Arid J, Xavier TA, da Silva RAB RANKL is associated with persistent primary teeth and delayed permanent tooth emergence. Int J Paediatr Dent. 2019; 29:294-300 https://doi.org/10.1111/ipd.12467
Din A, Bhatti N, Sharma PK Orthodontic management of delayed permanent tooth eruption and a case report of hyper-IgE syndrome. Orthod Update. 2017; 10:24-27 https://doi.org/10.12968/ortu.2017.10.1.24
Suri L, Gagari E, Vastardis H Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004; 126:432-445 https://doi.org/10.1016/j.ajodo.2003.10.031
Cameron AC, Widmer RP: Mosby; 2013
Scott JK, Atack NE The developing occlusion of children and young people in general practice: when to watch and when to refer. Br Dent J. 2015; 218:151-156 https://doi.org/10.1038/sj.bdj.2015.54
Makino Y, Fujikawa K, Matsuki-Fukushima M Role of innate inflammation in the regulation of tissue remodeling during tooth eruption. Dent J (Basel). 2021; 9 https://doi.org/10.3390/dj9010007
Nagata M, Ono N, Ono W Mesenchymal progenitor regulation of tooth eruption: a view from PTHrP. J Dent Res. 2020; 99:133-142 https://doi.org/10.1177/0022034519882692
Frazier-Bowers SA, Puranik CP, Mahaney MC The etiology of eruption disorders – further evidence of a ‘genetic paradigm’. Semin Orthod. 2010; 16:180-185 https://doi.org/10.1053/j.sodo.2010.05.003
Vitalle MS, Weiler R, Niskier S, Braga J Delayed tooth eruption in an adolescent with hypothyroidism. Revista Paulista de Pediatria. 2012; 30:613-616
Miranda Galvis M, Faustino ISP, Ferraz FC Orthodontic treatment in a patient with cherubism: bBenefits and limitations. Spec Care Dentist. 2020; 40:291-297 https://doi.org/10.1111/scd.12457
Balaji MS, Sundaram RK, Karthik P, Asokan K Pycnodysostosis: a bone dysplasia with unusual oral manifestation. Indian. 2014; 5:218-221 https://doi.org/10.4103/0975-962X.144738
Boos Lima F, Viana APC, Lima LHF A rare case of Gorlin-Goltz syndrome in children. Case Rep Dent. 2019; 2019 https://doi.org/10.1155/2019/1608783
Koh KJ, Park HN, Kim KA Gardner syndrome associated with multiple osteomas, intestinal polyposis, and epidermoid cysts. Imaging Sci Dent. 2016; 46:267-272 https://doi.org/10.5624/isd.2016.46.4.267
de la Dure-Molla M, Quentric M, Yamaguti P Pathognomonic oral profile of Enamel Renal syndrome (ERS) caused by recessive FAM20A mutations. Orphanet J Rare Dis. 2014; 9 https://doi.org/10.1186/1750-1172-9-84
Kala Vani SV, Varsha M, Sankar YU Enamel renal syndrome: a rare case report. J Indian Soc Pedod Prev Dent. 2012; 30:169-172 https://doi.org/10.4103/0970-4388.100006
Meixner I, Hagl B, Kroner CI Retained primary teeth in STAT3 hyper-IgE syndrome: early intervention in childhood is essential. Orphanet J Rare Dis. 2020; 15 https://doi.org/10.1186/s13023-020-01516-3
Frías M, Lemus O, Ayala C Oral and systemic manifestations of congenital hypothyroidism in children. A case report. J Oral Res. 2015; 4:329-334 https://doi.org/10.17126/joralres.2015.063
OMIM. An online catalog of human genes and genetic disorders. https://www.omim.org (accessed July 2024)
Orphanet. The portal for rare diseases. www.orpha.net (accessed July 2024)
Klein OD, Oberoi S, Huysseune A Developmental disorders of the dentition: an update. Am J Med Genet C Semin Med Genet. 2013; 163C:318-332 https://doi.org/10.1002/ajmg.c.31382
Atar M, Korperich EJ Systemic disorders and their influence on the development of dental hard tissues: a literature review. J Dent. 2010; 38:296-306 https://doi.org/10.1016/j.jdent.2009.12.001
Bouare F, Noureldine MHA, Hajhouji F Complex craniosynostosis in the context of Carpenter's syndrome. Childs Nerv Syst. 2022; 38:831-835 https://doi.org/10.1007/s00381-021-05288-4
Elsten E, Caron C, Dunaway DJ Dental anomalies in craniofacial microsomia: A systematic review. Orthod Craniofac Res. 2020; 23:16-26 https://doi.org/10.1111/ocr.12351
Kjaer I Mechanism of human tooth eruption: review article including a new theory for future studies on the eruption process. Scientifica (Cairo). 2014; 2014 https://doi.org/10.1155/2014/341905
Anomalies of teeth eruption and/or resorption. In: Bloch-Zupan A, Sedano HO, Scully C (eds). London: Elsevier;
Răducanu A, Feraru V Delayed eruption – case study. Oral Health and Dental Management. 2007; VI:58-65
Tooth eruption comprises a highly coordinated cascade of complex cellular and molecular interactions resulting in axial movement of the tooth germ from an intra-osseous position to its functional occlusion. Odontogenesis is under genetic control, governed by more than 300 genes, with environmental factors playing a comparatively minor role. Delayed tooth eruption (DTE) describes the most frequently encountered deviation from normal eruption and can be the solitary materialization of local or systemic pathology. Where local pathology has been excluded, the dentist should be aware of the multitude of systemic conditions that may be contributing, and liaise with relevant medical colleagues. This article provides a review of the literature regarding the systemic causes of DTE.
