Subasioglu A, Savas S, Kucukyilmaz E Genetic background of supernumerary teeth. Eur J Dent. 2015; 9:153-158
Lubinsky M, Kantaputra PN. Syndromes with supernumerary teeth. Am J Med Genet A. 2016; 170:2611-2616
Brook A H. Dental anomalies of number, form and size: their prevalence in British schoolchildren. J Int Assoc Dent Child. 1974; 5:37-53
Fleming P S, Xavier G M, DiBiase AT, Cobourne MT. Revisiting the supernumerary: the epidemiological and molecular basis of extra teeth. Br Dent J. 2010; 208:25-30
Backman B, Wahlin Y B. Variations in number and morphology of permanent teeth in 7-year-old Swedish children. Int J Paediatr Dent. 2001; 11:11-17
Yusof W Z. Non-syndrome multiple supernumerary teeth: literature review. J Can Dent Assoc. 1990; 56:147-149
Paduano S, Rongo R, Lucchese A Late-developing supernumerary premolars: analysis of different therapeutic approaches. Case Rep Dent. 2016; 2016
Rocha R, Zasso M B, Floriano G Orthodontic traction in a patient with cleidocranial dysplasia: 3 years of follow-up. Am J Orthod Dentofacial Orthop. 2014; 146:108-118
Mundlos S. Cleidocranial dysplasia: clinical and molecular genetics. J Med Genet. 1999; 36:177-182
Waller A, Findeis S, Lee M J. Familial adenomatous polyposis. J Pediatr Genet. 2016; 5:78-83
Merjaneh L, Parks JS, Muir AB, Fadoju D. A novel TRPS1 gene mutation causing trichorhinophalangeal syndrome with growth hormone responsive short stature: a case report and review of the literature. Int J Pediatr Endocrinol. 2014; 2014
Milani D, Manzoni F M, Pezzani L Rubinstein–Taybi syndrome: clinical features, genetic basis, diagnosis, and management. Ital J Pediatr. 2015; 41
Spena S, Gervasini C, Milani D. Ultra-rare syndromes: the example of Rubinstein–Taybi syndrome. J Pediatr Genet. 2015; 4:177-86
Gjørup H, Haubek D, Jacobsen P, Ostergaard J R. Nance–Horan syndrome. The oral perspective on a rare disease. Am J Med Genet A. 2017; 173:88-98
Preiksaitiene E, Krasovskaja N, Utkus A R368X mutation in MID1 among recurrent mutations in patients with X-linked Opitz G/BBB syndrome. Clin Dysmorphol. 2015; 24:7-12
O’Byrne J J, Laffan E, Murray DJ, Reardon W. Oculo-faciocardio-dental syndrome with craniosynostosis, temporal hypertrichosis, and deafness. Am J Med Genet A. 2017; 173:1374-1377
Hosseini-Farahabadi S, Gignac SJ, Danescu A Abnormal WNT5A signaling causes mandibular hypoplasia in Robinow syndrome. J Dent Res. 2017; 96:1265-1272
Cammarata-Scalisi F, Avendaño A, Callea M. Main genetic entities associated with supernumerary teeth. Arch Argent Pediatr. 2018; 116:437-444
Basaran G, Erkan M. One of the rarest syndromes in dentistry: Gardner syndrome. Eur J Dent. 2008; 2:208-212
Madani M, Madani F. Gardner’s syndrome presenting with dental complaints. Arch Iran Med. 2007; 10:535-539
Wesley R K, Cullen C L, Bloom W S. Gardner’s syndrome with bilateral osteomas of coronoid process resulting in limited opening. Pediatr Dent. 1987; 9:53-57
Supernumerary teeth can be an important sign for early diagnosis of an underlying syndrome, and in some circumstances, may be one of the only presenting features. Dentists are best placed to detect supernumerary teeth and therefore, it is important to understand the syndromes associated with them to aid early diagnosis of any associated syndromes. Craniofacial, ophthalmological and gastro-intestinal findings are just a few of the characteristics that may cause a dentist to suspect an underlying genetic disorder. Although it is not within the scope for dentists to diagnose these rare associated syndromes, early referral to the general medical practitioner may in turn help patients access the interdisciplinary management they may need.
CPD/Clinical Relevance: An awareness of the signs and symptoms of syndromes associated with supernumerary teeth can aid early diagnosis.
