Johnson KB, Mol A, Tyndall DA. Extraoral bite-wing radiographs: a universally accepted paradox. J Am Dent Assoc. 2021; 152:444z-447 https://doi.org/10.1016/j.adaj.2021.02.015
Kühnisch J, Anttonen V, Duggal MS Best clinical practice guidance for prescribing dental radiographs in children and adolescents: an EAPD policy document. Eur Arch Paediatr Dent. 2020; 21:375-386 https://doi.org/10.1007/s40368-019-00493-x
Tsiklakis K, Mitsea A, Tsichlaki A, Pandis N. A systematic review of relative indications and contra-indications for prescribing panoramic radiographs in dental paediatric patients. Eur Arch Paediatr Dent. 2020; 21:387-406 https://doi.org/10.1007/s40368-019-00478-w
Felemban OM, Loo CY, Ramesh A. Accuracy of cone-beam computed tomography and extraoral bitewings compared to intraoral bitewings in detection of interproximal caries. J Contemp Dent Pract. 2020; 21:1361-1367
Gander DL. Guidelines for the use of radiographs in clinical orthodontics [book review]. Dentomaxillofac Radiol. 2002; 31
Timms L, Deery C. Do panoramic radiographs offer improved diagnostic accuracy over clinical examination and other radiographic techniques in children?. Evid Based Dent. 2021; 22:110-111 https://doi.org/10.1038/s41432-021-0194-y
Abdinian M, Razavi SM, Faghihian R Accuracy of digital bitewing radiography versus different views of digital panoramic radiography for detection of proximal caries. J Dent (Tehran). 2015; 12:290-297
Kaur H, Gupta H, Dadlani H Delaying intraoral radiographs during the COVID-19 pandemic: a conundrum. Biomed Res Int. 2022; 2022 https://doi.org/10.1155/2022/8432856
Farman AG. There are good reasons for selecting panoramic radiography to replace the intraoral full-mouth series. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:653-654 https://doi.org/10.1067/moe.2002.129766
Clark HC, Curzon ME. A prospective comparison between findings from a clinical examination and results of bitewing and panoramic radiographs for dental caries diagnosis in children. Eur J Paediatr Dent. 2004; 5:203-209
Davis AT, Safi H, Maddison SM. The reduction of dose in paediatric panoramic radiography: the impact of collimator height and programme selection. Dentomaxillofac Radiol. 2015; 44 https://doi.org/10.1259/dmfr.20140223
Wiley D, Yepes JF, Sanders BJ Pediatric phantom dosimetry evaluation of the extraoral bitewing. Pediatr Dent. 2020; 42:41-46
The Use of Extra-oral Bitewing Radiographs for Treatment Planning in Paediatric Patients Bethan Jones Eleanor O'Grady Nicholas Drage Mechelle Collard Dental Update 2025 50:9, 767-770.
Authors
BethanJones
BDS, MFDS (RCSEng)
Dental Core Trainee in Paediatric Dentistry, University Dental Hospital, Cardiff and Vale University Health Board
The extra-oral bitewing is becoming increasingly popular among clinicians to help overcome some of the challenges posed when taking intra-oral radiographs for paediatric patients. When combined with clinical examination, this radiographic view provides important diagnostic information in the management of caries in the posterior dentition. In this article, the use of extra-oral bitewings will be explored. The introduction of a decision tree provides the dental practitioner working in either a primary or secondary care setting, a pathway to assist with deciding the optimal radiographic prescription.
CPD/Clinical Relevance: Extra-oral bitewings can be a useful radiographic tool for dental caries diagnosis in the mixed dentition.
Article
Although there is an inherent contradiction in calling an extra-oral approach a ‘bitewing’, this term best describes the panoramic alternative. The terms ProxiPan and Proxi-optimised radiograph have been suggested; however, the term extra-oral bitewing (EBW) is more widely used, and is the term used in this article.
The European Academy of Paediatric Dentistry (EAPD) advise that any radiographs should be optimised in terms of dose, following the ‘as low as diagnostically achievable being indication-oriented and patient-specific’ principle.2 Indications for radiographs in children include suspected and active caries, dental and facial trauma, pathology of teeth and bone, including infections and abscesses, suspected loss of vitality and developmental abnormalities.3,4 EAPD guidance recommends that an EBW may be considered when a child is unable to tolerate a conventional intra-oral bitewing, whether through disability or sensory discomfort.1,2
Intra-oral bitewings are recommended for assessing caries (proximal and occlusal), existing restorations and bone levels, and give the lowest radiation dosage when compared to extra-oral views.5,6 They are considered the standard of care in assessing caries with the greatest accuracy, and so should be used as such.1,2,6,7,8 However, they can increase the gag reflex, presenting further challenges in uncooperative paediatric patients, leading to improper positioning or re-takes causing re-exposure.4,8,9 EBWs and cone beam computed tomography (CBCT) have been found to be comparable to intra-oral bitewings for assessing proximal caries4,10 and reduce risks in terms of gagging, and also aerosol production during COVID-19.1,9,10 However CBCT is not indicated for routine caries assessment owing to the higher radiation dose and the issue of artefacts arising from metallic restorations.6
Oblique lateral radiographs may be used for caries assessment in patients who are unable to accept intra-oral bitewings and are unable to keep still long enough for panoramic or EBW radiographs. However, it is technique sensitive and requires the use of cassettes. Cassettes are only available for film-based systems and phosphor plate digital systems. Most new panoramic systems in general practice are solid state detector systems11 for which there is no cassette available.