CPD/Clinical Relevance: Systemic conditions can be aetiological factors in delayed tooth eruption.
Article
Delayed tooth eruption (DTE), or delayed tooth emergence is defined as the emergence, or eruption of a tooth into the oral cavity at a time statistically different from what would be expected for age, sex and ethnicity.1–3 This is generally accepted to be greater than 12-months' delay beyond chronological norms,4 or greater than 6 months compared to eruption of the contralateral permanent tooth.5 Local factors that result in DTE are numerous, and are listed in Table 1.
Supernumerary teeth
Ectopic eruption of permanent tooth
Impaction of primary tooth
Crowding
Ankylosis of primary tooth
Premature loss of primary tooth
Trauma of primary tooth
Cleft palate/lip
Post radiation/chemotherapy
Cysts
Odontogenic/non-odontogenic tumours
Scarring of gingiva (post-surgical)
Gingival hyperplasia/gingival fibromatosis
Physiology and molecular biology of tooth eruption
Odontogenesis, or tooth eruption, is under genetic control, governed by more than 300 genes,6 with environmental factors playing a comparatively minor role. It is a highly complex and tightly regulated physiological process that occurs over a broad chronological age. Numerous theories have been postulated to explain the eruption process, hypothesizing involvement of many adjacent tissues and chemical mediators. More recently, the dental follicle, a sac-like membranous tissue that surrounds the developing tooth germ has been promoted as a pivotal mediator of eruption owing to its production of copious mediators (tumour necrosis factor alpha (TNF-α), transforming growth factor beta (TGF-β), receptor activator of nuclear factor kappa B ligand (RANKL), colony stimulating factor 1 (CSF-1), and interleukin-1 (IL-1)).7 Stellate reticulum cells of the dental follicle secrete parathyroid hormone-related peptide (PTHrP), an imperative autocrine/paracrine cytokine that exerts pleiotropic effects regulating tooth eruption.8,9 RANKL, CSF-1, and TNF-α secreted by cells of the dental follicle are quintessential for differentiation of precursor mononuclear cells into osteoclasts, which govern eruptive tooth movement.7 Osteoprotegerin (OPG) is a cytokine with a role in inhibiting osteoclastogenesis and prohibits osteoclast activity by binding to RANKL.10 The RANKL/OPG axis provides an essential mechanism to regulate a balance between osteoclastic resorption and osteoblastic deposition.10 Much of our understanding of the molecular mechanisms of tooth eruption are attributable to the study of genetic diseases where functional mutations in mediators such as RANKL or PTHrP result in delayed tooth eruption or primary failure of eruption.
Delayed tooth eruption in systemic disease
Systemic and genetic causes of DTE are less widely described in the literature compared to local factors. In the absence of aetiological local factors, the possible role of systemic conditions must be considered (Table 2 and Appendix 1).