Article
Supernumerary teeth are those present in addition to the normal complement of the dentition.1 They can occur in isolation or be associated with systemic features as part of a syndrome. The presence of multiple supernumerary teeth is rare and usually associated with certain underlying developmental disorders/syndromes.2
Although the prevalence of syndromes associated with supernumerary teeth is rare, the consequences of such syndromes if left undetected can be severe. Supernumerary teeth can occasionally be the only, or the first presenting feature of an associated syndrome. Dentists are best placed to detect supernumerary teeth and should be vigilant and up to date in their knowledge of the associated syndromes. In knowing what accompanying systemic signs and symptoms to be aware of in a patient's medical history and examination, this could in turn facilitate earlier referral for the diagnosis and long-term interdisciplinary management of these patients.
Supernumerary teeth
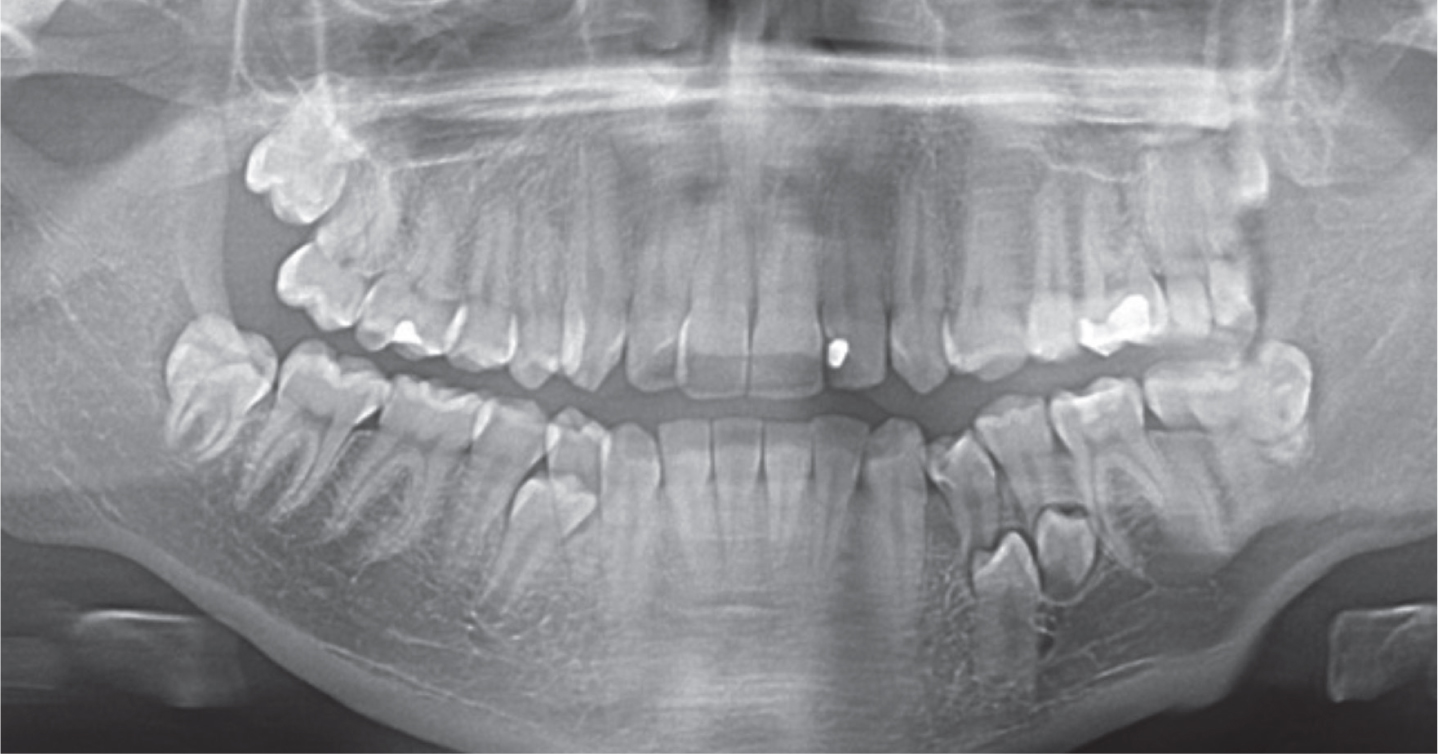
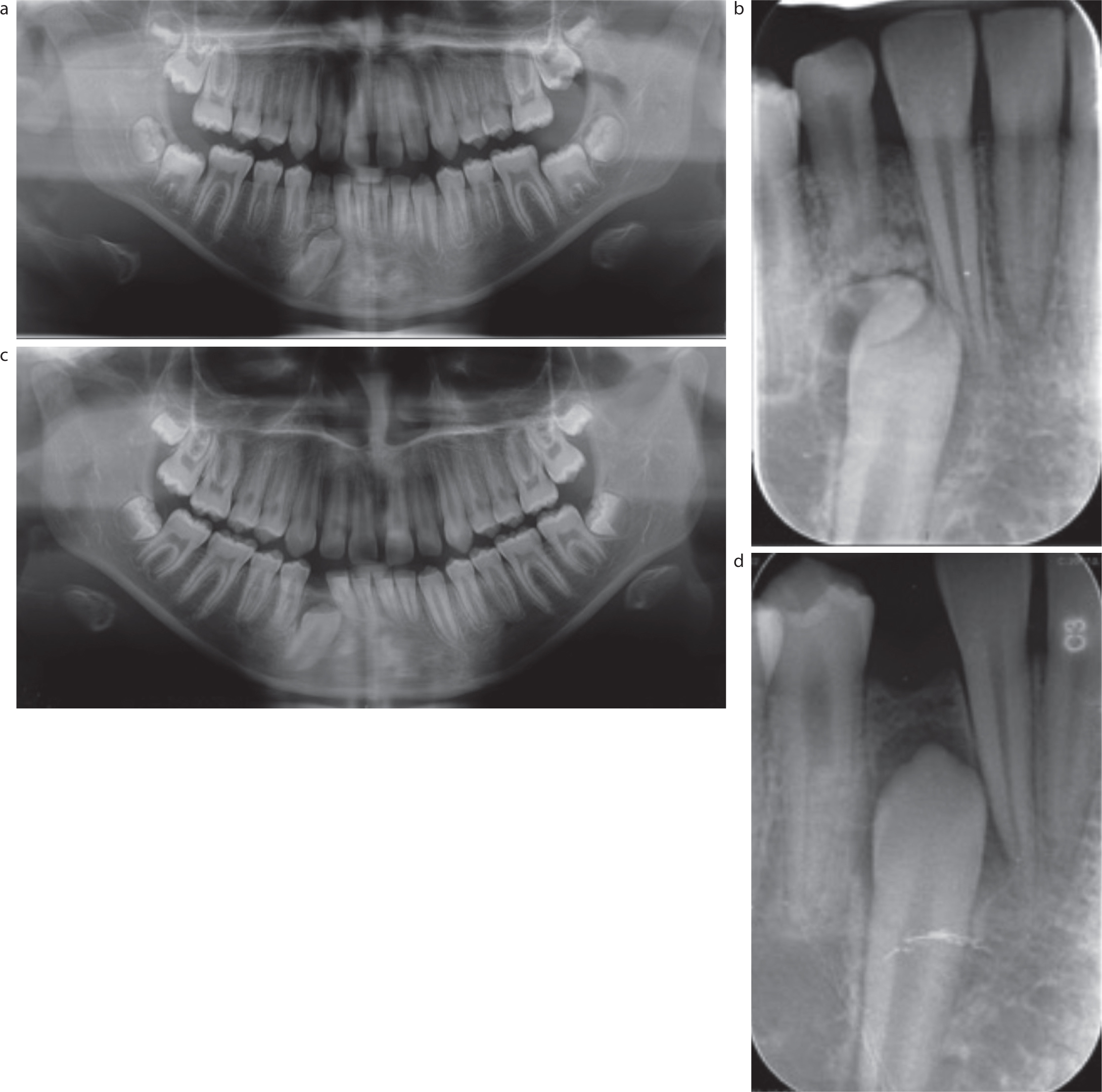
The prevalence of supernumerary teeth is reported to range between 0.1% and 3%. They are more frequently found in males than females and more common in the permanent than deciduous dentition.3 Supernumerary teeth are generally classified according to their morphology or location4 as described in Table 1. Although individual supernumerary teeth are usually found in the anterior maxilla,5 multiple supernumerary teeth occur more commonly in the mandibular premolar regions (Figures 1–4).6 The aetiology of supernumerary teeth is poorly understood; however, there is a clear genetic component because they tend to present in families, demonstrate ethnic and sexual dimorphism, and are a prominent feature of many syndromes.
Table 1. Classification of supernumerary teeth.
