Meningococcal septicaemia is an acute bacterial infection with high morbidity and mortality. The infection can cause multiple systemic manifestations including disseminated intravascular coagulation, haemorrhage, infarction and necrosis of internal organs and bone abnormalities. Children with meningococcal septicaemia present most frequently between the ages of 3 months and 5 years; a crucial period for the developing dentition. Disturbances to developing dentition are frequent sequelae of this infection and include hypoplasia and hypo/hypermineralization, failed or delayed eruption, root and crown malformation. This is thought to be related to subclinical premaxillary osteomyelitis secondary to septicaemia. This case series describes three patients with rare but similar patterns of dental development, notably in the anterior maxillary region, following meningococcal septicaemia in early childhood. The patient journey through multidisciplinary assessment and management is explored, from initial diagnosis to definitive oral rehabilitation. This article underscores the importance of effective communication and care pathways between the dental team and wider medical profession.
CPD/Clinical Relevance: To raise awareness of the impact of early childhood meningococcal septicaemia on the developing dentition and the potential need for referral to secondary dental care.
Article
Meningococcal disease presents in two forms: bacterial meningitis and septicaemia, where septicaemia accounts for approximately 25% of cases.1Neisseria meningitides, Streptococcus pneumoniae and Haemophilus influenzae type b are the leading cause of bacterial meningitis in children over 3 years of age and young adults. Paediatric patients typically present with meningococcal septicaemia between the ages of 3 months and 5 years. The incidence in infants is 16 per 100,000 and in children aged 1–4 years, this figure is 4 per 100,000.2 The infection has a high morbidity and mortality rate. Up to 20% of the children who contract severe meningococcal septicaemia die, usually within 24 hours of the first symptoms.
The infecting organisms are members of the healthy microbiome, found in the human nasopharynx and are spread via close contact, including saliva and respiratory secretions.
Complications of infection can present in multiple systemic manifestations. This can include non-specific symptoms, such as general malaise, fever, nausea and respiratory problems, in addition to signs of septic shock and classic purpuric non-blanching rash. Specific symptoms include altered mental state, hypocalcaemia, disseminated intravascular coagulation (DIC), haemorrhage, infarction and necrosis of internal organs and bone abnormalities. Consequently, children are left with hearing impairments, sensory disabilities, neurological damage (including epilepsy), chronic organ damage as well as psychiatric and behavioural difficulties. DIC can cause occlusion of blood vessels and microthrombi that lead to fasciitis, necrosis of the limbs and truck resulting in widespread scarring and the need for limb and digit amputation.
Dental disturbances are frequent sequalae of the infection and described by Walton et al as '…severe upset in odontogenesis with arrested development and bony repair…'.3 Developmental abnormalities include; hypoplasia and hypo/hypermineralization of teeth, failed or delayed eruption, root and crown malformation.
The correlation between infection and odontogenic abnormalities can be due to the timing of infection and calcification of the maxillary permanent incisors between the ages of 3 and 12 months and the complete development of maxillary deciduous incisors in the first 18 months. There is a suggested association between reduction in blood supply to the premaxilla as a result of DIC in the acute phase of the infection resulting in 'subclinical premaxillary osteomyelitis that resulted in a severe upset in odontogenesis'.2 Walton et al were unable provide an explanation for increased susceptibility of the premaxillary region compared with the posterior mandibular region, where reduced vascular supply is known to cause osteomyelitis.3 Faibis et al discussed the relationship between coagulation and DIC, which may cause infarction and reduce blood supply to the smaller vessels of the premaxilla, resulting in death of osteoblasts and odontogenic cells. The maxillary anterior region is thought to be affected similarly to that of the limb extremities.4
Patients are referred to secondary care between 6 and 7 years of age with concern about failure of eruption and poor-quality tooth tissue of aesthetic concern related to the maxillary anterior incisors. This can be of significant impact to the psychosocial wellbeing of the child as they mature into teenage years: it is known hypodontia negatively affects oral health-related quality of life (OHRQoL)5 and that having missing teeth is a predictor of emotional distress.6 The dental effects of meningococcal septicaemia can result in a child developing issues with self-esteem, socialization, formation of interpersonal relationships and friendships at a crucial time for social development.
Meningococcal septicaemia is rare; however, the cases presented here demonstrate similar impacts on the developing dentition at similar ages. Treatment for the patients was planned by a multidisciplinary team that included paediatric dentists, orthodontists and restorative dentists.
