References
Echarri P. Revisiting the history of lingual orthodontics: a basis for the future. Semin Orthod. 2006; 12:153-159
Fujita K. New orthodontic treatment with lingual brackets and mushroom archwire technique. Am J Orthod. 1979; 76:657-675
Geron S. Self-ligating brackets in lingual orthodontics. Semin Orthod. 2008; 14:64-72
McCrostie HE. Lingual orthodontics: the future. Semin Orthod. 2006; 12:211-214
Kurz C, Swartz ML, Andreiko C. Lingual orthodontics: a status report. Part 2. Research and development. J Clin Orthod. 1982; 16:735-740
Shpack N, Geron S, Floris I, Davidovitch M, Brosh T, Vardimon AD. Bracket placement in lingual vs labial systems and direct vs indirect bonding. Angle Orthod. 2007; 77:509-517
Buso-Frost L, Fillion D. An overall view of the different laboratory procedures used in conjunction with lingual orthodontics. Semin Orthod. 2006; 12:203-210
Fillion D. Clinical advantages of the Orapix-straight wire lingual technique. Int Orthod. 2010; 8:125-151
Fillion D. Up-to-date lingual indirect bonding procedure. J Lingual Orthod. 1999; 1:4-8
Geron S. Finishing with lingual appliances, problems and solutions. Semin Orthod. 2006; 12:191-202
Gorman JC, Smith RJ. Comparison of treatment effects with labial and lingual fixed appliances. Am J Orthod Dentofacial Orthop. 1991; 99:202-209
Liang W, Rong Q, Lin J, Xu B. Torque control of maxillary incisors in lingual and labial orthodontics: a 3-dimensional finite element analysis. Am J Orthod Dentofacial Orthop. 2009; 135:316-322
Echarri P. Lingual orthodontics: patient selection and diagnostic considerations. Semin Orthod. 2006; 12:160-166
Van der Veen MH, Attin R, Schwestha-Polly R, Wiechmann D. Caries outcome after orthodontic treatment with fixed appliances: do lingual brackets make a difference?. Eur J Oral Sci. 2010; 118:298-303
Hohoff A, Seifert E, Fillion D, Stamm T, Heinecke A, Ehmer U. Speech performance in lingual orthodontic patients measured by sonography and auditive analysis. Am J Orthod Dentofacial Orthop. 2003; 123:146-152
Miyawaki S, Yasuhara M, Koh Y. Discomfort caused by bonded lingual orthodontic appliances in adult patients as examined by retrospective questionnaire. Am J Orthod Dentofacial Orthop. 1999; 115:83-88
Wu AKY, McGrath C, Wong RWK, Wiechmann D, Rabie ABM. A comparison of pain experience by patients treated with labial and lingual orthodontic appliances. Eur J Orthod. 2010; 32:403-407
Caniklioglu C, Oztürk Y. Patient discomfort: a comparison between lingual and labial fixed appliances. Angle Orthod. 2005; 75:86-91
Wiechmann D, Gerb J, Stamm T, Hohoff A. Prediction of oral discomfort and dysfunction in lingual orthodontics: a preliminary report. Am J Orthod Dentofacial Orthop. 2008; 133:359-364
Stamm T, Hohoff A, Ehmer U. A subjective comparison of two lingual bracket systems. Eur J Orthod. 2005; 27:420-426
Fritz U, Diedrich P, Wiechmann D. Lingual technique – patients' characteristics, motivation and acceptance. Interpretation of a retrospective survey. J Orofacial Orthop. 2002; 63:227-233
Shum LM, Wong R, Hagg U. Lingual orthodontics – a review. Hong Kong Dent J. 2004; 1:13-20
Gorman JC, Hilgers JJ, Smith JR. Lingual orthodontics: a status report. Part 4. Diagnosis and treatment planning. J Clin Orthod. 1983; 17:26-35
Wiechmann D, Rummel V, Thalheim A, Simon J-S, Wiechmann L. Customized brackets and archwires for lingual orthodontic treatment. Am J Orthod Dentofacial Orthop. 2003; 124:593-599
Invisible orthodontics part 2: lingual appliance treatment
From Volume 40, Issue 5, June 2013 | Pages 391-402
Article

A review of the literature1 suggests that, as far back as 1726, Fauchard introduced using appliances on the lingual surfaces of teeth. However, it was Fujita2 in the 1970s who is credited with pioneering modern lingual treatment with lingual brackets and ‘mushroom-shaped’ archwires. Interestingly, this came about to address the demands of martial artists undertaking orthodontic treatment. The poor outcome of completed cases triggered a drop in interest in the 1990s, but with technological advances there has been a recent resurgence in the use of lingual appliances.