Craniofacial microsomiaEllis Van Creveld syndromeMucopolysaccharidosis (Type X)Pierre Robin sequence
Mechanisms by which systemic disease can cause delayed tooth eruption
Bone defects
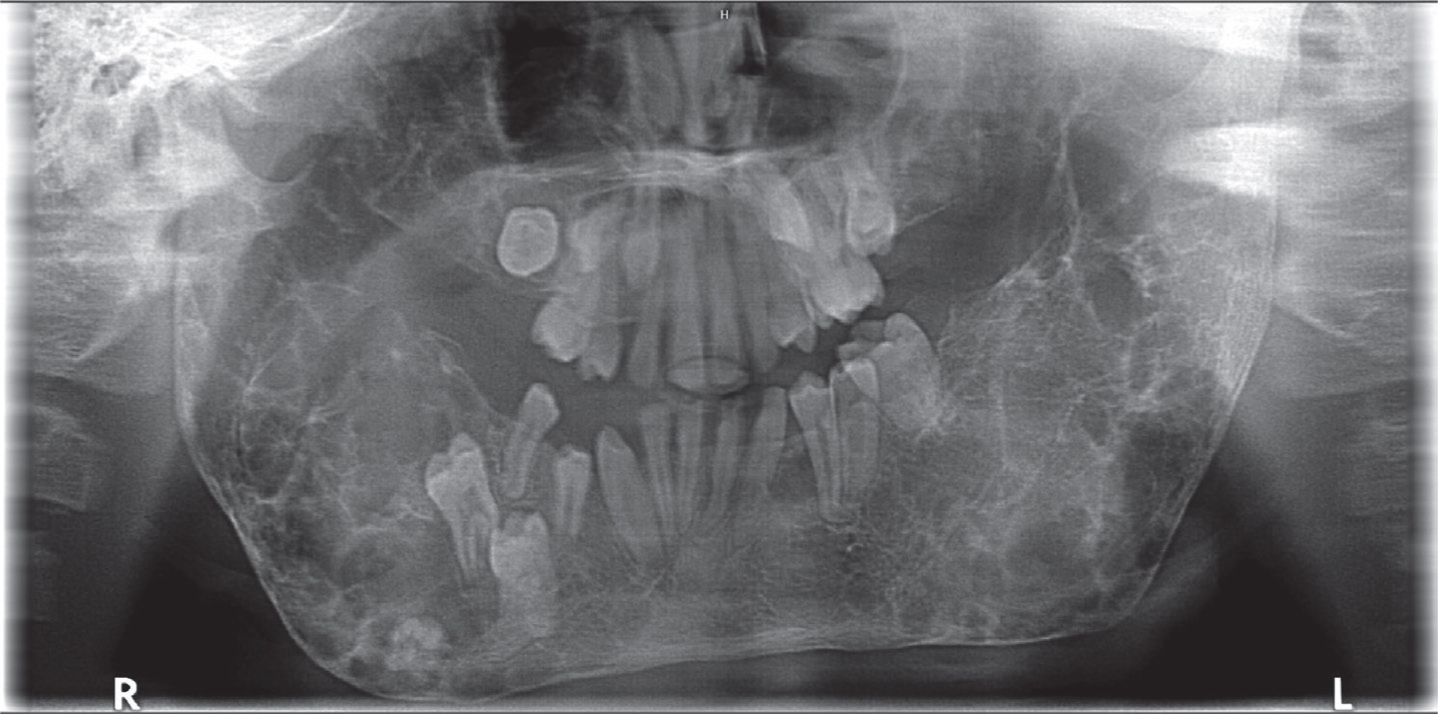
Osteoclasts have an elementary role in clearing the eruption pathway for the developing tooth by resorbing the cortical shell of alveolar bone occlusally.8 Defects in osteoclastic function subsequently have the propensity to delay or even preclude normal eruption. Cherubism (Figure 1), an autosomal dominant fibro-osseous disorder resulting in bilateral symmetrical enlargement of the maxilla and mandible demonstrates the clinical sequalae of defective osteoclastic function.11 The SH3BP2 gene, which is mutated in cherubism has a cardinal role in signalling transduction pathways, which ultimately increase osteoclastic function during tooth eruption,11 with bone being replaced by fibrous hypervascular tissue.
Figure 1. Orthopantogram of a patient with cherubism showing delayed tooth eruption (11 years and 6 months).
The effects of osteopetrosis (marble bone disease) on DTE are clearly discernible and attributed to inactivity or absence of fully functioning osteoclasts. Genetically, mutations in one of the several genes that support acidification, and consequential dissociation of calcium hydroxyapatite at the resorption pit, cause the defective bone resorption seen in osteopetrosis. By a comparable mechanism, DTE is consistently observed in patients with pycnodyostosis, a lysosomal storage disorder characterized by sclerosing bony dysplasia. It is a rare autosomal recessive disorder with an estimated prevalence of 1 in 1 million.12 Mutations in cathepsin K (CTSK) lead to defective osteoclastic resorption. CTSK is a lysosomal cysteine protease that has a central role in bony remodelling and is highly expressed by osteoclasts.