Case report 1
ELB is a female patient referred by orthopaedics at the age of 7 years for discolouration and was symptomatic with sensitive lower anterior central incisors. ELB had meningococcal septicaemia aged 13 months. She developed a small leg abnormality, nonfunctioning spleen and unusual bowel construction and underwent multiple surgeries under general anaesthetic.
Effects on dental development:
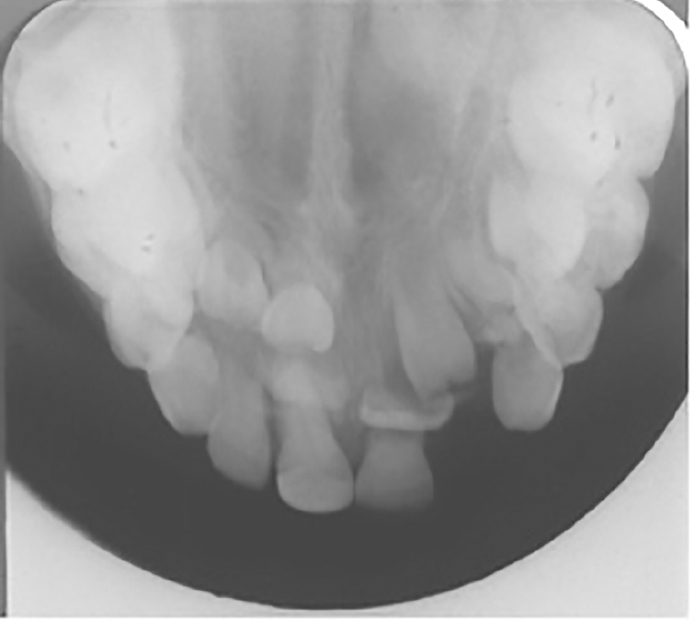
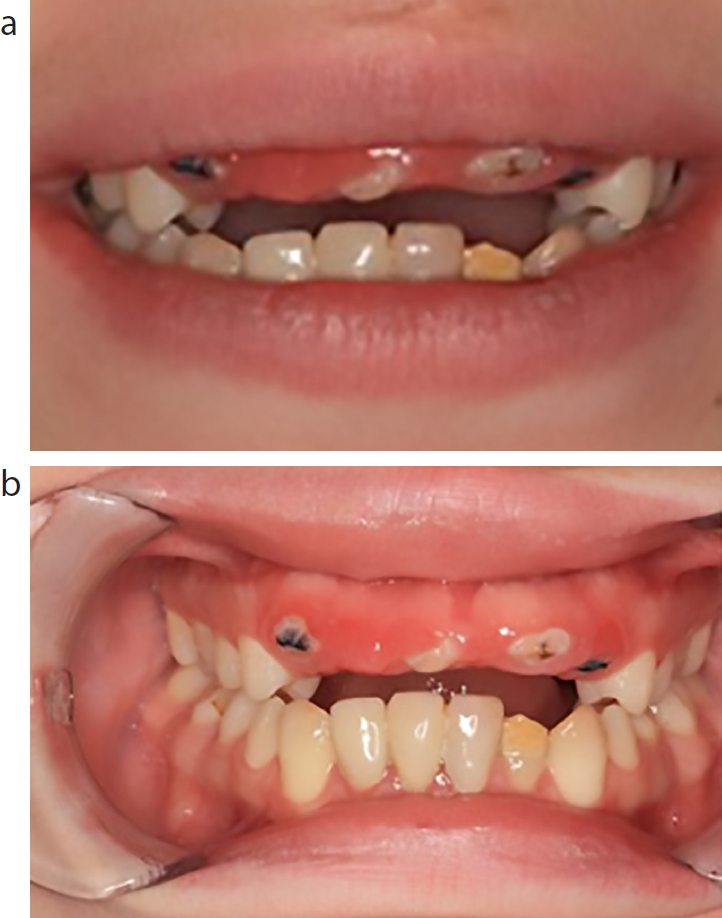
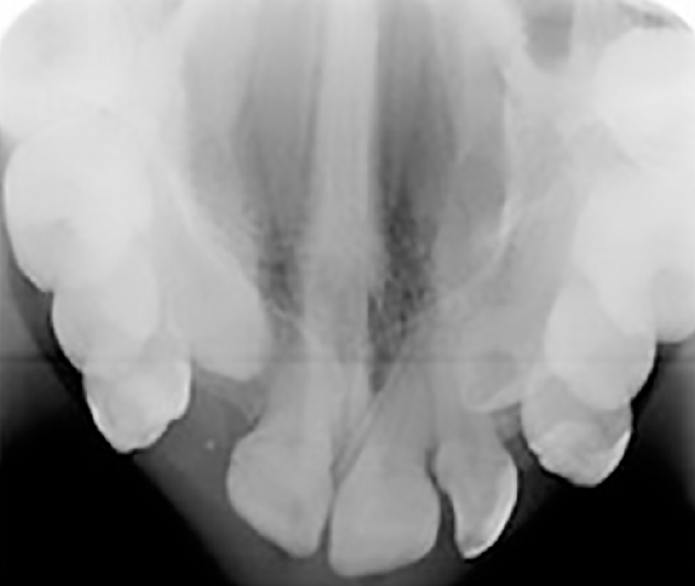
The maxillary anterior region was predominantly affected both odontogenically and in terms of alveolar bone volume. ELB had multiple poorly mineralized, partially formed and unerupted teeth in both primary and permanent dentition in both maxilla and mandible. In the primary dentition, both upper central incisors had a poor aesthetic appearance with yellow discolouration. In the permanent