When performing a conventional intra-oral bitewing, the image receptor is placed in the lingual sulcus parallel to the dental arch, and the X-ray beam is aimed perpendicular to the image receptor and the posterior teeth with a slight downward angulation on the beam. The use of an image receptor holder and beam aiming device aids positioning and reduces image faults and re-takes. On the other hand, traditional panoramic radiography produces a tomographic image. Modern panoramic units produce the tomographic layer by using complex synchronized rotations of the X-ray source and image receptor, producing a curved horseshoe shaped tomographic layer that matches the dental arch. Positioning of the jaws within the focal trough is of paramount importance to produce an accurate undistorted image. Even so, overlap of the premolar contact points is common. EBWs are also produced by using tomographic techniques with additional beam collimation. The tomographic movements have been described as using ‘improved orthogonality’. This change in image geometry allows separation of the contact points between the posterior teeth, optimising caries detection, making them comparable to intra-oral imaging.8,12
The literature review findings were discussed at a multidisciplinary team meeting involving paediatric and orthodontic colleagues, which contributed to the development of an EBW decision tree (Figure 1) to aid appropriate prescription in all care settings.
Figure 1. A flow diagram to assist decision making when considering dental radiographs for caries assessment in paediatric patients.
Factors to take into account when considering EBWs
Caries diagnosis
It is important to note that despite bitewing radiographs being described as the gold standard for detection of proximal caries lesions,13 the requesting of radiographs is patient specific, and is also not a replacement for dental examination by a clinician.2 In paediatric patients, bitewing radiographs are beneficial to detect proximal caries in enamel and dentine, occlusal dentine caries, secondary caries, and assess the quality of a dental restoration.2 The use of EBWs, combined with clinical examination, provides practitioners with the information to identify approximal surface caries in primary and mixed dentitions.14 EBW views should be considered for caries diagnosis in cases when children are unable to tolerate the intra-oral alternative. Disadvantages in using panoramic views for caries detection include the distortion from movement/incorrect positioning and presence of ghost shadows.2
Effective dose
Dose considerations are important because children are more susceptible to the stochastic risks of radiation. The effective dose of a panoramic radiograph is 2.7–38 μSv and for an intra-oral bitewing between 0.3 and 21.6 μSv.6 The radiation dose from a panoramic radiograph can be reduced by appropriate collimation of the beam.15 Interestingly however, a recent study showed that the effective dose from EBWs is comparable to that of a panoramic radiograph. The same study showed that the dose from EBWs was 3–11 times higher than that of intra-oral bitewing examination.16
Patient specific factors
The age of the patient must be taken into account when considering this investigation as good cooperation is required for the longer exposure cycle required for EBWs and panoramic radiographs. Intra-oral bitewings and oblique lateral radiographs require only a short exposure time, so movement errors are less likely.
Paediatric patients with a sensitive gag reflex and/or an inability to cooperate with positioning of the intra-oral image receptor will find intra-oral bitewings difficult. Extra-oral radiographs, such as the EBW, eliminate the trigger factors initiating a gag reflex.
Some patients with disabilities may not be able to stay still for the whole EBW or panoramic exposure. In these cases, intra-oral bitewings or oblique lateral radiographs would be more appropriate.
The panoramic unit can be adjusted for patients in wheelchairs. However, if there is a high headrest on the wheelchair, panoramic radiographs and EBWs may not be possible.
Solid state detectors used for intra-oral radiographs are also bulky, making intra-oral radiography more difficult in children. In addition, anatomical variations including large mandibular tori may prohibit correct positioning of an intra-oral image receptor. An extra-oral view overcomes this barrier.
Timing interval between bitewing radiographs
An effort should continue to be made among the dental profession to request radiographs on a patient-specific, indication-orientated basis. However, it is recognized that caries is prevalent among young and adolescent populations, and bitewings remain an important tool used to detect and monitor caries progression at regular intervals. Expert recommendation suggests the following interval of bitewing prescription:6
High caries risk: 6 month;
Moderate caries risk: 1 year;
Low caries risk: 12-18 month (primary dentition) and 2 year (secondary dentition).
