Fuentes R, Borie E Bilateral macrodontia of mandibular second premolars: a case report. J Morph Sci. 2011; 28:212-215
Nemes JA, Alberth M The Ekman-Westborg and Julian trait: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2006; 102:659-662
Dugmore CR Bilateral macrodontia of mandibular second premolars: a case report. Int J Paed Dent. 2001; 11:69-73
O'Sullivan EA Multiple dental anomalies in a young patient: a case report. Int J Paed Dent. 2000; 10:63-66
Reichart PA, Westergaard J, Jensen KA Macrodontia of a mandibular premolar. Oral Surg. 1977; 44:606-609
Groper JN Macrodontia of a single tooth: review of literature and report of case. J Am Dent Assoc. 1987; 114
Rootkin-Gray VF, Sheehy EC Macrodontia of a mandibular second premolar: a case report. ASDC J Dent Child. 2001; 68:347-349
Primack JE Individual bilateral megadontism: report of a case. J Am Dent Assoc. 1967; 75:655-657
Hermel J, Yardeni J, Hass N Bilateral molarization of teeth erupted in the region of second mandibular premolars. Am J Phys Anthrop. 1968; 28:345-350
Peck S, Peck H Megadontism anomaly of the mandibular second premolars. Oral Surg. 1983; 55
Dadpe M, Kale YJ, Patil PS Molarization of the mandibular second premolars with concurrent dentin dysplasia: a rare case report. Int J Contemp Dent. 2010; 1:66-69
Canoglu E, Canoglu H, Aktas A, Cehreli Z Isolated bilateral macrodontia of mandibular second premolars: a case report. Eur J Dent. 2012; 6:330-334
Kyriazidou A, Haider D, Mason C, Parekh S, Bloch-Zupan A Case report: macrodont mandibular second premolars, a hereditary dental anomaly. Eur Archiv Paed Dent. 2013; 14:411-416
Hall RJLondon: Chapman and Hall Medical; 1964
Ekman-Westborg B, Julin P Multiple anomalies in dental morphology: macrodontia, multituberculism, central cusps and pulp invaginations. Oral Surg Oral Med Oral Pathol Oral Radiol. 1974; 38:217-222
Solanki M, Patil S, Baweja DK, Noorani HPKS Talon cusps, macrodontia and aberrant tooth morphology in Berardinelli syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2008; 105:e41-e47
Pereira T, Shetty S, Pereira S Permanent mandibular incisor with multiple anomalies – report of a rare clinical case. Ped Dental J. 2014; 24:67-70
Brook AH A unifying aetiological explanation for tooth anomalies of human tooth number and size. Archiv Oral Biol. 1984; 29:373-378
Garib DG, Peck S Extreme variations in the shape of mandibular premolars. Am J Orthod Dentofacial Orthop. 2006; 130:317-323
Chate RA Odontometric evaluation of mandibular premolars with tooth shape deviation: a case-control study. Angle Orthod. 2012; 82:785-791
Moyers RE, van der Linden FPGM, Riolo ML, McNamara JA Standards of human occlusal development.Ann Arbor: Center for Human Growth and Development, University of Michigan; 1976
Isolated bilateral macrodontia of the mandibular second premolars is a rare condition. We believe that the case reported here is the first in which isolated bilateral macrodontia of the mandibular second premolars presents with numerous dental anomalies affecting other teeth. A 14-year-old boy was referred to the Paediatric Dental Department of King's College Hospital with a partially erupted mandibular left second premolar. Clinical and radiographic examination subsequently revealed macrodontia of both mandibular second premolar teeth and multiple other dental anomalies. This report discusses the presentation and multidisciplinary management of this case.
CPD/Clinical Relevance: This case report describes an already rare condition made even more extraordinary owing to its presentation with multiple other dental anomalies.
Article
Macrodontia is a rare dental anomaly and can be characterized by an excessive enlargement of all tooth structures and can be associated with morphological anomalies.1
Macrodontia can be classified as ‘true generalized’, ‘relative generalized’ or ‘isolated’. ‘True generalized’ macrodontia in which all teeth in the dentition are larger than normal may be associated with certain conditions such as Klinefelter's syndrome or pituitary gigantism.2,3 ‘Relative generalized’ macrodontia refers to the presence of normal or slightly larger than normal teeth in relatively smaller jaws.2 The term ‘isolated’ macrodontia describes the situation in which individual teeth are larger than those of the normal series.
The incidence of ‘isolated’ macrodontia affecting the permanent dentition has been reported to be 0.9–2%, with a slightly higher prevalence in males.4 However, the incidence of macrodontia of the mandibular second premolars has not been reported to date.
Macrodontia of the mandibular second premolars may present unilaterally5,6,7 or bilaterally.1,3,8,9,10,11,12,13 The altered occlusal morphology in such cases appears to be quite distinct with large, multitubercular, molariform crowns being observed.12 Dugmore3 has previously suggested the separate categorization of such premolar macrodontia describing affected teeth as ‘macrodont molariform premolars’.