Multiple tumours or cysts
Cherubism provides an example of a syndromic condition that results in DTE by more than one mechanism. Bony expansion and distortion of the alveolar ridges by soft fibrous tissue histologically comparable to giant cell granulomas obscures the eruption pathway manifesting as failed eruption or DTE (Figure 1). Gorlin–Goltz syndrome, is an autosomal dominant condition characterized by basal cell carcinomas, odontogenic ketatocysts, palmoplantar pits, bifid ribs, calcification of the falx cerebri and coarse facial features among other characteristics.13 The presence of multiple odontogenic keratocysts may displace unerupted teeth, thus contributing to delayed eruption. Finally, the presence of osteomas in up to 82% of patients with familial adenomatous polyposis explains a mechanism by which DTE may also be attributed to tumours in addition to supernumerary teeth.14
Gingival hyperplasia
Hereditary gingival fibromatosis has the propensity to impede normal eruption by providing a mucosal barrier. The array of syndromes reported in the literature describing gingival fibromatosis is diverse (Table 2). Cowden syndrome, an autosomal dominant disorder, is characterized by multiple hamartomas histologically presenting as papillomatous lesions or fibromas.15 Comparatively, patients with enamel renal syndrome (ERS), a genetic disorder caused by mutations in the FAM20A gene, is characterized by hypoplastic amelogenesis imperfecta and nephrocalcinosis.16,17 Patients with ERS can present with focal ectopic calcification of gingival connective tissue, tissue in proximity to odontogenic epithelium, vasculature, and in the pericoronal follicles of impacted teeth.16 Infantile systemic hyalinosis on the other hand, presents with excessive hyaline deposition in multiple tissues including the gingiva. Despite variations in the exact histology of the overgrowth, the clinical manifestations of hereditary gingival fibromatosis are comparable. Commonly, the overgrowth is slowly progressive involving either the marginal and/or attached gingiva. Dentists have a fundamental role in understanding the various causes of drug-induced, idiopathic and syndromic causes of gingival fibromatosis and should liaise with appropriate medical colleagues as necessary.
