Consultant in Orthodontics, University of Manchester Dental Hospital, Higher Cambridge Street, Manchester, M15 6FH, Salford Royal NHS Foundation Trust, Stott Lane, Manchester and Northenden House Orthodontics, Sale Road, Manchester, M23 0DF
In this, the third part of the series, aesthetic orthodontic treatment will be considered. The previous two articles have looked at invisible orthodontics with Invisalign and lingual brackets. This article will discuss the properties and use of aesthetic brackets, along with examples of orthodontic treatment cases using the aesthetic brackets.
Clinical Relevance: Increasing demand for aesthetics during orthodontic treatment has resulted in a significant increase in the use of aesthetic brackets. Clinicians need to be aware of the benefits and drawbacks of aesthetic brackets.
Article
Although fixed appliances have been used for many years, the brackets have been constructed from a metal stainless steel material. Although functionally the metal brackets provide excellent properties with low friction, good resilience to breakage and superior debonding qualities, the appearance of the brackets are anaesthetic. The metal bracket appearance, often referred to as ‘train-track’ braces, are often unappealing to patients, especially adults who may already be conscious of wearing braces. The introduction of aesthetic ceramic brackets in 1986 has allowed many adults to seek orthodontic treatment, reassured in the knowledge that the aesthetic brackets are less visible and more socially acceptable (Figure 1).
Figure 1. A patient with upper and lower ceramic aesthetic brackets. Tooth-coloured wires have been used to maximize the aesthetic appearance and invisibility.
Evolution of aesthetic brackets
The majority of aesthetic brackets are ceramic, composed from an aluminium oxide material. Originally, plastic brackets constructed from acrylic and later polycarbonate were introduced to improve the aesthetics of fixed appliances.1 Problems with rigidity, strength and staining led to further development, including reinforcing the polycarbonate with ceramic. These brackets demonstrated improved mechanical properties but still maintained torque control problems. Full ceramic brackets, using aluminium oxide in various forms, provided a major improvement in aesthetic brackets, with improved strength resistance to wear and overall aesthetic appearance. A number of manufacturers now produce aesthetic ceramic brackets, each implying an advantage often relating to mechanical or improved aesthetic properties (Table 1).
Bracket Name (Manufacturer)
Features of Bracket System
Debonding Technique
Monocrystalline Ceramic Brackets
Inspire ICE (Ormco)
Improved breakage resistance and torque strengthHeat polished smooth surface to decrease frictionBall-base technology for easy debondingTooth-specific pad contours
Ultra smooth with low friction sliding mechanicsCuspid brackets available with hooks
Flash removal then apply bracket removers under pad
Radiance (American Orthodontics)
Patented Quad-Matte base - strong bond in centre for retention but weaker on outside for easy debondEnlarged under tie-wing space for ease of ligation
No special extra tools required for debond
Spa Aesthetics (DB Ortho)
Accurate base contour for reliable fitOptimum slot design to decrease frictionExcellent tie-wing area
SPA direct bond remover
Polycrystalline Ceramic Brackets
Contour (DB Ortho)
Base has surface comparable to mesh base on steel bracket
Flash removal then DB Band Slitter applied
Intrigue Silk (OrthoCare)
Pseudo-twin design increases strengthSilk cleat holds adhesive within bracket base rather than on tooth surface - debonding easier
Stealth debonding instrument recommended
InVu (TP Ortho)
Exclusive colour matching technology so bracket blends with individual teethCompound contoured baseWedge-shaped lower anterior brackets to minimize interferences and wearMoulded polymer mesh base which flexes during debond retaining most of adhesive
No special extra tools required
Tip-Edge Plus Ceramic (TP Ortho)
Aesthetic version of Tip-Edge Plus - horizontal tunnel permits uprighting and torquing from superelastic auxiliary archwire
No special extra tools required
20/40 (American Orthodontics)
Reduced particle size - smaller more rounded bracket and slot cornersBevelled lower anterior brackets to decrease wear and interferences
No special extra tools required
Polycrystalline Ceramic Brackets with Metal Slot
Clarity (3M Unitek)
Metal-lined archwire slot - no metal-ceramic frictionMechanical lock baseEasy debonding due to vertical debonding slot (bracket collapses) and stress concentrator on base of bracket
