Children's dentistry in secondary care during COVID-19 Kunal B Patel Franchesca Fong Ravinder Kaur Janet Davies Rosemary Whatling Dental Update 2025 47:8, 652-661.
Authors
Kunal BPatel
BDS, MJDF, MPaedDent RCSEd
Specialist in Paediatric Dentistry, The Royal London Dental Hospital, Barts Health NHS Trust; Honorary Clinical Lecturer in Paediatric Dentistry, Queen Mary University of London
Consultant in Paediatric Dentistry, The Royal London Dental Hospital, Barts Health NHS Trust Honorary; Clinical Lecturer in Paediatric Dentistry, Queen Mary University of London
Consultant in Paediatric Dentistry, The Royal London Dental Hospital, Barts Health NHS Trust Honorary; Clinical Lecturer in Paediatric Dentistry, Queen Mary University of London
Honorary Consultant in Paediatric Dentistry, The Royal London Dental Hospital, Barts Health NHS Trust; Senior Lecturer in Paediatric Dentistry, Queen Mary University of London
The COVID-19 pandemic has brought a unique set of challenges to assessing and treating paediatric dental patients in the secondary care setting. These children often present with high disease burdens and high levels of anxiety. In addition, they may have medical conditions which add to their treatment complexity. At the Royal London Dental Hospital, innovations have been put in place to improve the patient journey in a time where access to both out-patient and general anaesthetic services have been severely limited. Long term these innovations will help us to improve our service and facilitate communication with patients/carers, general dental and medical practitioners, safeguarding and specialist medical teams. It will create more flexible and creative work patterns for the dental team.
CPD/Clinical Relevance: This paper illustrates the innovations that were introduced to overcome the challenges faced during the COVID-19 pandemic.
Article
With COVID-19, the past few months have brought about challenges that are unique to the management of paediatric dental patients. This has led to the adaptation of paediatric dental services across the country and inspired innovations to facilitate the continuity of emergency and elective procedures. At the Royal London Dental Hospital, Barts Health NHS Trust, some of these innovations will have a lasting impact and can be utilized going forward into the recovery phases and beyond.
Challenges
Outpatient activity
We receive approximately 5,000 referrals and undertake 15,000 outpatient appointments in the Paediatric Dental department annually. The COVID-19 pandemic has temporarily halted elective face-to-face dental assessments and procedures. This resulted in a precarious situation of having a large backlog of patients requiring dental assessment and treatment.
Dental anxiety is prevalent for many children accessing dental care. Changes in our environment, such as having to wear personal protective equipment (PPE), can enhance children's anxiety further.
Reduced access to general anaesthetic
The reduced provision of general anaesthetic (GA) services following the cancellation of all elective procedures has had a profound effect on our service. Dental caries accounts for a large proportion of general anaesthetic admissions for children in the UK. In 2015-16, tooth decay was the most common reason for hospital admission for children aged 5 to 9 years-old and the sixth most common procedure in hospital for children aged 4 years and under.1 London alone has a combined waiting list of over 3000 children awaiting dental procedures under GA. The children presenting to our service are largely pre-cooperative, have special care needs or are medically compromised. Our current waiting list of over 700 patients has been exacerbated by new emergency cases requiring dental treatment under GA. General anaesthetic services across the United Kingdom are still limited for many paediatric dental units, who are competing for theatre access with other surgical specialties and are operating with a significantly reduced patient flow.
Staffing and space restrictions
We have faced multiple challenges with the availability of our paediatric dental workforce. Three-quarters of our team were unavailable for a variety of reasons. They were either: redeployed to COVID-19 wards and maternity services; self-isolating; shielding; ill themselves; caring for family members who were ill; sadly affected by family bereavements; diverted to University online teaching; or had childcare difficulties owing to nurseries closing, loss of help from shielding grandparents and respite services for children with special educational needs. The result of which was a large proportion of motivated staff being unable to contribute to clinical activity at a time when we needed them most. The remaining patient-facing staff were limited by availability of appropriate PPE and fit testing as this was rightly diverted to the COVID-19 wards.
