the prognosis and response of a PDC is canine angulation in relation to the midline (alpha angle (α)). Again, this can be determined only from panoramic radiographs (Figure 3). The smaller the alpha angle (ie the more vertical the canine is), the better the prognosis. A clear-cut measurement regarding the alpha angle and prognosis is different between studies.27,39,30,32 Generally speaking, an alpha angle less than 30 degrees (ie more vertical) has a better prognosis than a PDC with an alpha angle more than 30 degrees. If using CBCT imaging, another angle can be measured to determine prognosis for successful eruption of PDC, the mesioangular angle (Figure 4). This angle can only be measured on CBCT (unlike the alpha angle which can be measured from panoramic radiograph) from a coronal view by measuring the angle between a horizontal reference line and the long axis of the canine.31 A mesioangular angle equal to or less than 103 degrees is associated with a higher success rate for spontaneous eruption of the PDC.31
Figure 4. Mesioangular angle of a right PDC. This can be estimated from a coronal view of a CBCT.
Key points
The smaller the α-angle, the better the success rate for interceptive management. An α-angle of less than 30 degrees was shown to be a possible cut-off point.
Patient's age
It is important to note that interceptive extraction of the primary maxillary canine should only be considered for patients between the ages of 10 and 13 years. In older patients, the position of a PDC is less likely to improve with the extraction of the primary canine. Therefore, alternative treatment options should be considered.29
Multiple RCTs have concluded that if the patient's age at the time of intervention by extracting primary canines is below 13 years, more significant improvement and self-correction of the PDC would occur. Patients older than 13 years show a significantly poorer response to interceptive treatment.29,30,32
Key points
Interceptive treatment (in the form of primary canine extraction) is recommended in patients aged 13 years or younger, assuming that the other factors are favourable.
Amount of space available
The final factor that influences the eruption of PDC after interceptive treatment is the amount of space available at the PDC region. Lack of space (or crowding) at the PDC region is considered as a contraindication to interceptive extraction of the primary canines.27,28 Crowding in the maxillary arch exceeding 2 mm is considered a limiting factor in success rate for eruption of the PDC.31 If extraction of primary canines is performed in these cases, the crowding is most likely to be resolved by the unwanted movement of the anterior and posterior teeth into the resultant extraction space, preventing eruption of the PDC (Figure 5). Other treatment alternatives may also be used in combination with the extraction of primary canines such as maxillary arch expansion (with RME),26,28 distalization of the buccal segments (with HG)24,25,28 or anchorage reinforcement to prevent mesial migration of first permanent molars (with TPA).27 However, it must be emphasized that these techniques have only been investigated in a limited number of low-quality trials, and so they are not widely adopted except in carefully selected cases, and better carried out by the treating orthodontist.
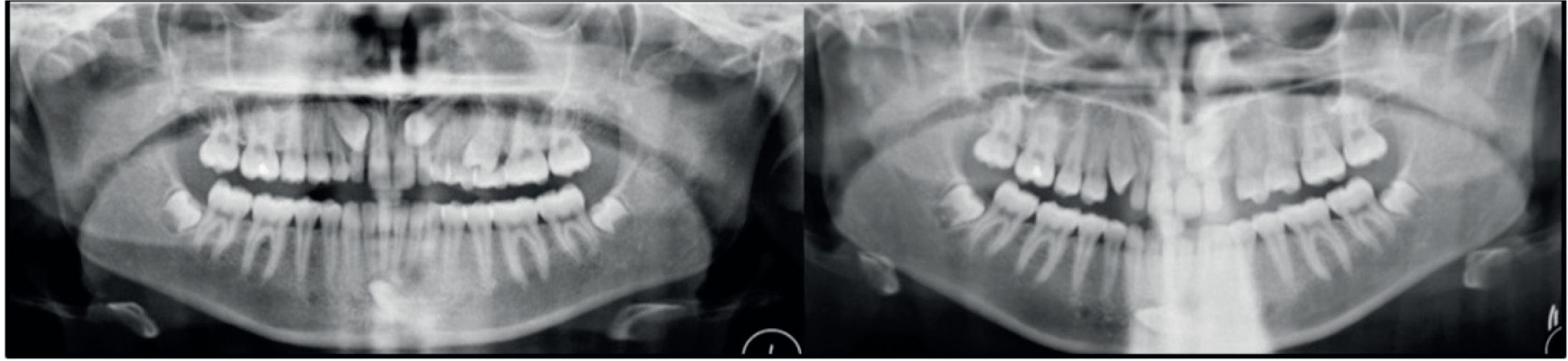
Figure 5. A 13-year-old girl with bilateral PDCs. (a) UR3 was in S3, α-angle was 20° and there was no crowding in the upper right quadrant. UL3 was in S4, α-angle was 40° and there was space deficiency in the upper left quadrant. Both URC and ULC were extracted. (b) Updated panoramic radiograph at 6 months shows the self-correction and normalization of UR3, while there was no improvement of the UL3. Surgical exposure and orthodontic alignment are required for the UL3.
Key points
There is a small body of evidence to suggest that additional interceptive treatment, in addition to the extraction of primary canine, (RME, HG and TPA) can be effective, and can increase the success rate for eruption of PDC. However, the evidence is generally of low–moderate quality and associated with high risk of bias.
Key Points
The current evidence shows that interceptive extraction of the primary canine can be a successful treatment modality in carefully selected cases of PDCs.
Timely management of PDCs by extracting the primary predecessors could significantly decrease the overall treatment time and complexity of future orthodontics. However, the patient/parent must be made aware that surgical exposure and orthodontic treatment may ultimately be required.
Flowcharts (decision trees) are presented in this article to help simplify the assessment and interceptive management of PDCs.
In patients where active orthodontic treatment is contraindicated, interceptive management in the form of removal of the primary predecessor may not be ideal, as it may commit the patient to future active orthodontic treatment, removing the option of accepting the primary canine long term. Therefore, it is important to liaise with an orthodontist.
Conclusion
Good planning requires careful assessment of the determinant prognostic factors associated with the PDC (mesial-distal sector position, alpha angle, patient's age and amount of space available), as well as determination of the future need for orthodontics. The current evidence confirms that early diagnosis and careful assessment of the canine position determines the success of interceptive management for PDCs.