Bracket mechanics
Since the initial suggestion that brackets could be placed behind the teeth in the 70s, several American orthodontists formed the Lingual Task Force to promote the use of lingual appliances. This has led to the development of numerous lingual appliance systems. Table 1 gives a breakdown of the brackets currently available. Ormco Corporation (Orange, CA, USA) produced one of the first bracket systems following work undertaken by Kurz et al;5 this was placed as an edgewise appliance. As access is difficult and there is a lack of direct visualization of the lingual surfaces, numerous indirect bonding set-up systems have developed as an alternative to direct bonding. Published research has suggested significant improvement in bracket position with reduced torque and rotational errors using an indirect bonding system.6 A high degree of accuracy can therefore be achieved using these techniques in bracket positioning. The chairside bond-up time is also reduced. Table 2 lists some of the main bracket set-up systems and outlines their main features. Actual bonding protocols have also advanced over the last decade. Previous problems relating to the increased debonding of brackets negatively influenced the lingual technique in the US during the 1980s.9 The standard technique was difficult to employ with bracket positional discrepancies and inaccuracies in finishing.
| Conventional Brackets1 | |
| Ormco 7th Generation Lingual Bracket |
|
| Incognito/iBraces |
|
| Self-Ligating Brackets3,4 | |
| Forestadent Philippe 2D SL Bracket |
|
| Forestadent 2D Lingual SL Bracket – 3rd Generation |
|
| Adenta Evolution LT – 2nd Generation |
|
|
Ormco Scuzzo/Takemoto Bracket (STb)
|
|
| GAC In-Ovation-L Bracket |
|
| Gestenco Phantom Bracket |
|
| Lab System | Set-Up Model? | Mode of Positioning | Advantages | Disadvantages |
|---|---|---|---|---|
| CLASS System (Custom Lingual Appliance Set-up Service) | √ | Separate metal plates aid anterior/posterior positioning Transfer to original model via acrylic caps | 1st order bends not needed in labial segment as tooth thickness factored in | Multi-step process Errors in transfers cumulative |
| TARG System (Torque Angulation Reference Guide) | Χ | Brackets at same distance from incisal/occlusal plane Silicone/thermoplastic transfer tray | Possible to prescribe torque & angulation for each tooth individually | Many 1st order bends required as thickness of teeth not factored in |
| BEST System (Bonding with Equal Specific Thickness) | Χ | Caliper to measure tooth thickness |
No need for bends in anterior section of wire | Archwire bends between canine and premolar, premolar and molar required |
| LBJ (Lingual Bracket Jig) | Χ | Set of 6 anterior, 1 universal posterior jig plus a special ruler |
Allows indirect and direct bracket positioning | Limited number of jigs available |
| TOP (Transfer Optimized Positioning) | √ Virtual target set-up | TARG Professional used |
High levels of precision | Customized brackets with high gold content expensive |
| KIS System (Korean Indirect Bonding Set-Up) | √ | All brackets positioned at once | Simpler and faster |
Special model gauge required for precise set-up model |
| Hiro System | √ | Full-sized rigid rectangular wire used to aid bracket positioning Individual bracket transfer trays made | No need for 1st order bends in labial segment (customized resin pads) | Initial bond-up appointment longer Need new tray if debond occurs |
| Orapix System | √ Virtual Set-up | Model scanned to create 3D data file (3Dxer) |
Straightwire principles can be used |
Orapix software required by clinician to finalize the set-up |
There are both clinical and biomechanical differences between labial and lingual orthodontics. Lingual tooth surfaces have a greater slope than the labial side and a more irregular anatomical form. The built in bracket prescription tends to be expressed later in lingual treatment.10 It is harder to correct rotations due to the small arch perimeter and the decreased interbracket distance. Kurz and Bennett suggest the shorter interbracket distance decreases torque control and leads to a more obtuse interincisal angle and more upright incisors, especially in extraction cases.11 In the horizontal plane, the inter bracket distance is reduced compared to labial orthodontics, which produces less flexibility in the archwire. Therefore a more flexible wire should be used to compensate for this and allow for physiological tooth movement. A 3D finite element model study12 found identical loads in labial and lingual orthodontics produce very different results – translation and uncontrolled tipping with intrusion, respectively. When retracting incisors it is suggested that one uses mild forces and that the root torque is increased.