No special extra tools required
Desire (Orthocare)
Gold slot to decrease frictional resistanceSmaller more compact bracket with mechanical locking baseTorque in base and individual customization available
No special extra tools required
Virage (American Orthodontics)
Gold alloy slot insert (100% nickel free) for enhanced slidingMechanical lock base with dovetail grooves
No special extra tools required
Polycrystalline Ceramic Self-Ligating Brackets
Damon clear (Ormco)
Passive self-ligation system with SpinTek slide for fast and comfortable archwire changesCustomized base design with laser-etched pad
Damon Clear DebonderNo flash removal required
Clarity SL (3M Unitek)
Combines SmartClip technology with a ceramic bracket
Remove flash then use Unitek Self-Ligating Bracket Debonder
Properties of aesthetic brackets
Hardness
Aluminium oxide has an extremely high hardness property,2 nine times harder than stainless steel or enamel.3 This can be a desirable property in that ceramic brackets can resist damage from patient trauma or during orthodontic adjustments, but may be considered as a disadvantage if they come in contact with enamel from an opposing tooth. Indeed, a major concern is enamel abrasion that can occur when occlusal contact is made from a ceramic bracket.
Strength
The tensile strength of aesthetic ceramic brackets is higher than stainless steel,4 which will reduce or resist structural failure. This strength, however, also causes the ceramic to be more brittle1 and this can lead to a higher bracket breakage clinically.
Orthodontic bonding
Early aesthetic ceramic brackets, chemically bonded using a silane-coupling agent, demonstrated extremely high bond strengths that could cause enamel damage during debonding procedures. The initial challenge was to reduce this to a level that had sufficient bond strength to allow orthodontic mechanics but could be debonded safely with no enamel damage.5 Studies have assessed various chemical and mechanical bond techniques and suggest that the use of a mechanical interlock reduces enamel detachment but still maintains high strength, durability and retention similar to metal brackets.6
Friction
Ceramic brackets tend to have a rougher surface than stainless steel7 and this inevitably produces a greater coefficient of friction. In simulated clinical conditions, conventional ceramic brackets generated significantly higher friction than other brackets tested.8 Manufacturers have attempted to address this by placement of a metal slot in the bracket to allow improved sliding of archwires. Although the overall appearance of the bracket remains aesthetic, particularly image conscious patients may still be concerned with the appearance of the metal slot. A lab-based study,9 however, failed to demonstrate improved properties in resistance to sliding following the insertion of a metal slot.
Frictional resistance properties have been of major consideration in orthodontics over the last decade, with an increased interest in self-ligating brackets. These are considered to have optimal frictional properties and this has led to the introduction of ceramic self-ligating brackets (Figures 2 and 3). These usually contain a metal gate that can be dulled to improve the appearance. Of course, the need for maximum resistance to frictional forces is debatable, as many adult treatments are undertaken on a non-extraction basis that do not require large sliding mechanical movements suited to low friction brackets.
Figure 2. The Clarity Self-ligating aesthetic bracket incorporating a smart-clip to position the wire.Figure 3. Self-ligating Aesthetic ‘Innovation’ bracket (GAC). The bracket base is ceramic with a metal facing clip.
Clinical use of aesthetic brackets
Although most orthodontists would favour the use of stainless steel brackets10 for reasons expressed above, the use of aesthetic brackets can be used in most clinical cases. Table 2 lists the ideal case for the use of aesthetic brackets. Their use tends to be restricted to adults who are seeking private orthodontic treatment, although there is no reason for not using on adolescents and children. Adult patients should be counselled that, although the brackets may be tooth-coloured, the elastics that hold the archwire in place could often stain during treatment, even though these are routinely replaced. Initially, orthodontists may place tooth-coloured archwires, which also provide an excellent aesthetic appearance, but usually a metal-appearance archwire is needed at the later stages of treatment.
