Hiro T, Takemoto K. Resin core indirect bonding system – improvements of lingual orthodontic treatment. J Jap Orthod Soc. 1998; 57:83-91
Wiechmann D, Rummel V, Thalheim A, Simon JS, Wiechmann L. Customized brackets and archwires for lingual orthodontic treatment. Am J Orthod Dentofacial Orthop. 2003; 124:593-599
Sinclair PM, Cannito MF, Goates LJ, Solomos LF, Alexander CM. Patient responses to lingual appliances. J Clin Orthod. 1986; 20:396-404
Gorman JC, Hilgers JJ, Smith JR. Lingual orthodontics: a status report. J Clin Orthod. 1983; 17:26-35
Årtun J. A post treatment evaluation of multibonded lingual appliances in orthodontics. Eur J Orthod. 1987; 9:204-210
Gorman JC. Treatment of adults with lingual orthodontic appliances. Dent Clin North Am. 1988; 32:589-620
Chaushu S, Becker A, Chaushu G. Lingual orthodontic treatment and absolute anchorage to correct an impacted maxillary canine in an adult. Am J Orthod Dentofacial Orthop. 2008; 134:811-819
Wiechmann D, Schwestka-Polly R, Hohoff A. Herbst appliance in lingual orthodontics. Am J Orthod Dentofacial Orthop. 2008; 134:439-446
Hong RK, Lee JG, Sunwoo J, Lim SM. Lingual orthodontics combined with orthognathic surgery in a skeletal class III patient. J Clin Orthod. 2000; 34:403-408
Smith JR, Gorman JC, Kurz C, Dunn RM. Key success in lingual therapy. Part 1. J Clin Orthod. 1986; 20:252-261
Caniklioglu C, Öztürk Y. Patient discomfort: a comparison between lingual and labial fixed appliances. Angle Orthod. 2004; 75:86-91
Hohoff A, Stamm T, Goder G, Sauerland CM, Ehmer U, Seifert E. Comparison of 3 bonded lingual appliances by auditive analysis and subjective assessment. Am J Orthod Dentofacial Orthop. 2003; 124:737-745
Stamm T, Hohoff A, Ehmer U. A subjective comparison of two lingual bracket systems. Eur J Orthod. 2005; 27:420-426
Wiechmann D, Stamm T, Hohoff A. Prediction of oral discomfort and dysfunction in lingual orthodontics: a preliminary report. Am J Orthod Dentofacial Orthop. 2008; 133:359-364
Ling PH. Lingual orthodontics: history, misconceptions and clarification. J Can Dent Assoc. 2005; 71:99-102
Rosvall MD, Fields HW, Ziuchkovski J, Rosenstiel SF, Johnston WM. Attractiveness, acceptability, and value of orthodontic appliances. Am J Orthod Dentofacial Orthop. 2009; 135
As adults increasingly seek orthodontic treatment, a growth has been witnessed in the demand for aesthetic orthodontics, the ultimate of which are appliances bonded to the lingual surfaces of the teeth. Development has spanned 30 years and many of the initial challenges faced with this approach have now been overcome. An overview is provided on the development of lingual appliances from conception through to the current systems available. Lingual orthodontics is not for every patient seeking treatment and therefore the indications and contra-indications are discussed, together with the advantages and disadvantages of this increasingly popular approach.
Clinical Relevance: Patients are increasingly asking dental professional about lingual appliances.