Most bracket systems rely on the use of ‘mushroom-shaped’ archwires with canine, premolar and molar offsets (Figure 1) as their set-up method is based on individualized resin pads to compensate for the differences in tooth thicknesses. This results in particularly the incisor attachments being further from the lingual surfaces, compounding known difficulties with anterior torque control in lingual appliances. The mushroom archwire formation has an area of weakness between the canines and premolars, which is prone to fracturing. More recently, lingual straightwire techniques have evolved with modifications in the bonding heights and the positioning of canine and premolar attachments to eliminate the use of mushroom loop archwires.8 Brackets are placed as close as possible to the tooth surface, which reduces the slot-tooth distance, improving 3D control of tooth positions. Mechanics are easier with straight archwires and it is suggested that there is improved patient comfort.

Table 3 outlines the types of cases which are suitable for lingual therapy, and those that are not. The advantages and disadvantages are listed in Table 4. As with any new technique, there is a learning curve associated with switching from labial to lingual appliance therapy. Access and visualization of the working area are reduced and there is a different range of factors to which to adapt.
| Favourable Cases for Lingual13 | Unfavourable Cases for Lingual13 |
|---|---|
|
|
|
| Advantages of Lingual Therapy | Disadvantages of Lingual Therapy |
|---|---|
|
|
Patient factors
Patients do report problems with lingual appliances, including altered speech, tongue soreness, difficulty maintaining oral hygiene and adherence of food between brackets. Lingual brackets alter the morphology of the lingual surface and the second articulation zone, leading to difficulty with speech performance, in particular ‘s’ and ‘t’ sounds. Both patients and speech professionals rate speech as poorer with lingual appliances, with most but not all overcoming speech issues by debond.15,16 This contrasts with labial appliance patients who report some speech alteration initially which recovers within a month. The onset of pain has been found to be earlier with lingual compared to labial appliances.17 There does, unsurprisingly, seem to be a difference in the areas of discomfort between lingual and labial fixed appliances, with tongue soreness and speech difficulties greater in lingual appliances and cheek and lip soreness greater in labial appliances.18 Tongue soreness, a particularly uncomfortable feature, is often graded as severe and can persist until lingual appliance removal.