dentition, enamel hypoplasia was present on LR1, LR2, LL1, LL2 and lower first molars. Radiographic examination showed gross root disturbances to both upper permanent central incisors, UR2 remained unerupted while clinically, UR3, UR1, UL2, UL3 were partially erupted with hypoplastic features (Figures 1 and 2). UL3 had a microdontic appearance associated with a thin and narrow root, and LL5 was hypodontic. Clinically, UR1 remained mobile, UL1 exfoliated due to poor root formation and UR2 remained unerupted (Figure 3).
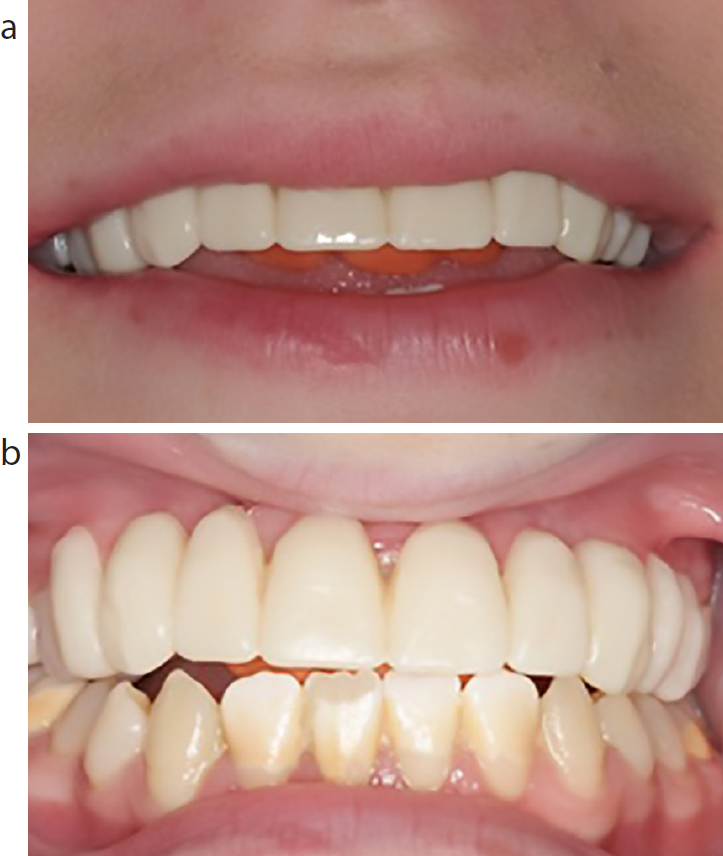
Figure 1. Upper occlusal radiograph showing poorly formed UR3, UR2, UR1 and UL3.Figure 2. (a, b) Patient aged 18 years. Shows poorly formed and partial erupted upper maxillary teeth and hypoplastic lower left lateral incisor.Figure 3. OPG depicts poor root formation of maxillary anterior teeth and presence of lower left retained decidious molar tooth.