Adults
Minimal occlusal contact between bracket and opposing tooth
Non-extraction cases
Good oral hygiene
Low restorative experience
If oral hygiene is suspect, it may be preferable to consider metal brackets as much as possible in areas such as premolars and the lower arch, which make the detection and accumulation of plaque much more visible for cleaning.
Once the aesthetic brackets have been placed, a close inspection of the occlusion should be made. Any potential occlusal contact with the ceramic brackets should be identified and may require the placement of a bite-opening filling material placed on the posterior occlusal surfaces.
Bonding of aesthetic brackets
Owing to the high bond strength generally achieved with ceramic brackets, initial preparation of the tooth is straightforward. Cleaning with a pumice agent should be used to remove any surface debris and the enamel can be etched with a conventional system or using a self-etching primer. Normal curing techniques can be applied and reliable bond strengths can be routinely obtained. Bracket placement is more difficult than stainless steel brackets owing to the tooth-coloured appearance and less obvious bracket edges that act as a positional guide.
Debonding of aesthetic brackets
As discussed above, the aesthetic brackets can attain high bond strength and this can pose a particular difficulty in debonding. Previous suggested techniques have involved initial removal of excess flash around the bracket, ultra-sonic scaling and use of debonding agents. More recently, manufacturers have designed specific techniques for predictable debonding, such as the insertion of a ‘stress concentrator’ that fractures during mesio-distal squeezing (3M Clarity™).
The failure of the bracket/adhesive interface leaves residual adhesive on the tooth surface, which necessitates a longer clean-up procedure but reduces enamel detachment.
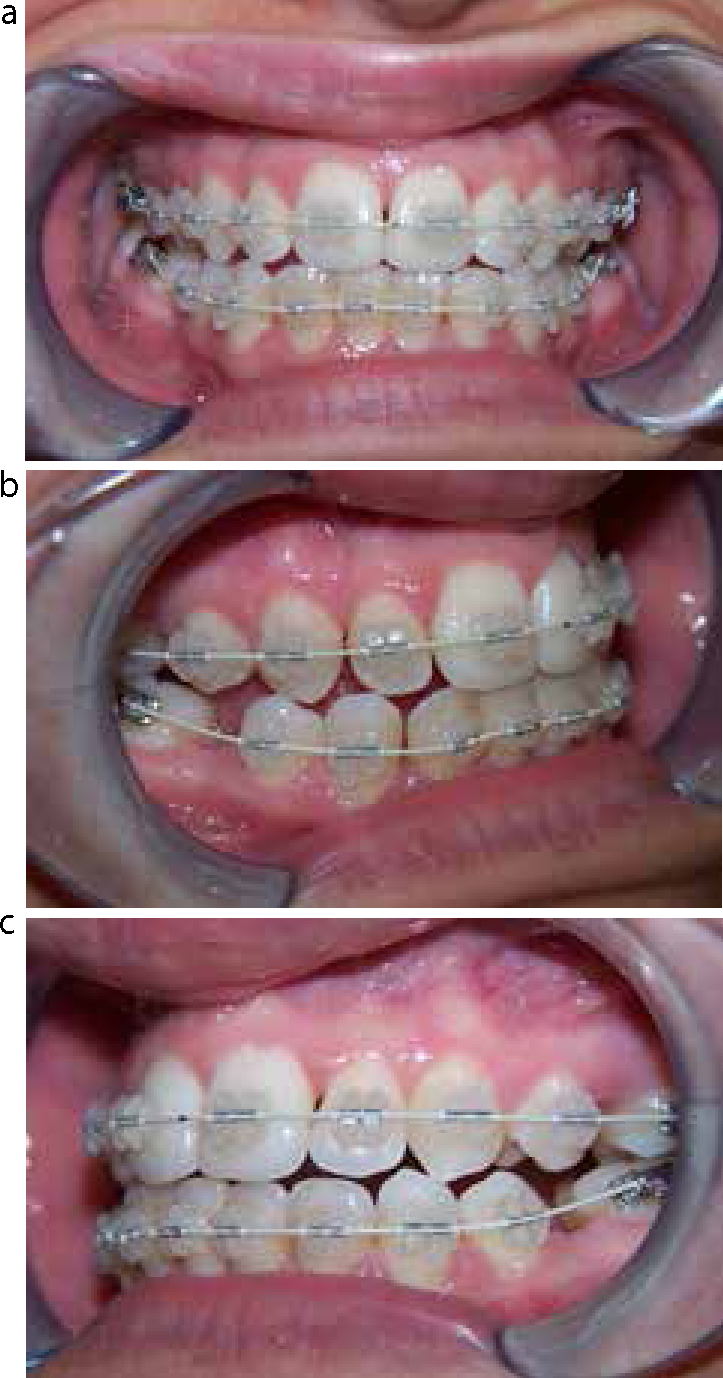
This 21-year-old patient attended with a Class III incisor relationship on a mild Class III skeletal pattern. The upper and lower arches were both severely crowded with a reverse overjet, displaced upper lateral incisors and anterior open bite (Figure 4). The patient was only prepared to wear aesthetic brackets because of her occupation, which involved contact with the public.
Figure 4.
(a–e) Pre-treatment views prior to placement of appliances (ClarityTM 3M).
A treatment plan was formulated which involved removal of four premolar teeth and camouflage of the malocclusion to finish with a Class I molar and incisor relationship.
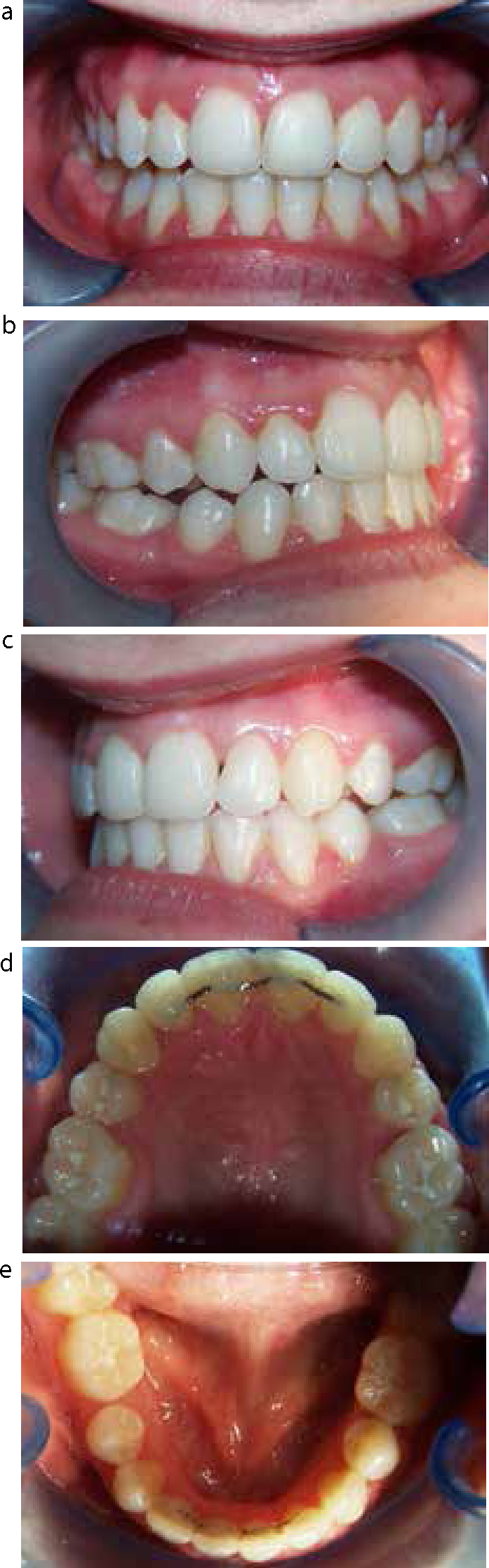
The case progressed well with placement of the upper arch initially with the lower arch bonded later and maintained in round stainless steel archwires (Figure 5). Space closure progressed rapidly and an overall good aesthetic result was obtained (Figure 6).