A significant negative correlation has been established between SNA and SNB angle and the restriction of tongue space with those with SNB less than one deviation below normal values experiencing more severe restriction of the tongue space.19 The newer lingual appliance systems that are custom made to fit an individual lingual tooth surface tend to be able to incorporate a lower profile of bracket. This has been shown to produce fewer tongue restriction problems, speech disturbances and impairments in chewing and biting.20 While much of the published research in lingual orthodontics has concentrated on the bracket mechanics, there has been little assessment of patient factors, although there appears to be increasing interest in the qualitative aspects of this system. Previously, in a patient-based study,21 it was suggested that the lingual technique appealed to a certain patient type, with females accounting for a higher patient uptake (75%), although this is also a widespread finding in labial fixed appliances. Clearly, the aesthetic aspect was the major factor in undertaking treatment with lingual appliances, as 53% of the patients would have refused orthodontic treatment with conventional/ceramic brackets placed labially. The initial irritations were mainly affecting the tongue (65%), but also speech impairment (24%) induced by the lingual appliance. It is generally accepted that placement of a single arch in separate visits rather than bonding of both arches in a single visit assists in patient comfort.22
The ideal malocclusion for lingual appliance treatment is a low angle deep bite case. In addition, Class I or Class II cases with pre-molar extractions are appropriate simple, predictable cases to begin therapy with lingual orthodontics, whereas full pre-molar extractions, posterior crossbites, anterior open bites and increased mandibular plane angle cases are difficult lingual appliance cases.23
Custom-made appliances
New lingual bracket systems are continuously being developed including simpler methods of bonding and ligation methods. Using the latest technology in CAD/CAM processes, Weichmann has produced a system (Incognito) that combines low profile customized brackets with an indirect bonding system.24 This has the advantages of:
Indirect bonding requires excellent technique with adequate moisture control and effective teamwork. The tooth surface should be appropriately prepared for the bonding, with use of a sand blaster followed by the recommended bonding technique. Customized brackets have the advantage of requiring less filler/resin to compensate for the lingual surface and, as a result, have a lower profile bracket. A customized approach also allows straightwire mechanics to be used – especially useful in the buccal segments during space closure. The Incognito system provides a series of archwires, which reduces the need for wire bending, which can be especially difficult in lingual orthodontics.
Non-customized appliances
Lingual appliance brackets have been popularized recently as direct placement non-customized brackets. These have the advantages of being less expensive and can be used for simple alignment of mild crowding cases. Examples include Forestadent Philippe 2D brackets and the STb (Scuzzo/Takemoto) system (Table 1). They can also be prepared for indirect bonding using a