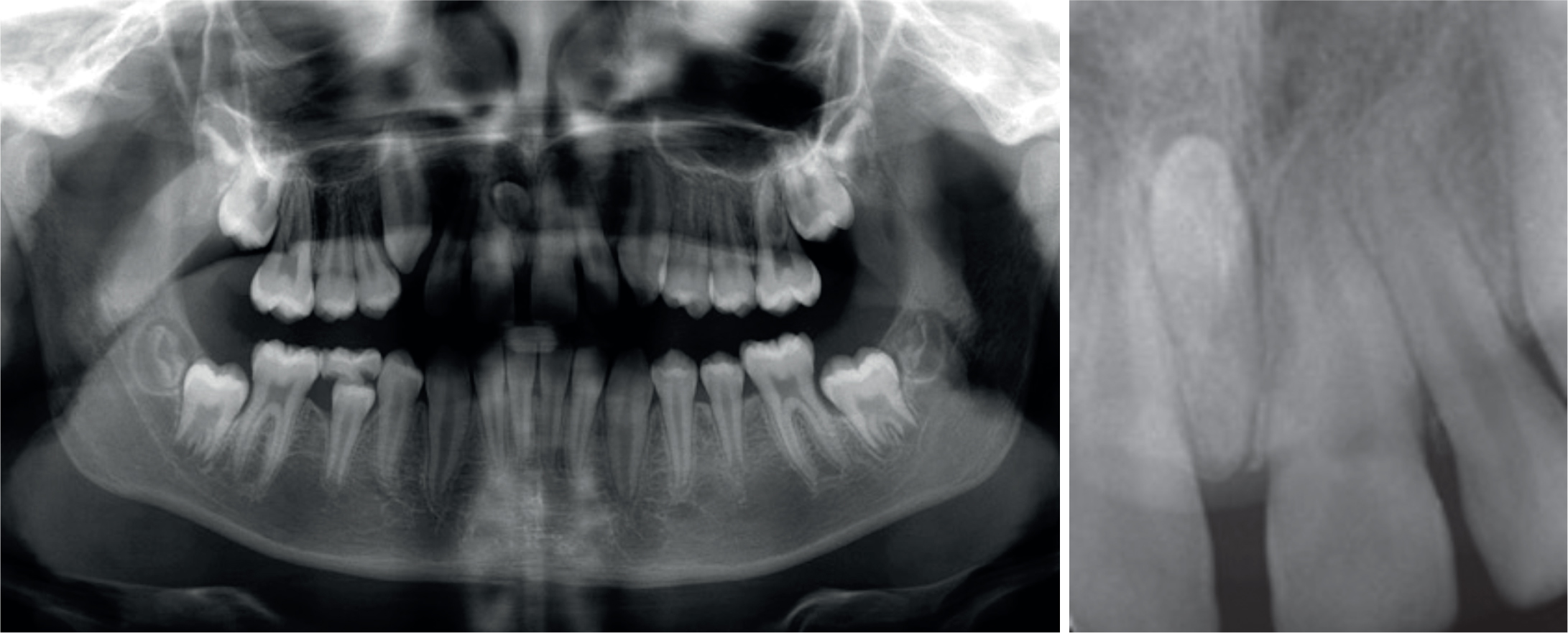
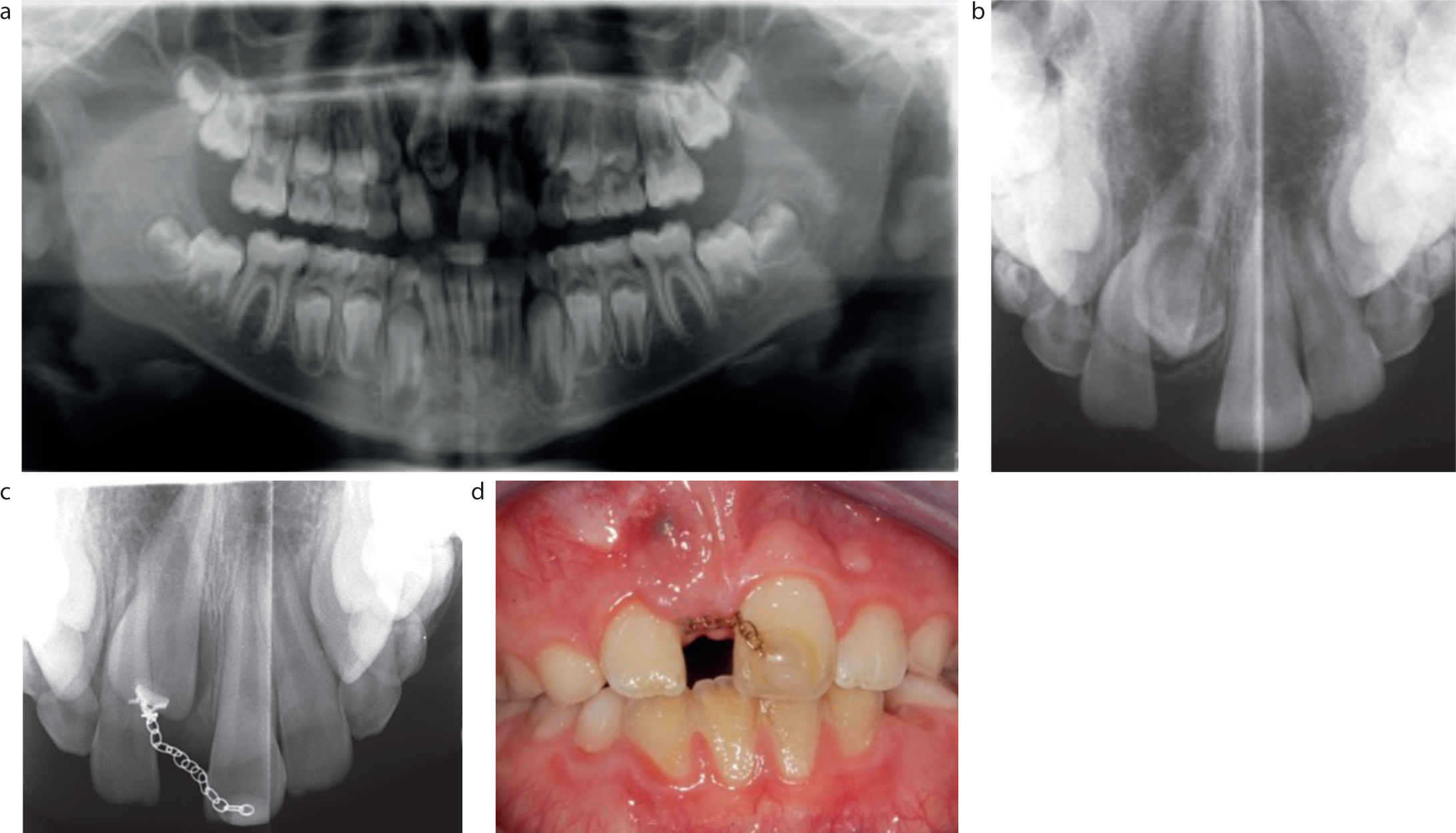
Figure 1. Frontal and upper occlusal photographs and DPT of a supplemental UR2.Figure 2. DPT showing multiple unerupted supplemental teeth in the lower left and right quadrants and possibly the upper right quadrant.Figure 3. DPT and long cone peri-apical radiograph showing an inverted conical supernumerary between the upper central incisors.Figure 4. (a,b) DPT and upper standard occlusal radiograph showing a tuberculate supernumerary obstructing the eruption of the UR1. (c,d) Upper standard occlusal radiograph and frontal photograph of the same patient following removal of the supernumerary and exposure and bonding of the UR1.
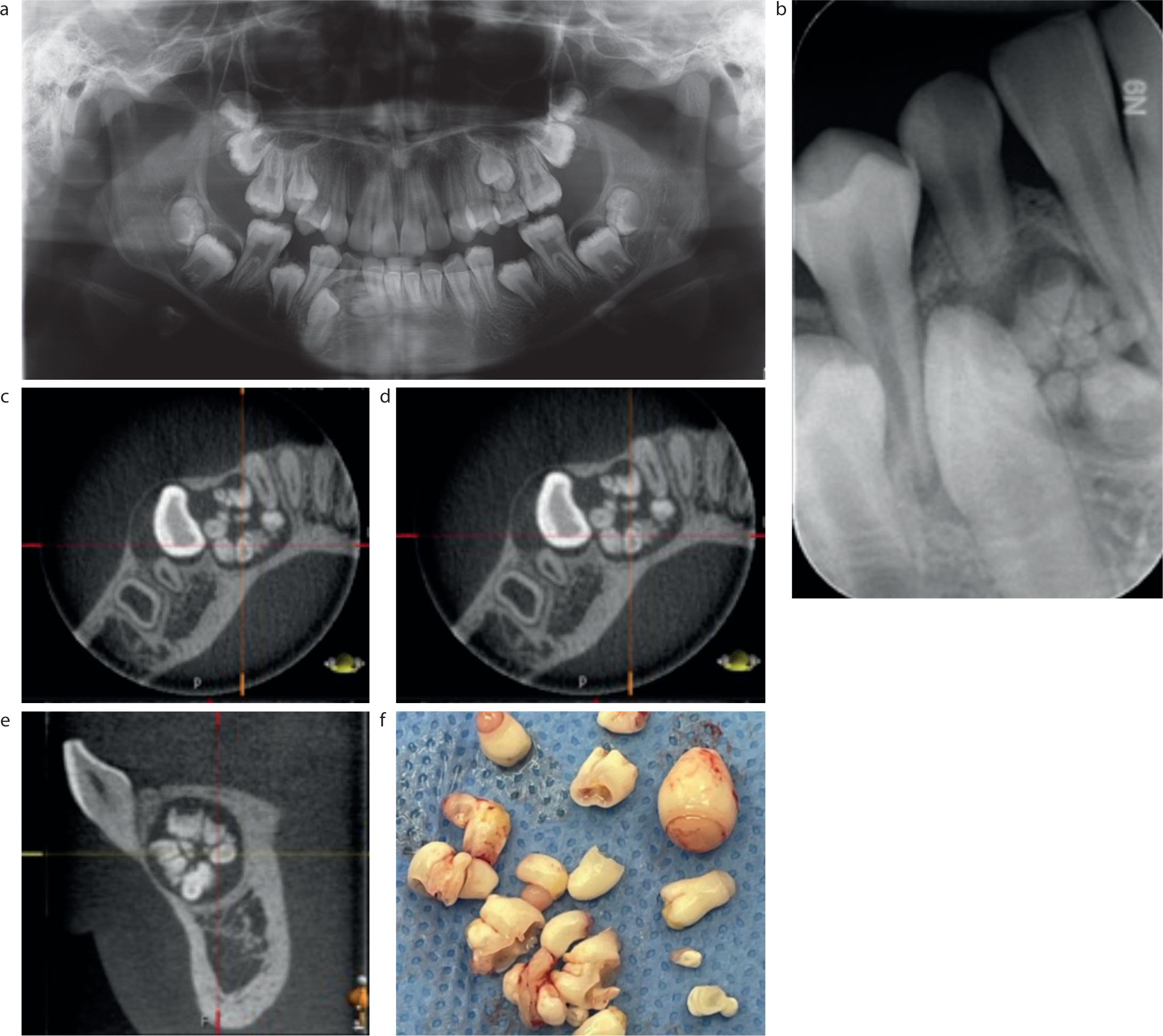
A thorough clinical and radiographic examination is required to detect the presence of supernumerary teeth. The eruption, orientation and morphological features associated with supernumerary teeth show wide variation, therefore, as part of the clinical and radiographic examination, the number of teeth should be counted in a systematic way. Possible complications associated with supernumeraries include local effects on the