Treatment completed
Initial treatment at age 7 included lab-made composite veneers for LR1, LR2, LL1 and LL2 to reduce sensitivity and improve aesthetics. The retained primary maxillary incisor teeth (URB–ULB) were deemed to be the cause of impaired eruption around age 10 years and were, therefore, extracted under sedation and an upper removable prosthesis with posterior bite plane was made to replace UR123–UL123 (Figure 4). ELB was regularly reviewed and underwent routine prevention and restorations.
Figure 4. (a, b) Shows upper removable denture replacing UR123–UL123 and LL2 lost veneer showing hypoplastic appearance.
Following radiographic and clinical examination at multispeciality clinic, aged 19, the decision was made to extract the unerupted anterior maxillary teeth due to their poor-quality crown and root structure being inappropriate for exposure and orthodontic alignment.
Implant funding was granted due to the presence of tooth structure disturbance resulting in acquired tooth loss with mild hypodontia. At age 20, ELB underwent surgery under general anaesthetic for ridge splitting, and augmentation of the anterior maxilla to increase the bone volume in this region for dental implants.
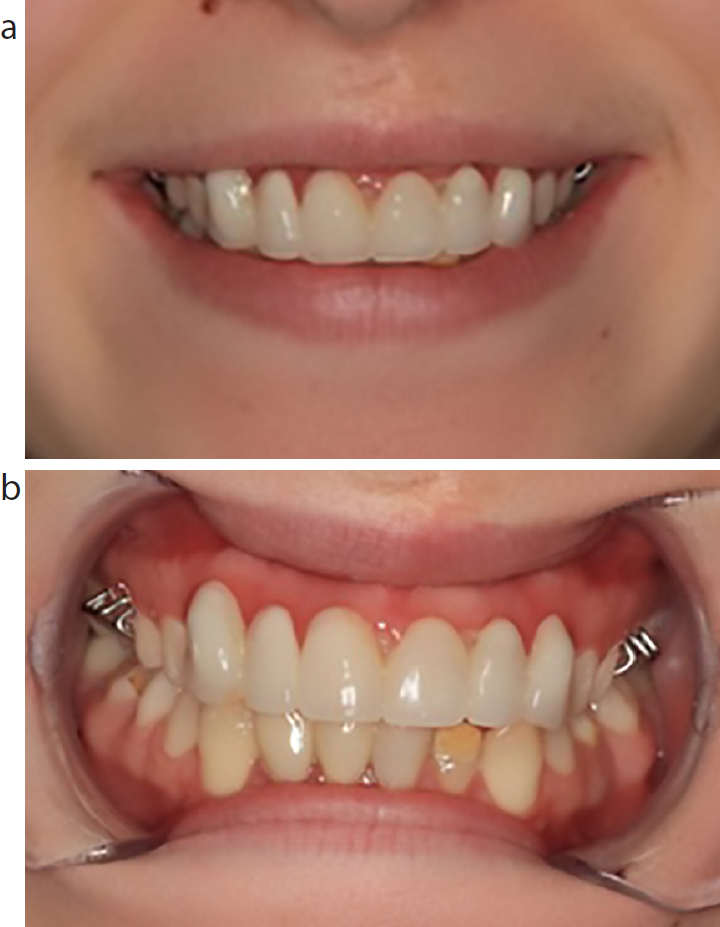
Implants were then placed at age 21, under intravenous sedation in the positions of UR3, UR1, UL1 and UL3. Following soft tissue healing and osteointegration, a screw-retained implant bridge was fitted (Figure 5).
Figure 5. (a, b) Shows implant-retained bridge; UR3 and UL3 are abutment teeth and replacement of lab-made buccal composite veneer on LL2.
Case report 2
MM, a female patient, was referred by her dentist to the orthodontic department at the age of 15 years because of spaced dentition and poor appearance of her front teeth. At the age of 3, she had tibial meningococcal septicaemia and had since undergone toe elongation surgery and skin grafts. Her dental concerns were a possible contributing factor to her depression.