Defective resorption of the primary tooth
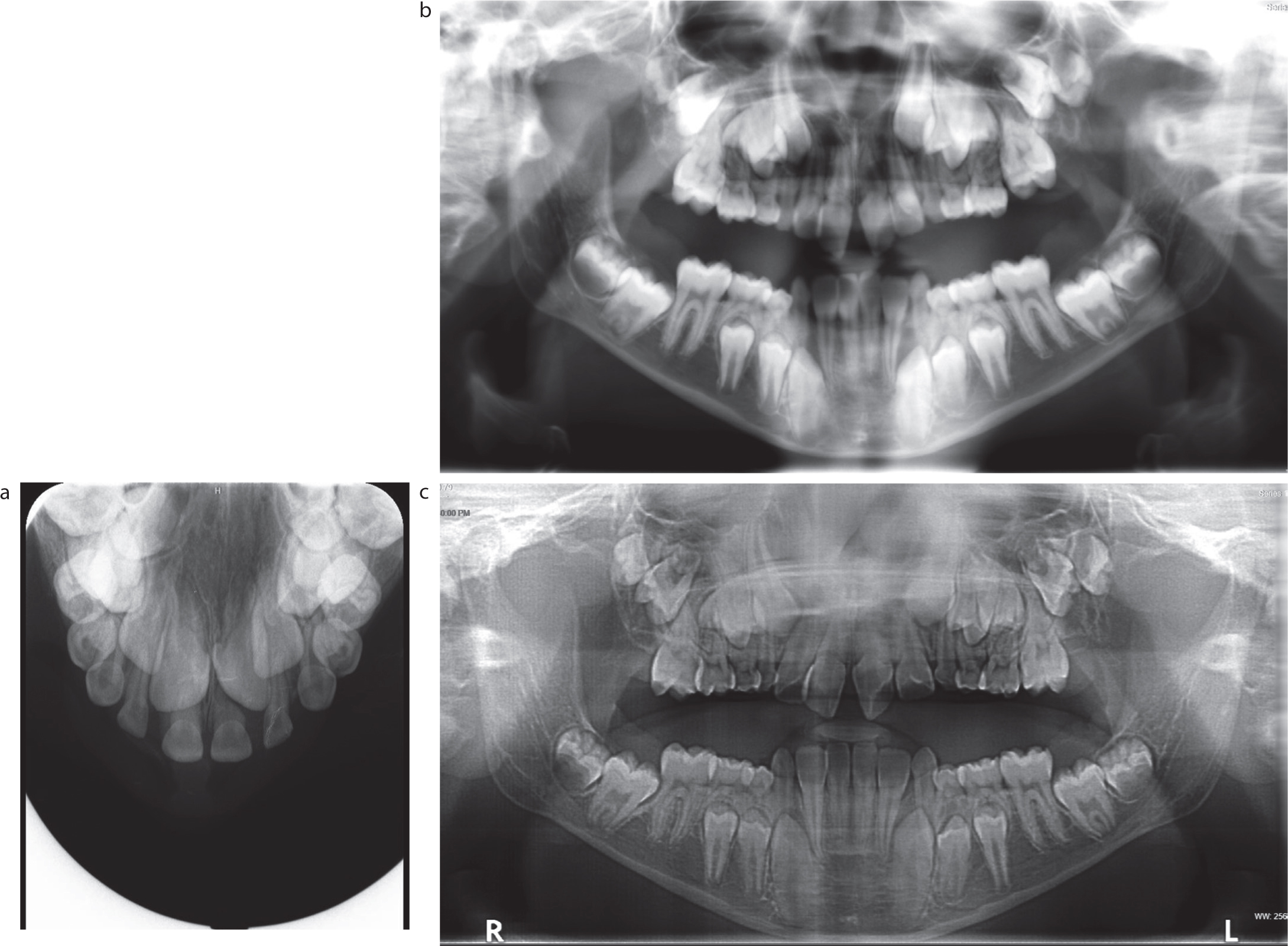
Hyperimmunoglobulin E (HIES) (Job syndrome) is a primary immunodeficiency syndrome characterized by high serum levels of immunoglobulin E (IgE).2 Genetically, mutations in the signal transducer and activator of transcription 3 (STAT3) gene manifest as defective antibody maturation and B-cell development resulting in recurrent Staphylococcus aureus, Haemophilus influenzae and Streptococcus pneumoniae infections.18 An example of this is seen in Figure 2, depicting a patient with STAT3 dominant negative loss of function mutation (autosomal dominant hyper IgE syndrome) and Crouzon-like craniosynostosis. Impaired and delayed resorption of primary roots is a commonly cited occurrence in STAT3-hyperimmunoglobulin-E syndrome, with the suspected aetiology being persistence of cells of the Hertwig's epithelial root sheath (HERS).18 Another proposed mechanism of delayed root resorption is defective odontoclastic function. Osteopontin (OPN), a protein involved in bony remodelling by promoting osteoclastic activity, has been found to be deficient in HIES patients, providing another possible theory for retained primary teeth. Without appropriately prescribed extractions of retained primary teeth in HIES, delayed tooth eruption of the permanent dentition is the norm. The dental radiographs at 8, 10 and 12 years of age illustrate these points.
Figure 2.
(a) Maxillary occlusal radiograph taken at 8 years, 2 months for a patient with autosomal dominant hyper IgE syndrome and Crouzon's-like craniosynostosis. (b) The patient at 10 years and 4 months following the removal of the primary incisors. (c) The patient at 12 years, 1 month. Delayed tooth eruption of the posterior dentition is evident.