The aetiology of macrodontia remains unknown; genetic and environmental causes have been proposed. Kyriazidou et al13 suggested an autosomal dominant inheritance pattern, illustrating this with a report of bilateral macrodontia of mandibular second premolar teeth in a father and son. It has been suggested that macrodontia may result from an increased vascularity of the tissues in the area of tooth development at the time of cellular initiation-proliferation of the tooth bud.14
Case report
A medically fit 14-year-old boy was referred by his general dental practitioner to the Paediatric Dental Department at King's College Hospital, for the management of his unerupted LL5. No history of dental trauma or family history of dental anomalies was identified.
Clinical examination (Figures 1–3) revealed that the patient was in the permanent dentition with a high-arched palate. He had a Class I incisor relationship on a Class I skeletal base. The molar relationship bilaterally was Class I. Both the overjet and overbite were within the normal range. Oral hygiene was noted to be poor with generalized marginal gingivitis. Multiple carious lesions were identified. The UR1, UL1 appeared tapered and hypomineralized and the UR2, UL2 had talon cusps on their palatal surfaces.
Interestingly, the macrodont LR5 had erupted into a functional position, but the LL5 was partially erupted and only just visible in the mouth. The LL4 had tipped distally, whilst the LL6 was noted to be mesially inclined, resulting in space loss in this region (Figure 3). The LR5 measured 10.5 mm mesio-distally and 7.0 mm buccolingually.
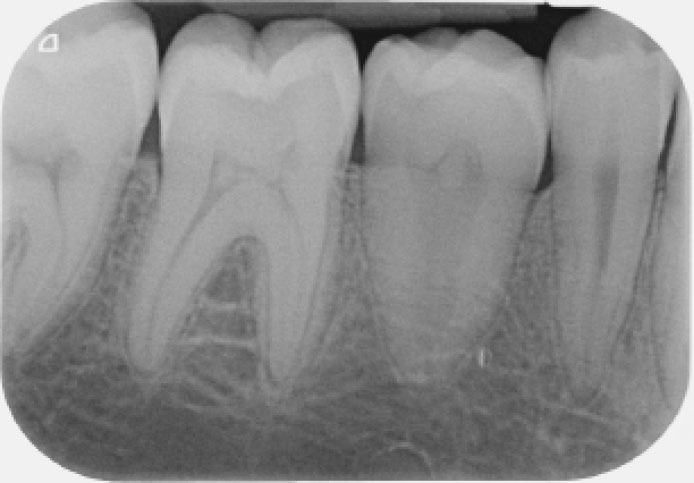
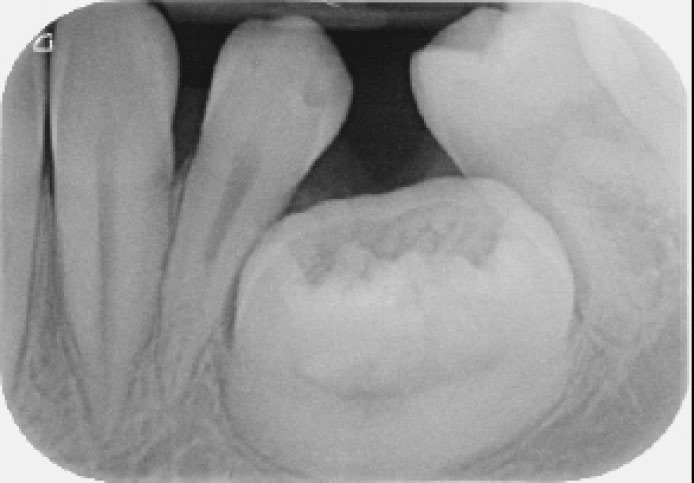
Radiographic examination (Figures 4–6) revealed that all the permanent teeth were present. The unerupted macrodont LL5 had a molariform crown, increased size and abnormal root morphology. The LR5 was larger in comparison to the other teeth but was noted to have normal dental morphology and a pulp stone. The UR7, UR6, UL6, UL7, LL7, LR7 were also noted to have pulp stones and pulp canal obliteration affected UR7, UR6, UL6, UL7.
Figure 4. Orthopantomogram.Figure 5. Periapical radiograph of macrodont LR5.Figure 6. Periapical radiograph of macrodont LL5.
Following a multidisciplinary discussion between colleagues in Paediatric Dentistry, Orthodontics and Oral Surgery, a cone-beam computed tomography (CBCT) scan was requested to aid treatment planning. This imaging (Figure 7) confirmed that the LL5 was vertically impacted, lingually placed and in contact with the adjacent LL4 and LL6, although there was no evidence of root resorption of these teeth. The LL5 was large (19 x 16 x 11 mm) with abnormal crown and root morphology and had an open root apex, supporting the diagnosis of a macrodont.
Figure 7. Cone-beam CT image of macrodont LL5.
Initial management involved the establishment of a rigorous preventive regimen to address the patient's poor oral hygiene and high caries risk. This included the prescription of 2800 ppm fluoride toothpaste and three monthly 2.26% sodium fluoride varnish applications. The carious teeth were restored and the UR2, UL2 and LR5 were fissure sealed.