Article
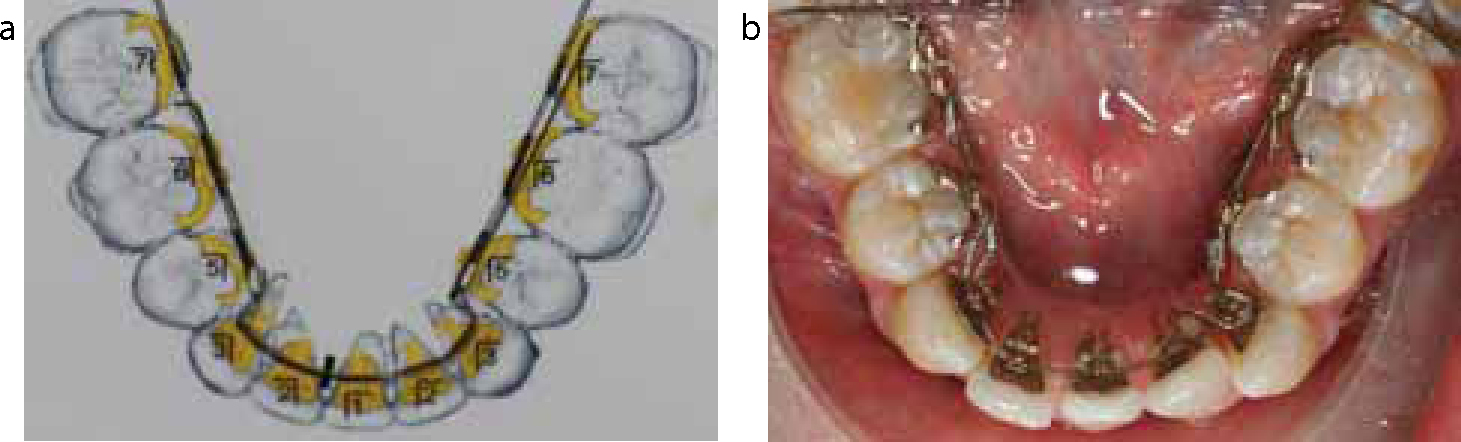
Most orthodontists would report that, in recent years, there has been a marked increase in the number of adults, particularly females,1 seeking orthodontic treatment. Tooth-coloured brackets have become widely available in response to the patient's desire for discreet treatment. Although plastic and porcelain brackets reduce the visual presence of the appliance, they are nevertheless still visible and this remains a problem for some patients. Other systems, such as Invisalign (Align Technology Inc, San Jose, USA), have been promoted as effective alternatives. However, their moderate aesthetic appeal and clinical limitations are well documented.2 Lingual appliances are unique in this respect as they provide the ultimate in aesthetics by attachment to the lingual surface of the teeth (Figure 1).
Figure 1.
(a) Lingual appliances provide the ultimate in aesthetics being hidden on the lingual surfaces of the teeth. (b) The same patient from the palatal aspect showing the Incognito system.
This article reviews the development and challenges of lingual appliances, the clinical procedure, treatment considerations, as well as the advantages and disadvantages of lingual appliances. It will provide readers with information that they can pass on to their patients who may be seeking an orthodontic referral for lingual appliances.
Development
Once bonding to enamel became established, several orthodontists, working independently in different parts of the world, experimented with the possibility of a fixed lingual appliance.
Kurz began experimenting with labial brackets bonded to the lingual surface of the mandibular teeth in 1973. He limited his treatment to the mandibular arch, fearing that the forces of occlusion would dislodge any brackets placed on the lingual surface of the maxillary anterior teeth. In 1979, he patented a lingual edgewise appliance incorporating a bite plane on the maxillary anterior teeth, mesh bonding pads to adapt to the lingual surface of the teeth and pre-torqued archwire slots.3
At around the same time, Fujita described a new lingual appliance and a mushroom archwire designed to compensate for the difference in labio-lingual thickness of the anterior and posterior teeth.4 This was seen as a breakthrough in aesthetic orthodontics. However, although many patients started with this new system, fewer completed treatment with lingual appliances alone. Many orthodontists, unable to straighten the teeth adequately, were spending 2 to 3 years trying to finish cases. They were forced to remove the appliances and replaced them with conventional labial appliances. They concluded that lingual appliances were unable to finish treatment satisfactorily. Faith in the lingual appliance faded and the initial excitement dampened.5 However, those using these early systems often lacked sufficient training6 and were using appliances that were in the infancy of their development.7 Consequently, aesthetic labial brackets gained popularity; although they were not invisible they were much easier to use.
The most popular lingual system in the following years was the Ormco 7th generation bracket (Ormco Corporation, Orange, USA) with varying degrees of torque, tip and thickness. The laboratory process required an individualization of the base of the bracket with a wedge of resin being added. This placed the bracket further from the tooth and increased the tendency for tongue irritation.
Challenges
The anatomical variations and the difficulty of direct vision and access to the lingual surface of the teeth make lingual orthodontics challenging. The lingual surface of the teeth has a unique morphology, especially on the maxillary anterior teeth, that makes it difficult to place brackets in ideal positions.
Other reasons why orthodontists have been hesitant to use lingual appliances include the wide range of bucco-lingual thickness of the teeth necessitating numerous in-out bends and much smaller inter-bracket distances in the anterior region, making compensatory bends difficult.
Despite little teaching in lingual orthodontics, users are more likely to be those who recently completed their formal orthodontic training8 and, previously, a global pattern has been reported with more users in Europe and Japan than the United States.6,9
Current systems
Many of these challenges have been overcome, or at least reduced, with several of the current systems available. A concise review of the positioning techniques is provided by Ye and Kula.9
The Custom Lingual Appliance Setup Service (CLASS) was developed by Ormco and requires accurate articulated stone casts.10 The original malocclusion model is sectioned and the teeth arranged in wax to an ideal occlusion. Template blades are used to position the brackets with all the slots parallel to the occlusal plane.