Effects on dental development
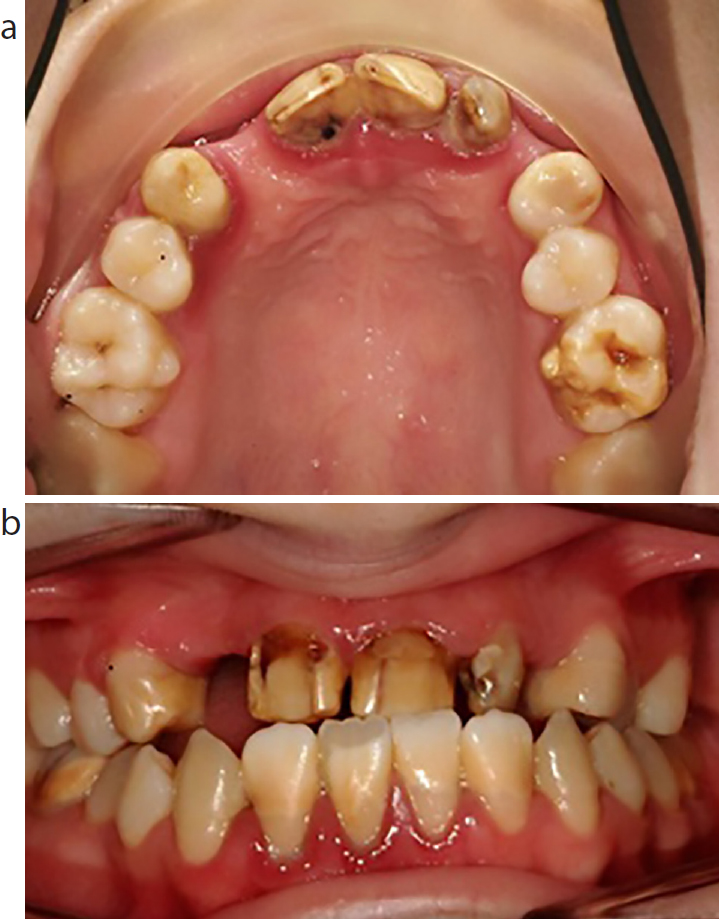
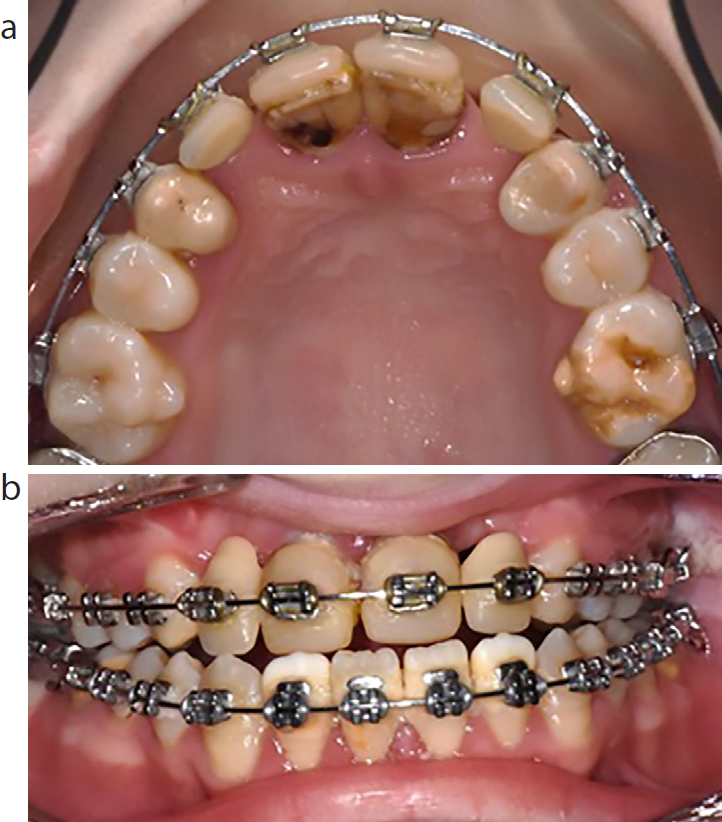
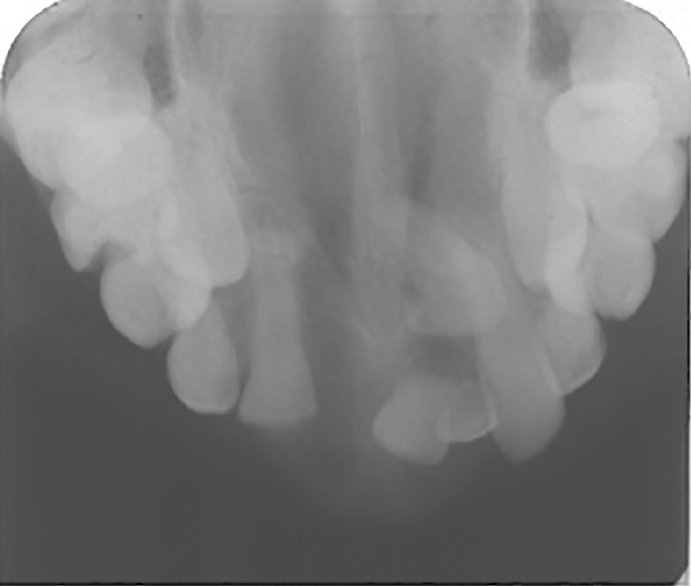
She had developmental enamel hypoplasia involving the permanent upper teeth (UR1234–UL1234) and the tooth surfaces were dark and discoloured (Figure 6). Both upper permanent canines were impacted, ectopic and, radiographically, had shortened roots. UL2 was peg-shaped and lateral; UR2 was horizontally impacted with the presence of an odontome, which was removed prior to the patient presenting.