As the LL5 was partially erupted it was considered to be at high risk of developing caries. There was also a concern that, if left in situ, this tooth could resorb and compromise the health of the adjacent teeth. Although it was appreciated that surgical removal of the macrodont was likely to result in the creation of a significant bony defect, it was decided that, on balance, this was the treatment option that would produce the most stable long-term result for this patient. The patient was not keen to undergo complex treatment.
The macrodont LL5 was surgically removed via a buccal mucoperiosteal flap under a short day-case general anaesthetic. Following the surgical exposure of this tooth, the crown was observed to have multiple cusps, irregular fissures and cratering (Figure 8). It was then divided, constituent pieces removed, the wound debrided and mucoperiosteal flap closed.
Figure 8. Macrodont LL5 surgically exposed.
The patient was reviewed three and six months after the extraction. He reported no pain or altered sensation and examination revealed that the soft tissues had healed well (Figure 9). The presence of a bony defect at the site of surgery was evident, as predicted. This and the inclination of the adjacent teeth made restoration challenging without further complex restorative, orthodontic and surgical treatment.
Figure 9. Post surgical extraction. Left buccal segment view.
The patient was unconcerned about the residual spacing in the mandibular left quadrant and the absence of a tooth caused little aesthetic compromise. He was neither suitable for orthodontic treatment nor interested in having the space restored. He reported experiencing no difficulty in keeping this area clean.
Discussion
Macrodontia of the mandibular second premolars is rare. It has previously been reported in children between 8–14 years of age.9 This, however, is the first case to be reported in which isolated bilateral macrodontia of the mandibular second premolars is associated with numerous other dental anomalies. These include talon cusps, pulp stones, pulp canal obliteration, hypomineralization and tapering of the central incisors.
Other cases in which patients have presented with multiple dental anomalies have been reported in the literature4,11,15,16,17 but none with the combination of abnormalities presented here. Pereira et al17 reported a macrodont incisor with a talon cusp and dens invaginatus. Another case report describes molarization of the mandibular second premolars with concurrent dentine dysplasia.11 This case described abnormal pulp morphology of the mandibular second premolars, which had short, conical roots and pulp canal obliteration affecting only these teeth.
Some dental anomalies are known to be associated with each other. Brook proposed a multifactorial model to explain the associations between hypodontia and microdontia and also macrodontia and supernumerary teeth, suggesting a continuous scale related to tooth number and size.18 To our knowledge no previous publication has described an association between the dental anomalies presented in this case.
Garib and Peck19 and Chate20 investigated mandibular premolars with tooth shape deviation (MnP-TSD). MnPTSD is characterized by a constriction in the facio-lingual diameter and elongation in the mesio-distal width when compared with normal mandibular premolars. Both authors describe the use of a mesio-distal/facio-lingual (MD/FL) index and the calculation of occlusal-crown area (MD x FL) to diagnose MnPTSD. Mandibular second premolars with 'normal' morphology are defined as having a MD/FL index of less than 90 and a mean crown area of 60.4 mm.2,21 Use of these measurements to differentiate MnP-TSD from macrodont premolar teeth was proposed because, whilst in both conditions, the MD/FL indices exceed 100, only macrodont premolars have increased occlusal areas. The MD/FL indices for LR5, LL5 in the case reported here were 150 and 119, respectively, whilst their occlusal crown areas were 73.5 and 304, respectively. Since the MD/FL of both teeth was greater than 90 and the mean crown area of both exceeds 60.4, LR5 and LL5 may both be categorized as macrodont teeth.
In the management of this case the use of CBCT scanning in addition to conventional radiography allowed the macrodont to be accurately located and its morphology and relationship to vital adjacent structures (including the inferior dental canal and mental foramen) was appreciated in three dimensions. This allowed better surgical planning for the procedure to be completed in the safest and most effective manner.
Comprehensive assessment and treatment planning are vital in cases involving the management of macrodont teeth. Such teeth often present with morphological anomalies that can predispose them to becoming carious3 If these teeth do erupt, the application of fissure sealant is recommended.13 The large crown size of macrodonts may also cause aesthetic and crowding issues. These teeth often fail to erupt due to impaction which results in disruption of the developing occlusion.3 The additional space required to accommodate larger macrodont teeth can have an adverse effect either on the positioning or alignment of adjacent teeth and those elsewhere in the dental arch.20
The surgical removal of macrodont teeth is often necessary to prevent the development of associated pathology (including caries) and to enable the orthodontic alignment of other teeth. This can be challenging and the best possible outcome is facilitated by appropriate imaging and surgical planning. Prosthetic replacement of macrodont teeth may be complicated by residual alveolar defects following surgery and non-anatomical spacing.
This case highlights the value of a multidisciplinary approach to the management of dental anomalies. The contribution of expertise from paediatric dentists, orthodontists and oral surgeons to the treatment planning of this complex case ensured an optimal patient outcome.
Conclusion
This report describes a rare case and management of bilateral macrodontia of the mandibular second premolar teeth associated with other additional dental anomalies, including talon cusps, pulp stones, pulp canal obliteration, hypomineralization and tapered central incisors.