Our open plan clinical space was re-allocated to the transfusion service. We moved location twice, to areas with reduced capacity, utilizing side surgeries to comply with health and safety concerns. Open plan administrative spaces were re-organized to maintain social distancing.
Innovations
With families, prior to the pandemic, routinely waiting 40 weeks for a Consultant Clinic appointment, we felt that we had to continue to provide this service. Following the implementation of lockdown, swift action of our department's senior team enabled the maintenance of emergency care and outpatient activity through utilization of the paediatric dental team both on and off site. This took place through several innovative changes to our daily practice.
Maintaining children's dental emergency services
Prior to COVID-19, we ran a busy children's walk-in dental emergency service. Once lockdown was enforced, we adapted our services to provide a dedicated telephone line for new and existing patients to contact us for emergency triaging. Subsequently, we were approached by commissioners to expand and become a 111 dental emergency hub. During the lockdown period, we provided emergency provision to over 850 paediatric patients. Many parents were distressed due to difficulties in finding dental care during the pandemic. Patients presented from across London and beyond for a variety of reasons including pain, oral lesions, swellings and trauma. Our continued use of inhalation sedation minimized the need for GA and contributed to successful outcomes. Our website was regularly updated with information on how patients could access our service. The feedback from grateful parents has been overwhelming (Figure 1).
Figure 1. Quotes from grateful parents.
Safeguarding vulnerable patients
An important part of our role as paediatric dentists is to identify vulnerable children. We were alert to the increased risk of non-accidental injury manifesting as dental injuries, with families under stress in lockdown. Our team identified safeguarding cases requiring involvement of the appropriate services. We have always considered face-to-face consultations as best practice to identify safeguarding concerns. The advent of our new video clinics (discussed later) enabled us to observe the care-giver/child interactions as well as possible, including physical signs of injury, compared to telephone consults, but only when there was a need.
Preparing paediatric patients
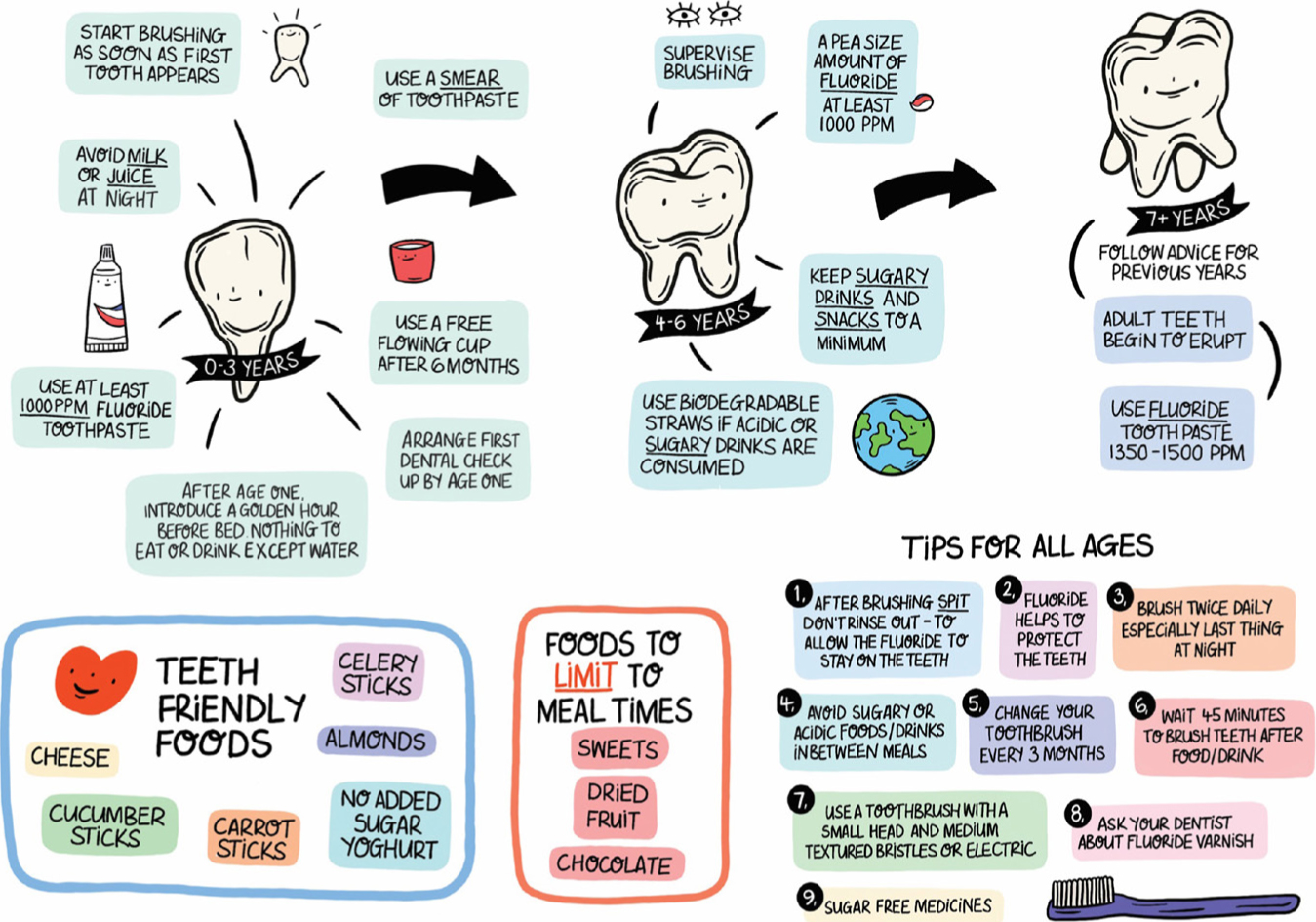