transfer jig. As a result of the bracket base being a standard uniform surface, there will be an increase in filler to compensate for the tooth surface and less predictable bonding. There are also the patient factors as discussed previously. These will continue to develop and produce improved non-customized bracket systems and pre-formed archwire sequences.
Case 1 (Figures 2–11)






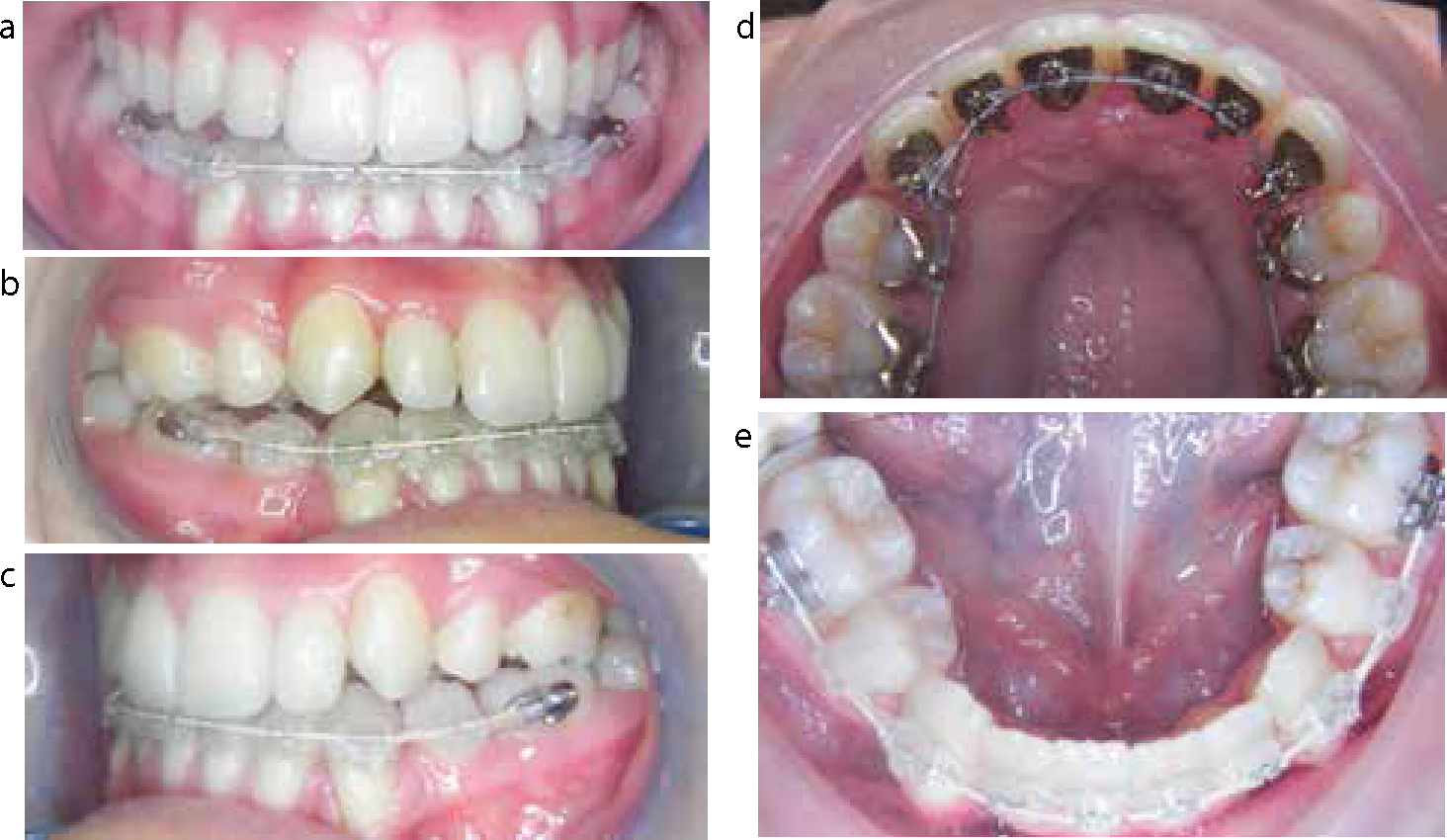

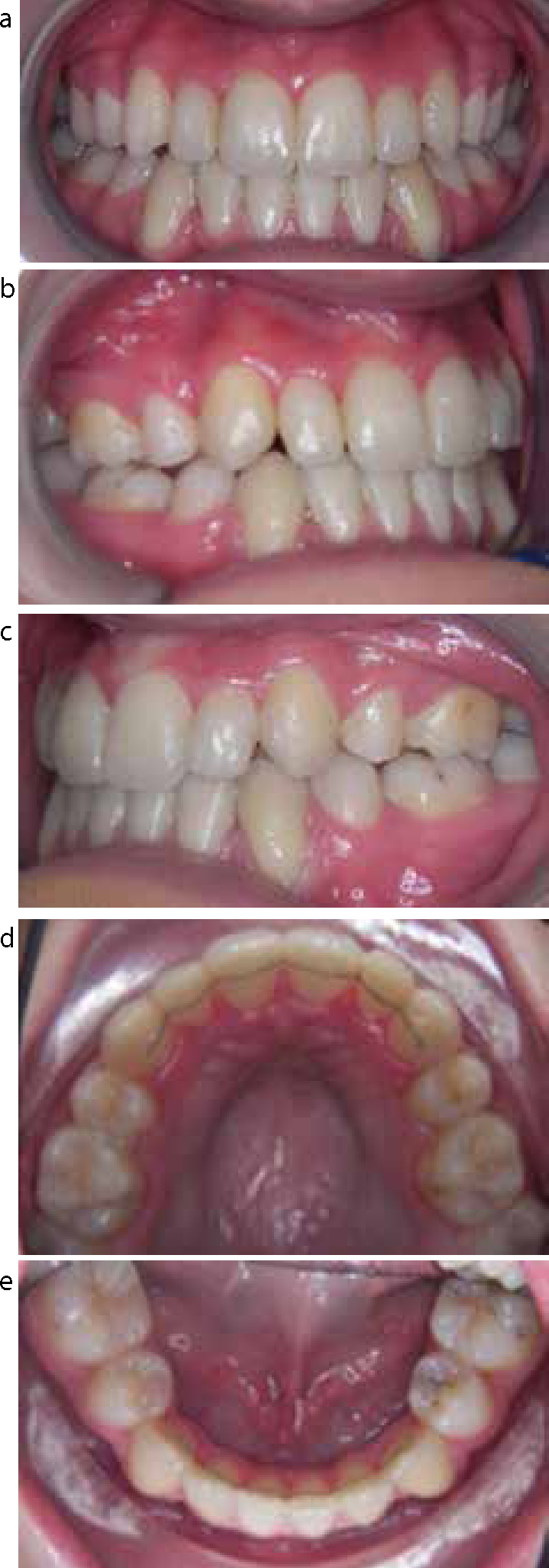
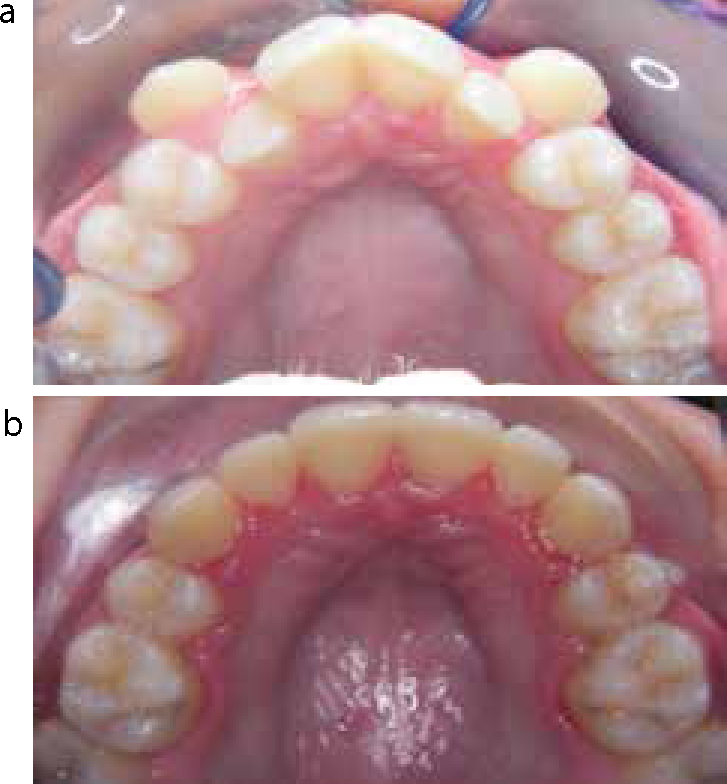
This young adult female was concerned about crowding of her upper and lower teeth. She did not want to wear a conventional upper fixed appliance. Intra-orally she presented with a mild Class III incisor relationship with severe crowding of her upper arch and moderate crowding of the lower arch. In the upper arch, both the upper canines were excluded from the line of the arch and displaced labially. Periodontal health was satisfactory, despite less then desirable hygiene levels.
The aim of treatment was alignment of upper and lower arches with Class 1 incisors and molar relationship. Owing to the severity of crowding in both upper and lower arches, all first premolars were extracted. The treatment plan involved an upper lingual appliance (Incognito, 3M, TOP Service) and lower conventional tooth-coloured fixed appliance. Treatment progressed very well and the labially displaced canines were aligned within seven months. A very successful outcome of treatment was achieved. The patient was fitted with upper and lower fixed bonded retainers from canine to canine. In addition, the patient was given vacuum-formed retainers to be worn on a night-time basis.