Figure 5.
(a–c) Mid-treatment views with the aesthetic brackets in place.Figure 6.
(a–e) Post-treatment views following treatment with aesthetic brackets.
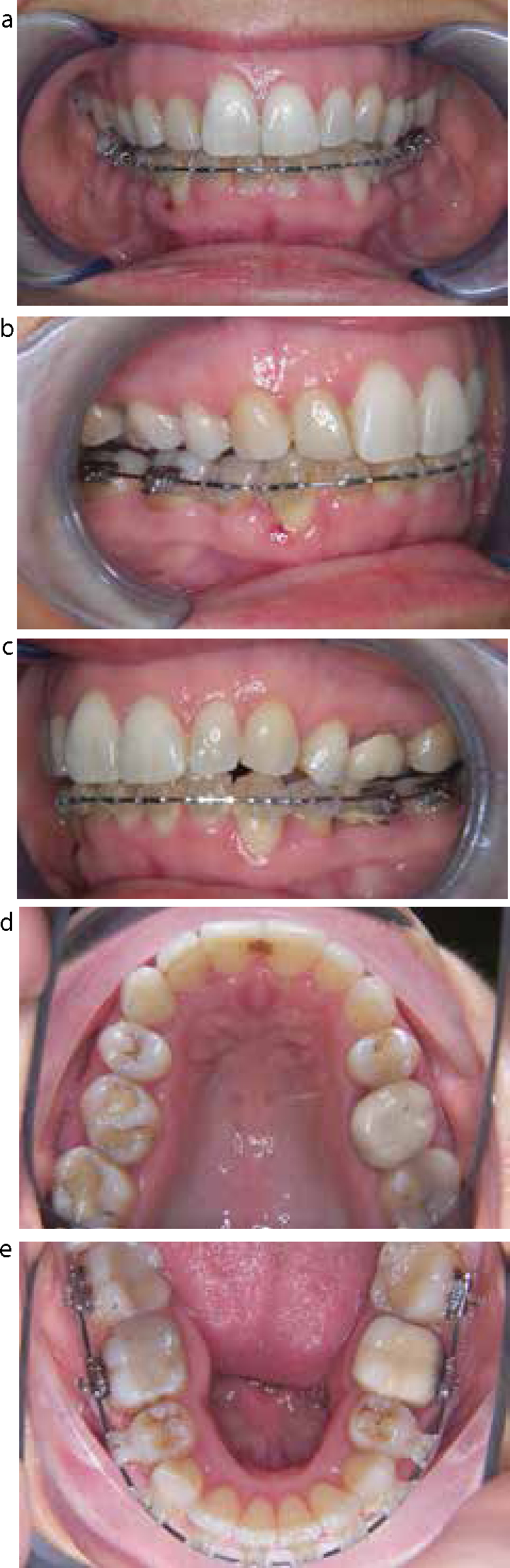
A 42-year-old lady presented with a Class II division I incisor relationship on a skeletal 1 base complicated by grossly lingually-tipped lower premolars (Figure 7). The patient had previously sought orthodontic treatment but was informed that no orthodontic treatment could correct her malocclusion. A fixed ceramic appliance was placed on the lower teeth and space created to allow uprighting of the tipped premolars (Figure 8).
Figure 7.
(a–e) Pre-treatment intra-oral views of Case 2.Figure 8.
(a-e) Mid–treatment views to show lower aesthetic brackets, aligning the displaced lower premolars.