Figure 6. (a, b) Generalized discolouration and hypomineralization of first molars. Upper canine teeth are impacted and UR2 is absent.
Treatment completed
At the age of 19 years, routine dental restorations had been completed on the hypoplastic UR4, UR2 andUL4. In the following year, composite build-ups were placed (UR1, UL1, UL2) on the maxillary incisors to improve the aesthetic appearance (Figure 7) and aged 20, a snap-on smile was trialled to assess potential aesthetic outcomes of orthodontics combined with orthognathic surgery (Figure 8). This removable prosthesis was also used to improve the appearance of the patient's teeth while she reviewed her options for treatment. There were several options:
Figure 7. (a, b) Stabilization of dentition with anterior composite fillings, OHI and polishing.Figure 8. (a, b) Shows snap on smile in maxillary arch extending from UR6 to UL6.
Continue with a removable prosthesis
Combined approach with extraction of UL2, orthodontic alignment of ectopic UR3, UL3 and UR1, UL1, orthognathic surgery, conventional crowns UL12 and bridge work UR1 abutment, UR2 pontic.
At age 20, she chose the combined approach; however, an attempt to expose and bond the impacted, ectopic upper canines was unsuccessful due to minimal physiological movement. Radiographic examination revealed internal resorption of UL3 and possible resorption of UL2 (Figure 9).
Figure 9. Upper occlusal radiograph showing UL3 internal resorption and coronal radiolucency. UL2 has peg-shaped appearance.
At a joint clinic review at age 21, changes were made to the treatment plan that included extraction of the ectopic UR3, UL3 due to resorption and ankyloses, UL2 due to poor crown form and resorption, and all four wisdom teeth in preparation for bimaxillary osteotomy (Figure 10) for which she is waiting.
Figure 10. (a, b) Mid-orthodontic treatment. Composite restorations bonded to UR1 and UL1 with prosthetic UR2 and UL2 attached to the arch wire.
Following completion of orthodontic and orthognathic surgery definitive restorative treatment will include conventional bridges, abutments UR1, UL1 and pontics UR2, UL2 with resin-retained bridges, abutments UR4, UL4 and UR3 UL3 pontics.
Case report 3
CRLM is a female patient who was referred at the age of 7 years by her dentist for carious primary molars.
CRLM had experienced two episodes of meningococcal septicaemia in close succession aged 13 and 14 months. DIC had caused gangrenous patches on her trunk and limbs, resulting in widespread scarring, amputation of her right ring finger and her other digits had formed short. Growth plate disruption had affected her lower limbs and caused her to stop walking soon after the infection. Her left leg was foreshortened. She has a scoliosis in the spine with a prominent angle at the costochondral junction of the sternum. The meningitis has also caused severe sensory neural loss in mid and high frequencies in both ears resulting in severe hearing loss for which she had worn hearing aids since the age of 15 months. She used sign language to assist with her delayed speech. She had a systolic ejection murmur.
Effects on dental development:
She had microdontia of UR3 and UL2; failure of formation of UR1; UL1 had poor root formation and a hypoplastic crown with failure of eruption; and UR2 had a short crown with hypoplasia (Figure 11).
Figure 11. Case 3: upper occlusal radiograph showing UR2 poorly formed crown and unerupted and poorly formed UL1.
Treatment completed
At age 10, the initial treatment had included restoration of carious lesions in the primary dentition and extraction of unrestorable URD and ULD. Composite build-ups of UR2 with extraction of ULA and ULB, and fabrication of an upper partial denture to replace UR1, UL1, UL2 was completed.