Case 2 (Figures 12–19)


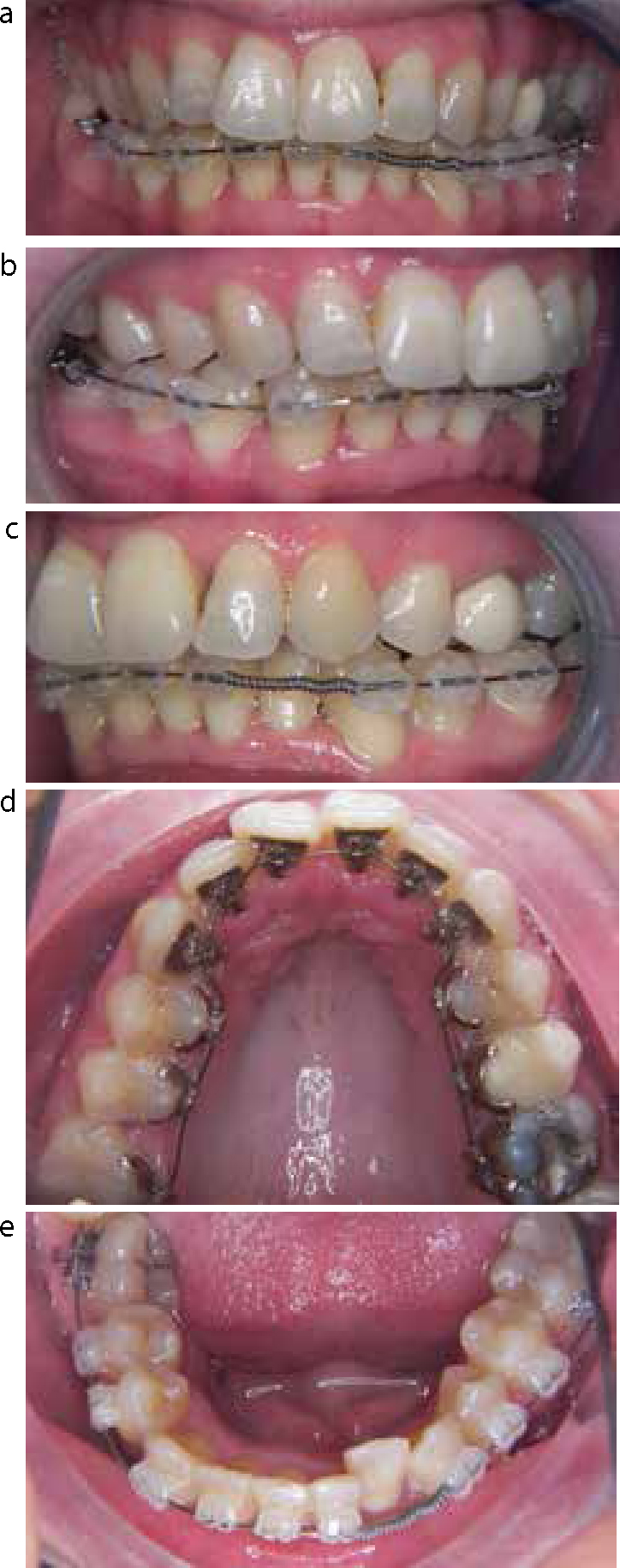
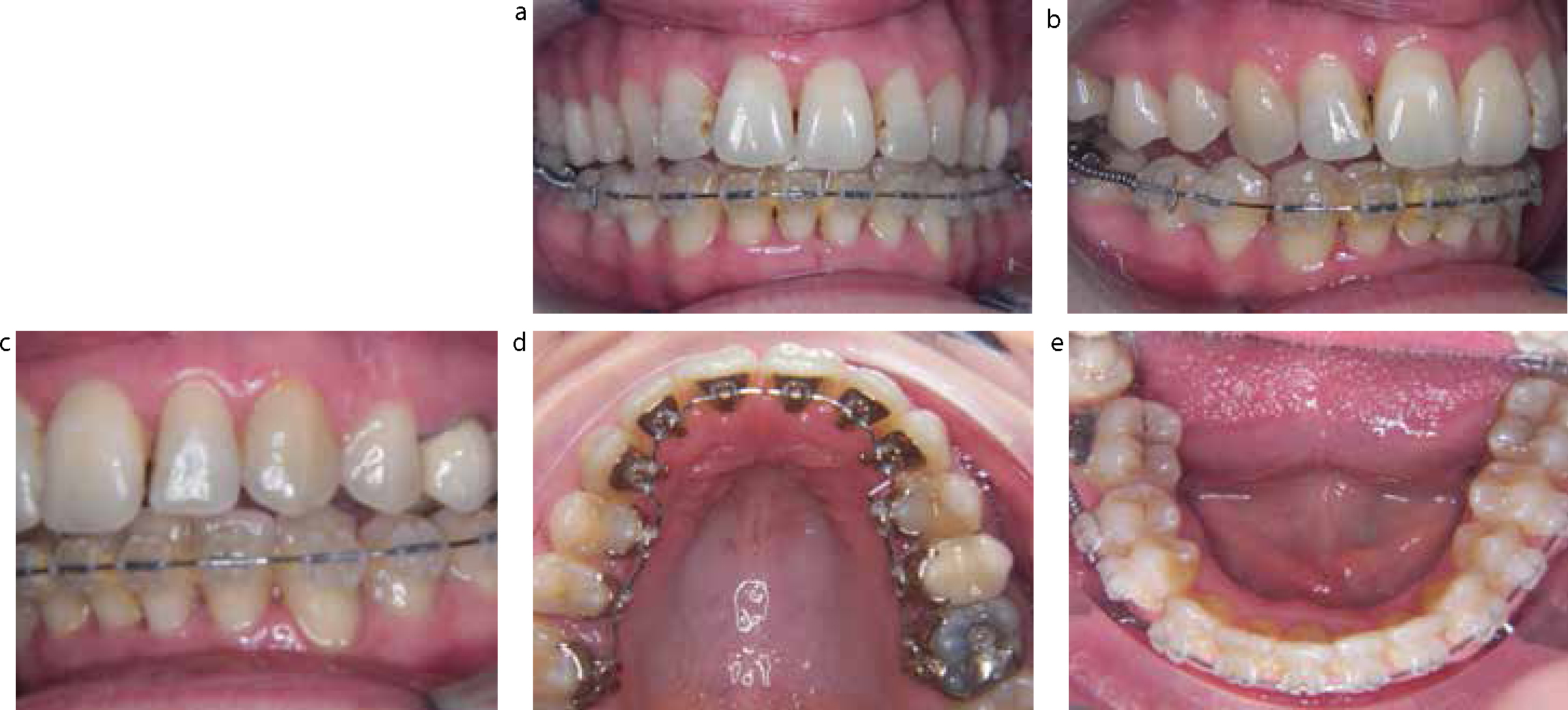




This patient presented with a Class II division 1 incisor relationship. She was very keen to have orthodontic treatment but was not prepared to wear conventional upper labial arch appliances. With the degree of crowding and transverse discrepancy other invisible appliances, such as Invisalign, were not going to be an option. The treatment plan involved lower conventional tooth-coloured appliances and upper lingual appliance. The upper lingual fixed appliance was Incognito (3M, TOP Service) which was custom-made to fit the lingual surfaces of the teeth precisely. Treatment was undertaken on a non-extraction approach and progressed very rapidly. An excellent outcome was achieved within 12 months and upper fixed and removable retainers were fitted.
Conclusion
This article has demonstrated the route of development that lingual orthodontic appliances have taken over the last 30 years. Clearly, improved technology in the construction of the brackets and improved bonding techniques has made the use of the appliance far more user-friendly with predictable results.