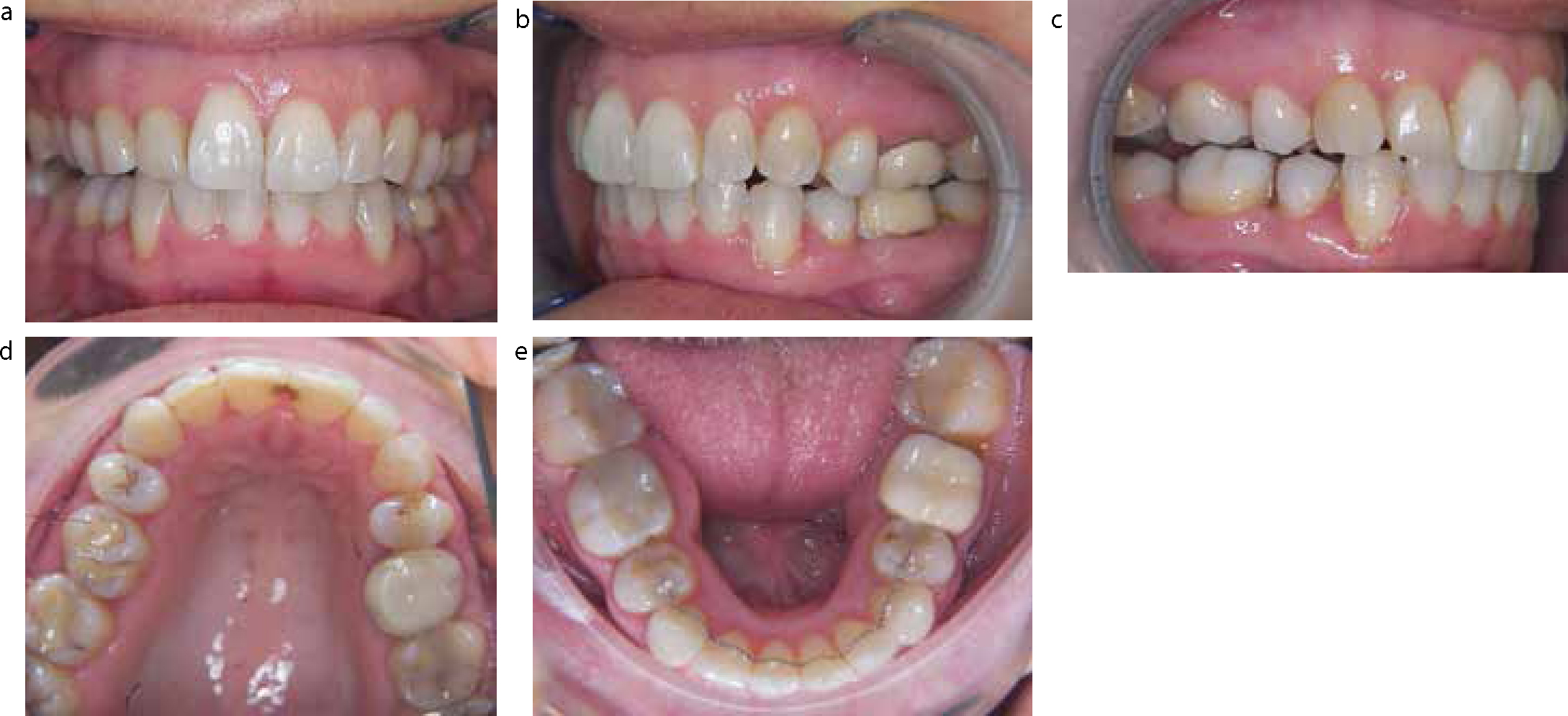
The fixed appliance stage progressed uneventfully and space was created to align the premolars. A bonded retainer (Manchester positioner) was placed along with a removable night-time retainer. The bonded retainer was extended to include the occlusal surfaces of the premolars (Figure 9).
Figure 9.
(a–e) Post-treatment views. The premolars have been uprighted and a bonded retainer fitted with a removable Essix retainer.
Conclusion
Aesthetic brackets have allowed a significant number of patients to undertake orthodontic treatment that would otherwise have been unable to do so. The appearance of the appliances is acceptable and mechanical properties have improved to ensure treatment goals can be achieved. The brackets clearly have some limitations and manufacturing research and development will continue in the pursuit of the ideal aesthetic bracket.