developing occlusion (crowding, spacing, impaction, displacement or rotations), cystic formation and resorption of adjacent teeth. Radiographic examination may include intra-oral and/or extra-oral radiographs. Dental panoramic tomographs (DPT) can show the full dentition, but lack the finer detail of intra-oral radiographs, and especially may not detect supernumeraries in the anterior maxilla due to superimposition of the spine. Therefore, as well as a DPT, supplementary intra-oral radiographs are often also required. In certain situations, a cone beam computed tomograph (CBCT) may be indicated, particularly when assessing the precise location of supernumeraries, to assess any resorption to adjacent teeth, or to aid planning surgical access (Figure 5).7 It is also important to appreciate that some supernumeraries are late forming, forming after the eruption of the permanent dentition and may not initially be detected.8 Therefore, if a patient presents with supernumerary teeth, clinicians should remain vigilant to the later diagnosis of further later forming supernumeraries.
Figure 5. (a–e) DPT, long cone peri-apical radiograph and CBCT of compound odontomes in the lower right quadrant obstructing the eruption of the LR3. (f) Clinical photograph of multiple compound odontomes / ‘denticles’ extracted from the previous patient.Figure 6. (a,b) DPT and long cone peri-apical radiograph showing an odontome obstructing the eruption of the LR3. (c,d) DPT and long cone peri-apical radiograph of the same patient following the extraction of the odontome showing an improvement in the position of the LR3.
Syndromes
Eight syndromes have been reported to have a strong association with supernumerary teeth.1,2 Diagnosis is primarily based upon identification of characteristic features from a thorough patient history, clinical and radiographic examination. In addition to this, genetic testing can reveal mutations of specific genes that can confirm the diagnosis.
The eight syndromes with a strong association with supernumerary teeth are detailed in Table 2 and are summarized below.9–19 It is currently unknown whether a specific type of supernumerary tooth is more common in any of these syndromes. Table 3 shows a summary of the systems affected by these eight syndromes.
Table 2. Characteristics of the eight syndromes strongly associated with supernumerary teeth.