At the age of 15 years, a cobalt– chrome overdenture was fabricated to replace and overlay the upper anterior incisors (UR2–UL1).
At age 20, implant funding was granted for a two-implant, three-unit bridge.
Prior to implant placement, localized autogenous and bovine bone grafts were placed in the UR2 and UL1 regions to augment these areas for implant placement. At age 21, two implants were placed under intravenous sedation in UR2 and UL1 (Figure 12) with cover screws.
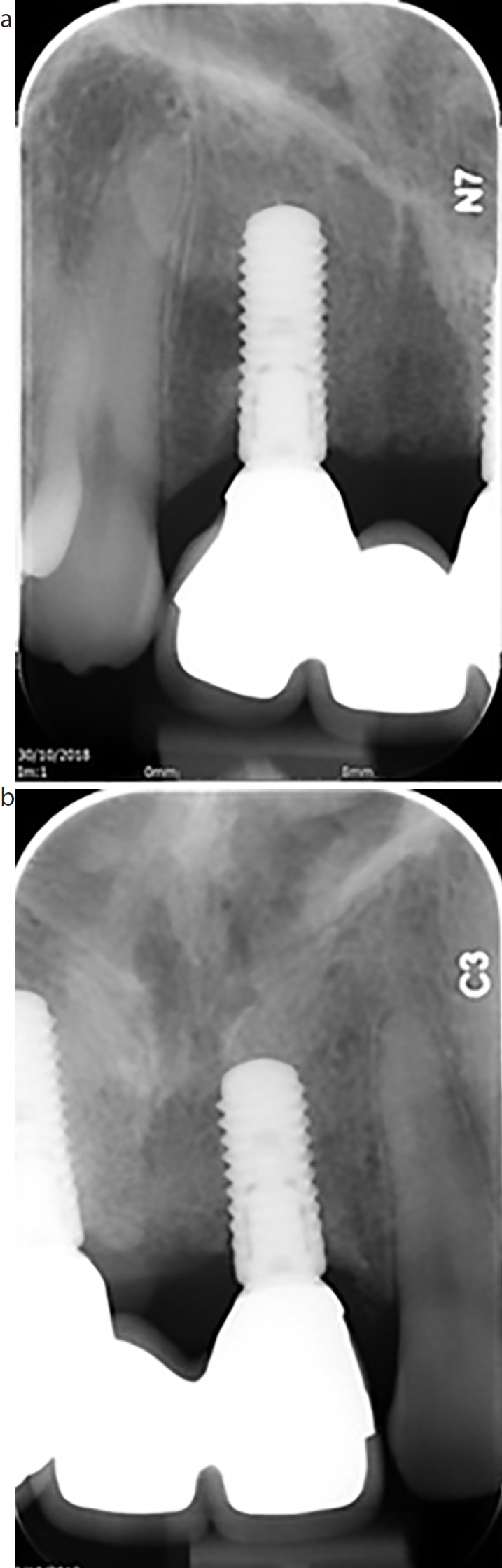
Figure 12. (a, b) Peri-apical radiographs to show implant retained bridge. Implant abutments UR2 and UL1.
Second-stage healing abutments were placed 3 months later. At age 21, the final implant screw-retained bridge replacing UR2, UR1, UL1 was placed. (Figure 13).
Figure 13. Fixed Implant retained bridge, implant abutments UR2 and UL1 and pontic in position of UR1.
Discussion
These three cases reflect the extensive medical complications following meningococcal septicaemia. All three patients had contracted the infection under the age of 3 years and all have a very similar pattern dental developmental abnormality.
It appears that the majority of changes are seen in the anterior maxilla. This area of the mouth is the region that most impacts on a child's facial appearance: it is a child's smile. The adult dentition would normal start eruption around age 6 and so changes in this region affect late childhood into young adolescence. Early identification of dental changes, such as those seen in these cases, can help to camouflage the poor aesthetics while the children/young adults are growing. Maintaining average dental aesthetics is important to allow children/young adults’ normal social development, unrestrained interaction and avoid bullying. Long-term plans can be made for tooth replacement once growth is completed.
There is limited awareness and knowledge of the causes of these profound disruptions of odontogenesis associated with meningococcal septicaemia. The aim of this article is to help ensure that dental and medical professionals are better informed about the dental abnormalities that can be associated with systemic sequelae suffered during tooth development.