A surveying instrument, the Torque Angulation Reference Guide (TARG), developed by Ormco and subsequently modified by Fillion, can be used to transfer the lingual bracket position from the labial surface of the teeth.11 The latter modification has allowed bonding material to be used to normalize the differing thicknesses of the anterior and posterior teeth.
Ormco's current system, STb Light Lingual System, was developed in association with Giuseppe Scuzzo and Kyoto Takemoto. It reduces the reliance on CLASS and TARG, using a custom composite material which helps ensure an accurate fit on the lingual surface of the tooth (Figure 2).
Figure 2. One of the lingual systems available, STb by Ormco is shown. Courtesy of Paul Ward.
In the Hiro system from Japan,12 the brackets are positioned on a set-up model using an ideal archwire and then transferred to the mouth using an individual mini-tray for each tooth.
There are several other brands of pre-formed lingual brackets on the market, such as Stealth by American Orthodontics (Sheboygan, USA), Forestadent (Pforzheim, Germany) with 2D Torque Lingual Brackets, Magic by Dentaurum Group (Ispringen, Germany) and In-Ovation L and MTM by GAC (Dentsply GAC International, Bohemia, USA). Some of these are manufactured for direct bonding, although many may be bonded indirectly using laboratory procedures, such as the Hiro system. In-Ovation MTM is marketed for correcting minor misalignment (for the anterior ‘social six’ teeth) using only round wires with no more than one or two wire changes!
Computer-aided design/computer-aided manufacturing (CAD/CAM) technology is used in the production of Incognito (3M Unitek Corporation, Monrovia, USA) brackets. After silicone impressions are cast (Figure 3), a set-up is performed and a 3-dimensional optical scan is taken. The digitized set-up plaster casts (Figure 4) are used virtually to construct each lingual bracket on its corresponding digital lingual tooth surface. A method called Transfer Optimized Positioning (TOP System, Top Service, Bad Essen, Germany) is used for positioning of the lingual brackets in the scanned model; these are then manufactured later using wax analogues and then converted into a high gold content alloy.13 The individualized brackets are bonded on the models of the initial malocclusion where the transfer tray is made. Figure 5 shows a transfer tray with the brackets in place. Either a ribbonwise vertical slot or a horizontal Edgewise slot can be requested. The geometry of the archwires is calculated with the CAD/CAM software and transferred to a wire bending robot which applies prescribed bends and torques as shown in Figure 6a. The same archwire is shown in Figure 6b ligated in the appliance. All archwires in the sequence of treatment have the same geometry to obtain the final position of the teeth in the set-up. This system, owing to the accurate fit of the bracket to the palatal surface, has the added benefit of easily relocating on the tooth should it debond, obviating the need for a transfer tray for re-bonding (Figure 7).
Figure 3. An impression for lingual appliance construction. Heavy and light-bodied silicone impression material has been used.Figure 4. A 3D digitized plaster cast with brackets added used in the manufacture of Incognito brackets.Figure 5. A transfer tray is used to locate the brackets in the correct position for bonding. The bonding surface of the brackets appears matt. In this case, a chemically cured composite adhesive is used because the tray is not transparent.Figure 6.
(a) Archwires can be customized using a wire bending robot which applies prescribed bends and torques. (b) The same archwire inserted into the appliance. Note that, although the wire is irregular, the teeth are almost aligned.Figure 7.
Incognito bracket system with large bracket bases to allow easy relocation should the bracket debond.
Clinical procedure
It is essential that the impressions be as accurate as possible, which is why a material such as a silicone should be used. A two-phase silicone impression is preferred13 which is sent to the laboratory for the set-up procedure to be completed.
In lingual orthodontics the following can all contribute to inaccurate bracket placement:
Limited access and visibility;
Greater variation in lingual surface morphology;
Shorter lingual crown height;
A wide range of labio-lingual crown thicknesses;
Sloped lingual surfaces;
Smaller inter-bracket distance; and
Tongue interferences.
Indirect bonding is therefore the standard in lingual orthodontics. This is usually carried out with a 2-phase silicone bonding tray with an inner softer silicone and an outer extremely hard silicone,13 which is returned from the laboratory carrying the brackets.