Prior to a child attending our service for a procedure, the treating clinician conducts a telephone or video consultation to obtain first stage consent and explains the procedure to the child in age appropriate language. To manage patient and carer anxiety and promote good oral health, we have created a range of resources that can be emailed to patients prior to their appointment. This includes: a ‘Going to the dentist leaflet’ (Figure 2) showing a storyboard of clinicians donning ‘superhero’ PPE outfits; and a ‘Diet and brushing guide leaflet’ (Figure 3) which provides prevention advice in a child friendly way.
Figure 2. Child friendly leaflet illustrating PPE worn by staff.Figure 3. Illustrated prevention advice leaflet for children.
We also commissioned a video to welcome patients and parents back to help allay any anxiety about attending the hospital. It highlights the measures taken to minimize COVID-19 transmission (Figure 4). The link for this video is sent out for the patient and carer to watch on their device so that they are aware of what to expect prior to arriving (https://www.youtube.com/watch?v=x_vfn8GUVfI).
Figure 4. Still taken from video welcoming patients back to the Paediatric Dental department.
Adapting personal protective equipment for children
Our play specialist team customized our visors with superhero or cartoon characters to make clinicians and nursing staff look more approachable whilst in PPE (Figure 5). We have had positive verbal feedback from patients and parents and the children love choosing which cartoon character will undertake their dental treatment. When the spaceman is selected the dentists enjoy pretending to walk and move in zero gravity to make the children giggle and feel relaxed.
Figure 5. Child friendly visor customization.
PPE prevents our body language and facial expression to be used to our advantage. In order to make the experience more personable, we created laminated name badges with each clinician's photograph (Figure 6). These were attached to the apron so that patients could see what each clinician looked like under their ‘superhero’ PPE.
Figure 6. Child friendly PPE with photo-badges showing clinicians' faces.
GA categorization
General anaesthetic services are a scarce resource in the current climate. We categorized our 700 general anaesthetic patients against the adapted surgical prioritization guidance document.2 The list of high priority patients was put forward to the theatre service managers highlighting the paediatric dental cohort within the surgical specialties.