Cleidocranial dysplasia
Familial adenomatous polyposis (FAP)
Trichorhino-phalangeal syndrome type I
Rubinstein–Taybi syndrome
Nance–Horan syndrome (cataract–dental syndrome)
Opitz BBB/G syndrome
Oculofaciocardio-dental syndrome
Autosomal dominant Robinow syndrome
Incidence
1 in a million9
1 in 10,00011
Unknown
1 in 100,000-125,00013
Unknown
1 in 10,000–50,00016
Unknown
1 in 500,00019
Inheritance
Autosomal dominant/sporadic
Autosomal dominant
Autosomal dominant
Autosomal dominant
X-linked
Autosomal dominant/X-linked
X-linked
Autosomal dominant
Gene mutation
RUNX210
APC11
TRPS-112
CREBBP and EP30014
NHS15
SPECC1L, MID117
BCOR18
MMTV and WNT5A19
Systems affected
Medical systems
Gastro-intestinal: adenomatous colon polyps with high risk of colorectal cancer Risk of cancer of the stomach, small intestine, pancreas, liver, biliary tree, thyroid, brain and skin
Cardiovascular: atrial and ventricular septal defects, mitral valve prolapse
Renal Genito-urinary
Ophthalmological features
Characteristic flat pigmented retinal lesion
Affected males have severe ophthalmological features including cataracts and poor vision Heterozygous females present with milder clinical manifestations
Congenital cataracts Secondary glaucoma
Skin and hair
Sparse hair on scalp, eyebrows and eyelashes
Hirsutism Keloid formation and predisposition to scarring
Hands and feet
Hands
Hands and feet
Hands and feet
Hands and feet
Hands
Skeletal
Short stature Scoliosis Chest abnormalities Aplastic/hypoplastic clavicles
Osteomas in the paranasal sinuses, mandible, skull and long bones Fibrous dysplasia of the skull
Protruding ears Midface hypoplasia Bulbous pear-shaped nose Long and flat philtrum Thin upper lip
Prominent forehead Full and arched eyebrows Ptosis of eyelids Downwards-slanting palpebral fissures Epicanthal fold Nasal lacrimal duct obstruction Beak-shaped nose with broad nasal bridge and low-hanging columella Grimacing or unusual smile Microcephaly
Broad prominent nasal bridge Bulbous nose Long narrow face
Craniosynostosis Prominent forehead Widow’s peak Hooded eyelids Hypertelorism Broad and flat nose Think upper lip Low set prominent ears and hearing loss
Long and narrow face High nasal bridge Broad nasal tip Bifid nose Ear deformities
Characterized as ‘fetal face’ High and broad forehead Frontal bossing Prominent eyes Hypertelorism Wide and depressed nasal bridge Short nose Midface hypoplasia Micrognathia
Intra-oral features
Supernumerary teeth High arched, narrow palate Cleft palate Delayed eruption Impaction of multiple teeth
Multiple unerupted supernumeraries High arched palate Microdontia Delayed tooth eruption
Supernumerary teeth High arched palate Talon cusps (particularly central incisors) Developmental grooves in teeth Hypodontia Natal teeth
Supernumerary teeth including supernumerary maxillary incisors Screwdriver blade-shaped incisors
Supernumerary teeth High arched palate CLP Geographic/bifid tongue Short lingual frenum Hypodontia
Supernumerary teeth including involvement of canines High arched narrow palate Radiculomegaly (root gigantism) of permanent teeth Delayed eruption Hypodontia
Supernumerary teeth Gingival hypertrophy
Learning difficulties
Moderate–severe learning difficulties
Learning and behavioural difficulties
Learning difficulties, neuropsychiatric disorders
Learning difficulties and ADHD
Table 3. Summary table of the systems affected by the eight syndromes strongly associated with supernumerary teeth.
Cleidocranial dysplasia is a rare genetic condition that affects the development of the teeth, skull and bones. There are extreme variabilities in the phenotypic presentation of cleidocranial dysplasia where some patients present with severe skeletal abnormalities and others only have supernumerary teeth with no systemic signs or symptoms. The systems commonly affected are skeletal, craniofacial, intra-oral features and abnormalities of the hands.9 Supernumerary teeth in patients with cleidocranial dysplasia are seen approximately 22% of the time in the maxillary incisor region and 5% in the molar regions.1 It is thought that the supernumerary teeth are likely to form by reactivation of the dental lamina after crown formation.
Familial adenomatous polyposis (FAP)
FAP is characterized by the development of more than 100 adenomatous colon polyps with the number usually increasing significantly after puberty.11 Adenomatous colon polyps have a high risk of malignancy; therefore, early diagnosis is critical. Common symptoms include abdominal pain, diarrhoea, melena and severe dehydration due to electrolyte imbalances and depletion from diarrhoea. Individuals with FAP also have an increased risk of developing desmoid tumours and cancer in the stomach, small intestine, pancreas, liver, biliary tree, thyroid and brain.20
Gardner syndrome is a variant of FAP where individuals develop multiple adenomatous colon polyps and in addition have various cutaneous and non-cutaneous features. Intra-oral features have been described to be present in 30–75% of patients with Gardner syndrome,21 including supernumerary teeth (11–27% cases) and osteomas (68–82% cases). Osteomas can be found in the paranasal sinuses and mandible.22 In the mandible, central or lobulated osteomas can be found; central osteomas characteristically occur near the roots of the teeth, and lobulated types arise from the cortex and most commonly occur at the angle of the mandible.23
Trichorhinophalangeal syndrome type 1 (TRPS1)
TRPS1 is characterized by distinctive abnormalities of the hair, face and skeleton.12 Three subtypes have been classified according to their clinical differences.20 The characteristics of TRPS1 include abnormalities of the hair, skeleton, hands and feet as well as craniofacial and intra-oral features.