A dry field is imperative to achieve good results in indirect bonding and the lingual surface should be thoroughly cleaned using either pumice or a micro-etcher.6 The teeth are then etched and washed and dried. Adhesive resin is applied to the etched tooth surface and adhesive is coated on the bracket bases which are held within the silicone tray. Once the tray is in place, sufficient time should be allowed to pass to ensure the composite adhesive is sufficiently set. Increasingly, chemically cured adhesives are being used and it is recommended to remove the transfer tray carefully. This allows for the removal of any excess, particularly in the inter-proximal areas where dental floss can be passed down into the contact points.
Archwires are usually provided by the laboratory and a range of lingual instruments such as lingual Weingart pliers, lingual arch bending pliers and lingual debonding pliers are now available from a range of suppliers. Once the archwire is in place, elastic modules, chain or steel ligatures are used to ligate wire, although there is an increasing supply of self-ligation lingual bracket systems.
The bracket slot size is often 0.018” x 0.025”, although with some systems this can be customized during the manufacturing process (3M Unitek Corporation, St Paul, USA). A typical archwire sequence will be as follows: 0.016” copper nickel titanium wire (CuNiti), 0.016” x 0.022” CuNiti, 0.016” x 0.022” stainless steel wire, 0.0182” x 0.0182” titanium molybdenum alloy (TMA). Figures 8a and 8b show a case treated with lingual appliances and the changes that occurred after three visits.
Figure 8.
(a) A case treated with upper and lower lingual appliances shown at the fitting appointment. (b) The same case, three visits later.
Patient information
Patient education should focus on problems that are most likely to occur after appliance placement: tongue irritation, masticatory problems and speech difficulty. Sounds such as ‘s’ and ‘z’ will be hard to communicate clearly for the first few days.14
Placement of lingual appliances in one arch at a time with an interval of two months has been recommended to allow the patient to adjust to the brackets.1 Adaptation tends to be longer for the lower arch, with tongue irritation disappearing in most patients within 2 to 3 weeks.1,14
Periodontal dressings, thermoformed silicone sports guards, wax products and composite restorative materials have all been used, to varying success, to reduce the discomfort of lingual appliances. Customized silicone material which is provided in a tube and mixed by the patient has also been recently introduced for reducing discomfort (Gishy Goo, Opal Orthodontics Limited, South Jordan, USA).
Patients should be prepared for lengthy appointments, particularly if the clinician is inexperienced15 and the mean chairside time for an archwire change can be just under an hour.16
Treatment considerations
The position of the lingual brackets places the slots closer to the centre of resistance of the teeth. Theoretically, this result in reduced undesired tooth movements and more predictable bodily movements during space closure and bite-opening, since the applied force is closer to the centre of resistance.
As the mandibular incisors contact the bite plane on the maxillary brackets, a bite opening effect is seen with the disclusion of the posterior teeth. The mandible rotates clockwise, the overjet increases and a Class II malocclusion is made more severe. It is often desirable to remove the maxillary first premolars in Class II cases to aid overjet reduction and allow mesial molar migration.17
The lingual appliance is equally effective at treating four premolar extraction cases and those requiring arch expansion.17 Class I patients with a deep overbite are ideal for lingual appliance treatment. When used properly, the bite plane effect can be advantageous not only for correcting deep bites but also crossbites, rotations and enabling space closure without the interference of the occlusion.
The versatility of the lingual appliance has been demonstrated in its use in combination with temporary anchorage devices for aligning ectopic canines in adults18 and functional appliance treatment has even been made possible with the attachment of Herbst telescopic mechanisms via custom-made labial pivot bases.19
Previously, lingual appliances were considered ill-suited for surgical orthodontics because of the challenges for stabilizing the jaws at the time of surgery. This can be overcome, in part by metal lingual buttons being temporarily placed on the labial surfaces of the teeth (Figure 9) for inter-maxillary fixation20 or with the use of temporary anchorage devices placed in maxilla and mandible.
Figure 9. Metal lingual buttons have been placed on the labial surfaces of the teeth which can be used for inter-maxillary elastics or inter-maxillary fixation. Courtesy of Paul Ward.
Patient selection
Lingual appliances differ enough from labial appliances to require a different approach to case selection and treatment planning.5,21 One contra-indication has been cited as those patients with significant open bites17 since lingual appliances have a bite opening effect. Those with a high maxillary-mandibular planes angle may prove challenging and clinicians may want to think carefully about treatment mechanics.
Individuals with partially erupted teeth pose a challenge and it is best to wait until full eruption has occurred. Lingual crown heights on the average patient are 30% shorter than the available crown on the labial surface.15 A minimum height of 7 mm of clinical crown makes lingual appliances unsuitable for those with short clinical crowns.