The highest need patients were allocated the first GA appointments in May 2020. All paediatric surgical specialties are vying for theatre space. There are a reduced number of paediatric theatres available as teams await the return of redeployed staff, particularly operating department practitioners (ODPs). Our dental theatre sessions have reduced from 9 to, on average, 3 per week. Since August 2020 this has increased to 6 GA sessions per week.
The number of patients being treated per theatre session has been halved. COVID-19 checks for patients and their sole accompanying parent, prior to entering the hospital and ward, all add time to pre-clerking. The ventilation of the operating theatre determines the number of patients that can be treated and patient flow. Patient induction is now carried out in the theatre rather than the separate anaesthetic induction room. This reduces exposure of COVID-19 to the wider team after an AGP. Donning and doffing of PPE for AGPs also add time.
We are emailing surgical elective procedure information prior to their GA to answer questions they may have regarding hospital attendance for their operation.3
Adult surgical specialties have reported high levels of patients declining their GA procedures owing to anxieties regarding hospital attendance during the pandemic. Up to 85% refusal has been reported in our Trust. This is understandable given that our hospital is London's largest NHS Trust and has been regularly featured as a high profile COVID-19 centre in the media. At the peak of the pandemic, on 8 April 2020, the Trust was treating 616 COVID-19 positive patients. By early June, 621 patients with COVID-19, including 4 Trust staff, had died but 2000 lives had been saved.4 Since our paediatric dental GA services resumed in May, no families have refused their GA appointments, such has been the dental discomfort of their children. For one family, whose child suffered from congenital neutropenia, the GA appointment was the first time they had left their house since the onset of lockdown. Informing parents of their child's dental operation has been one of the few pleasurable tasks of the pandemic as they are so grateful to receive the news, such has been their desperation.
Immediate transition to electronic record keeping
Prior to the COVID-19 pandemic, Barts Health NHS Trust were advancing their digitization programme, but dental were behind. The creation of specialty-specific templates on Cerner Millennium software to facilitate emergency, new patient, review and joint clinics enabled all prospective record-keeping to become electronic overnight at the start of the pandemic. Previous written clinical entries were digitized and uploaded to the patient's electronic record, where required.
Our knowledge and utilization of this software system has skyrocketed. This has had multiple benefits, including:
The improvement of cross-infection control by removing paper records from the clinical environment;
Enabling staff members to carry out clinical duties from home;
Aiding communication through interdepartmental referrals; and
Communication with medical colleagues, the safeguarding team and our anaesthetists as part of our pre-assessment policy.
Access to the East London Patient Record (ELPR), which links our medical records system to other care systems, including General Medical Practitioner (GP) surgery records and social care records, has been particularly useful in obtaining complex medical histories prior to GA and flagging safeguarding cases. Geographical expansion of the ELPR at the height of the pandemic linked more hospitals and GPs across London. This helped to obtain and share vital information rapidly and reduced the need to chase correspondence.
There is a decreased burden on the medical records administrative staff moving notes between sites. The transition has meant that missing notes are now a thing of the past. The longer-term environmental impact is a reduction in paper usage.
General dental practitioners have transitioned over to NHS.net email accounts and future implications of this include electronic clinic letters being formulated from the patient's record and sent via secure email in a time efficient manner.
Electronic notes and power forms facilitate data collection for research, service evaluation and quality improvement programmes in a timely manner. For example, data collected from our new electronic trauma clinic forms can be utilized in research projects; the diagnostic data will be linked with the treatment modalities and outcomes.
Introduction of telephone and video assessments clinics
The use of technology to triage and assess patients remotely has reduced face-to-face patient contact. Remote telephone clinics, in conjunction with language translation services, have been running since the beginning of lockdown, with carers sending relevant photographs that are uploaded onto the patient's record (Table 1). Patients assessed and accepted via our telephone emergency clinics are then allocated emergency treatment appointments if required.
Smart phone camera quality is often better and is easier for parents to position nearer the mouth than a laptop.