Hormonal changes
Thyroid hormones have receptors in numerous body systems, with dysfunction in endocrine systems having multi-system effects. Congenital hypothyroidism is the most common paediatric endocrinopathy;19 however, delayed tooth eruption is also commonly reported in hypopituitarism, hypoparathyroidism and pseudohyoparathyroidism.3 The RANKL/OPG axis, an important mechanism for maintaining the relationship between osteoclastic resorption and osteoblastic production of new bone is regulated by various hormones including thyroid hormones.10 Hypothyroidism results in localized decreased synthesis and degradation of proteins, causing both delayed tooth development and eruption.10
Discussion
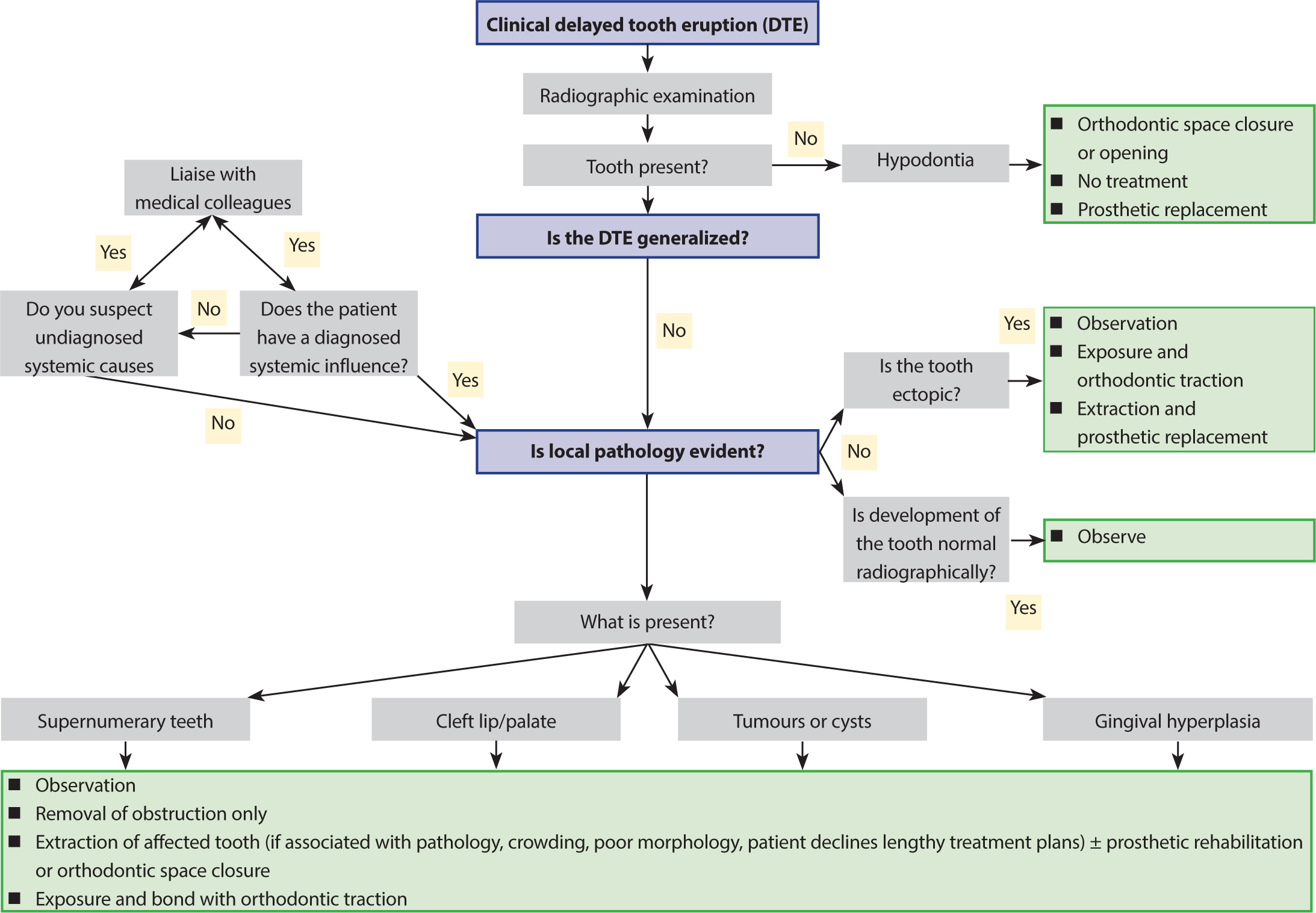
Accurate diagnosis of the cause of DTE is imperative to facilitate the appropriate treatment to produce the best possible outcomes. Obtaining a comprehensive medical history, as for any patient, is important to screen for genetic, inherited, endocrine and metabolic disorders. In the absence of the well-described local causes, the systemic conditions need to be considered (Figure 3, Appendix 1). It is important to liaise with the patient's primary medical team, not only to confirm the diagnosis, but also to understand the wider aspects of the condition and how it is being managed. The management of DTE requires an understanding of the aetiology of the condition to ensure that the correct approach is selected. There is no ‘cookbook’ recipe to manage DTE in many of these cases, and the impact of the condition on the patient and their family needs to be carefully evaluated before embarking on lengthy, time-consuming treatment. In some cases, no treatment may be the best option.
Figure 3. Flow diagram showing the suggested approach in diagnosis and management of clinical delayed tooth eruption (DTE).
Conclusion
The causes of DTE are numerous and can be broadly split into local, or much more rarely, systemic causes. The importance of obtaining a medical diagnosis and understanding how it might be the cause of DTE is crucial to inform the treatment planning process. If in doubt, get advice – both medical and dental.