Those with low pain thresholds should be encouraged to accept labial appliances, with one author finding one-third of patients seeking invisible braces choosing to have labial appliances after the pros and cons are explained.15
Advantages
The ultimate in aesthetic appliances: not only are lingual appliances discreet, but the labial surfaces of the teeth are not damaged from bonding, debonding, adhesive removal or decalcifications. The labial gingival tissues are also not adversely affected, although it must be remembered that the lingual surfaces are not immune to these detrimental effects!
The position of the teeth can be seen more precisely when their surfaces are not obstructed by the brackets and archwires of conventional labial appliances. Facial contours are visualized better as the drape of the lips is not distorted by the labial appliances.
We have already mentioned that lingual appliances are effective for correcting deep anterior bites with intrusion of the anterior teeth and extrusion of the posterior teeth. Another advantage is seen in anterior crossbite cases where bracket loss is reduced.
Vectors of orthodontic forces applied to lingual brackets pass lingually to the centres of rotation of the teeth, which increases lingual crown torque on the anterior teeth and forces the posterior teeth into an upright position. Vertical anchorage is reinforced as the molars tip lingually to create buccal root torque, establishing cortical bone anchorage. In the horizontal dimension, anchorage is also preserved because the force is applied lingual to the centres of rotation of the teeth and the posterior teeth rotate distally.
Disadvantages
Tongue discomfort, speech problems and masticatory difficulties remain significant drawbacks of the lingual appliance systems, with tongue discomfort persisting for more than three months for some patients.22 Customized lower-profile lingual brackets have been shown to enhance patient comfort significantly and also significantly reduce impairments of good speech performance compared with prefabricated brackets with larger dimensions.23,24 Lower SNA and SNB angles have been shown to be predictors for the level of tongue space restriction after placement of lingual brackets and may serve as a guide to identifying patients that may have increased problems with adaptation.25
The anterior bite plane effect can make mastication quite difficult at first, with the mandibular incisor edges biting on the maxillary anterior brackets. This usually resolves after one to three months, depending on the severity of the deep bite and crowding. Taste function may also be reduced for the first few months and weight loss in the first few weeks often occurs.1
Since most of the discomfort, speech and masticatory problems are associated with the mandibular lingual appliance, and most individuals display mainly the maxillary teeth when smiling, it is possible to provide a combination of maxillary lingual appliances and mandibular labial appliances.26 This also has the added advantage of reduced patient fees, however, an additional challenge is posed with inter-arch mechanics, since the appliance will be on the palatal surface of the maxillary teeth and the labial surface of the mandibular teeth.
Access for cleaning on the lingual surface can be difficult, so patients must not only be highly motivated, but should also be instructed to use a lingual ‘scrub’ technique.14 Despite the advantage of not damaging the labial surfaces of the teeth, lingual appliances can still be detrimental to the dental tissues, causing white spot lesions and gingival swelling and bleeding.16
Patients should be prepared to spend significantly greater time in the chair for adjustment appointments,15 since access to and visualization of the lingual surfaces of the teeth is difficult. Interestingly, there is little objective evidence to suggest that lingual appliance treatment takes longer than a similar case using conventional labial appliances.26 Postural challenges associated with potential back pain and related discomfort may discourage some operators.26
Mandibular rotation because of the bite plane effect and its detriment to the Class II cases has been mentioned. Inter-bracket distances are reduced with lingual appliances which can hinder full bracket engagement of the anterior teeth and make initial alignment difficult.
During canine retraction with the lingual technique, vertical bowing can result from lingual tipping of the incisors and mesial tipping of the molars. Transverse bowing can also occur from rotation of the canine and buccal displacement of the premolars. To reduce the vertical and transverse bowing effects, a compensating curve or reverse curve of Spee may be necessary in the archwire.
The cost of lingual appliance treatment is greater than that for labial appliances. This is due partly to the increased chairside time and partly to the laboratory costs involved. Patients, however, appear to be willing to pay more money for appliances they deem more aesthetic.27 Costs are at least twice the amount for a labial appliance case, although fees vary considerably, depending on the complexity of the case.26 As a guide, at today's prices, for upper and lower lingual appliances, a range of £6,000 to £10,000 can be given.
Conclusion
Lingual appliances, despite a turbulent beginning, have come of age. Driven by market demand and the patient's desire for the ultimate in aesthetics, clinicians are treating increasing numbers of patients with lingual appliances. Advances in technology related to bracket design and laboratory procedures have overcome many of the earlier problems, however, tongue discomfort, speech problems and masticatory difficulty remain, often in the early stages of treatment. With careful patient selection and due regard for treatment biomechanics, lingual orthodontics is here to stay, adding a valuable asset to the orthodontist's armamentarium.