Parents are asked to mark ‘R’ for right and ‘L’ for left on the child's face with a felt tip pen or eyeliner to avoid problems of interpretation. If preferred, the markings can be drawn on a plaster attached to the child's face (Figure 7).
Spoons can be used to obtain better photographs (Figure 8). Cheek retractors from the boardgame ‘Speak Out’ can help with pictures (Figures 9a and b).
A family took photos of their toddler's traumatized teeth during his afternoon nap.
Figure 7. Example of utilizing plasters to mark the patient's right and left side of face.Figure 8. The use of spoons to aid cheek retraction during video consultation.Figure 9.
(a) The use of ‘Speak Out’ cheek retractors to aid remote assessment. (b) The use of ‘Speak Out’ cheek retractors to aid remote assessment (close up).
Using the ‘Attend Anywhere’ portal for video consultations has improved remote clinical examinations. This platform allows invitation of other members of staff, such as trust advocates, when there is a language barrier. This invitation option can also be utilized by our junior staff to obtain a second opinion from a specialist or consultant. We can utilize the ‘share screen’ function to show patients their radiographs during a remote review consultation.
Clinical photographs can be obtained during the video consultation, with consent, using the ‘screenshot’ function and can be uploaded to the patient's record. The photographs saved represent a potential resource for teaching. Families have reported how grateful they are that we have kept their appointment, avoiding travel whilst their anxieties regarding public transport were high. We have reduced the burden of care, particularly for families of low income, those geographically far from the hospital and vulnerable patients, for example those with leukaemia. Parents and carers of children with autism have benefited from dental assessment whilst in their own familiar surroundings. The future value of remote telephone or video services includes assessment of those unable to travel or those requiring interdisciplinary opinions. This is particularly relevant due to the paucity and geographic inequity of paediatric dentistry specialists.5
We have identified limitations of this service with patients that have hearing difficulties, visual impairments, or those not confident with technology. There have been some connectivity issues dependent on a user's internet speed. An online feedback form helps improve and tailor our services. Positive comments from parents highlight the benefit of our video clinics (Figure 10).
Figure 10. Positive comments from parents highlight the benefit of our video clinics
We have completed over 780 remote new patient assessments in the Paediatric Dental department since the beginning of lockdown and have safely discharged 12% of these. To reduce the time spent in the dental hospital, the remaining 88% have been allocated to specific patient care pathways, for example pre-assessment general anaesthetic clinics. Future new patient and review clinics can be held remotely to minimize onsite patient interaction, improve patient flow and increase clinical space for treatment.
Positive impact of working from home on workforce availability
We have worked closely with our IT teams to activate remote access. This has included setting up a secure virtual private network, virtual smartcard access and providing headsets and webcams to staff. Remote access has enabled those shielding to continue effectively contributing to patient care. We have continued routine paediatric dental services, both on and off site, and have rotated staff returning from redeployment into the ‘working from home team’ to help maintain social distancing in the dental hospital. Future value of this includes flexible working patterns for those with childcare or carer responsibilities, and preparedness for changes to service provision. This allows us to concentrate on AGPs under LA, sedation and GA on site whilst emergency triage, consultant clinic assessments and preventive advice can be provided remotely.
Twice daily virtual team meetings were held to ensure effective communication and handovers for staff working on different days, both on and off site. Discussions of complex cases, safeguarding issues, dissemination of guidance and clinical information was also undertaken. Our team is largely comprised of part-time workers with school-aged children. Allowing staff to run clinics from home has increased their flexibility to spread working hours over more days and fit with school opening hours. This has positive implications for a specialty plagued by workforce issues and long waiting lists, particularly when chair space is at a premium.
Conclusions
Facing the challenges and adapting our service early in the pandemic has enabled our department to continue to provide essential specialist care and be well placed for the reopening of routine dental services. The innovations have ensured continued good communication with new and existing patients throughout the COVID-19 pandemic, whilst maintaining a safe and adaptable working environment for staff.