Rubinstein–Taybi syndrome
Rubinstein–Taybi syndrome is characterized by abnormalities of the cardiovascular, respiratory, genito-urinary systems as well as skeletal, craniofacial and intra-oral features.
Nance–Horan syndrome
Nance–Horan syndrome, also known as cataract–dental syndrome, is associated with both dental and ophthalmological anomalies, including congenital cataracts, microcornea and nystagmus resulting in poor vision.20 Affected males have more severe ophthalmological features, whereas heterozygous females present with milder clinical manifestations, which may include microcornea or congenital cataracts causing only slightly decreased clarity of vision.15
Opitz BBB/G syndrome
Opitz BBB/G syndrome is characterized by abnormalities along the midline of the body including cardiovascular, gastro-intestinal, craniofacial and intra-oral abnormalities.20
Oculofaciocardiodental syndrome
Oculofaciocardiodental syndrome is an X-linked dominant disorder that is seen in heterozygous females and is lethal in males.18 It is characterized by ophthalmological, cardiovascular, skeletal, craniofacial and intra-oral abnormalities.
Autosomal dominant Robinow syndrome
Robinow syndrome is a rare disorder that has an autosomal dominant and a recessive form, and supernumerary teeth appear to be only associated with the dominant form.2
Supernumerary teeth have also been shown to be associated with clefts of the lip and/or palate (CLP). However, in this article we have excluded discussing CLP as it can occur in isolation or in combination with a syndrome.
The literature also revealed case reports of supernumerary teeth less commonly associated with other syndromes including Ehlers–Danlos syndrome, Ellis–van Creveld syndrome, Marfan syndrome, Apert/Crouzon syndrome, Down syndrome, hereditary gingival fibromatosis, Gorlin–Gortz syndrome and incontinentia pigmenti. Additionally, case reports have found patients with associated syndromes often presented with a combination of hypodontia and supernumerary teeth within a single dentition. A few examples include patients with FAP, oculofaciocardiodental syndrome, Rubinstein–Taybi syndrome, Opitz BBB/G syndrome, Down syndrome, epidermolysis bullosa and Marfan syndrome.
Onward management of patients presenting with multiple supernumeraries
In patients with multiple supernumerary teeth, dentists must consider the possibility of an associated syndrome. In circumstances when the dentist suspects an underlying genetic disorder, early referral to the patient's general medical practitioner (GMP) is paramount to enable patients to access the interdisciplinary management that they need. The GMP will be able to arrange the appropriate investigations and refer onwards as required to ensure the most appropriate medical specialties are involved in the patient's care.
It is suggested that the questions shown in Table 4 are important to ask the patient to obtain a comprehensive history to aid the possible early detection of any syndromes associated with supernumerary teeth.
Table 4. Key questions to consider/ask patients to aid possible early detection of any syndromes associated with supernumerary teeth.
Is there a family history of supernumerary teeth?
Have you experienced any gastro-intestinal symptoms (i.e. abdominal pain, diarrhoea, melena or severe dehydration)?
Do you have any problems with your eyes, heart, breathing, kidneys, skin, hands, feet or skeleton?
Are there any associated craniofacial or intra-oral features?
Are you seeing any other medical specialties or allied health professionals?
Conclusion
Although the syndromes associated with supernumerary teeth are rare, the consequences, if left undetected, are severe. Early detection of supernumerary teeth can aid early diagnosis of an associated syndrome with potentially serious risks such as gastro-intestinal carcinomas. To detect supernumerary teeth, as part of a thorough clinical and radiographic examination, the number of teeth should be counted in a systematic way. Dentists are best placed to detect supernumerary teeth and should be aware of associated signs and symptoms to look out for in the patient history and examination in order to aid early diagnosis of any associated syndrome.
Craniofacial, ophthalmological (such as congenital cataract) or skeletal findings as well as cardiovascular disease or gastro-intestinal upset are just a few of the characteristics that may cause the dentist to suspect an underlying genetic disorder. Although it is not within the scope of dentists to diagnose these rare associated syndromes, early referral to the GMP may in turn help patients to access the complex interdisciplinary care that they require.