As a rule, it can be said the younger the patient and more extended/active the caries, the higher probability to progress, which may indicate shorter monitoring intervals on a patient-specific basis.2 There is no present literature specifying timing intervals for EBWs, but it seems sensible to adopt the same selection criteria used for standard intra-oral bitewings.
Orthodontic considerations
Clinical presentation of a patient in the mixed dentition with carious first permanent molars and/or molar incisor hypomineralization will often require orthodontic opinion. In these cases, EBWs are usually sufficient for treatment planning because they generally provide a clear radiographic view of the developing second permanent molars (Figure 2). If the examination of the child shows evidence of crowding in anterior or buccal segments and/or the maxillary canines are not palpable in a child of 9 years of age or over, or if an orthodontist wants to consider root anatomy, then a full panoramic radiograph is indicated as preference over an EBW. This prevents repeat radiographic views being taken, and provides a holistic care approach between orthodontic and paediatric specialties.
Figure 2. Right and left extra-oral bitewing radiographs, grade acceptable, showing clear radiographic view of the developing second permanent molars.
Case report
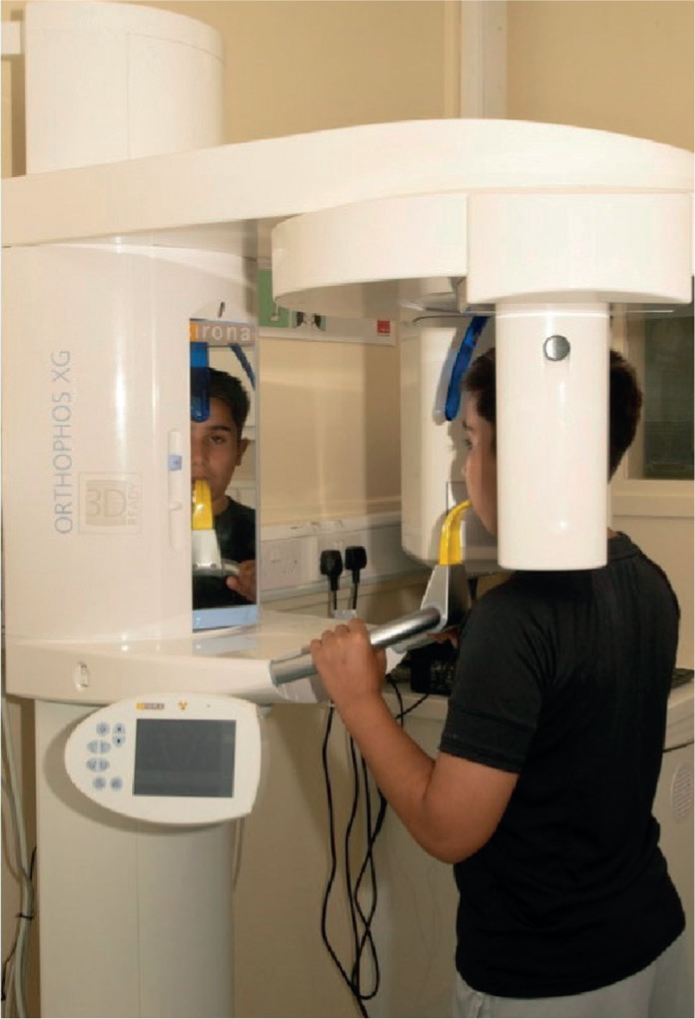
The following case illustrates the use of EBWs during treatment planning. A patient presented for a dental examination, accompanied by his mother. Symptoms of irreversible pulpitis were determined from his upper right first permanent molar (UR6). Despite excellent compliance, the patient's sensitive gag reflex meant that intra-oral bitewings were not possible, so EBWs were obtained to assess the extent of the caries. Figure 3 shows correct positioning of a patient for EBW radiographs. Acceptable right and left EBWs (Figure 4) showed extensive caries in the UR6 and early radiographic signs of occlusal caries in the LR6 and LL6. However, nothing abnormal was clinically detected in the LR6 and LL6, so a decision was made to keep both lower molars under review with appropriate preventive measures, in accordance with guidelines.17 The management plan, following consultation with an orthodontist, included immediate pulp extirpation and dressing of the UR6 for symptom relief, followed by treatment planning once the permanent dentition was fully established.
Figure 3. A paediatric patient with a sensitive gag reflex, correctly positioned to have extra-oral bitewings taken.Figure 4. Right and left extra-oral bitewing radiographs, taken for caries assessment in a paediatric patient who presented with irreversible pulpitis from UR6. Radiolucencies indicative of caries can be seen in UR6, URE, LR6, LL6 and LLE. In this case the developing upper second permanent molars are not fully visualized.
Conclusion
In specific cases, EBWs can play a vital role in dental caries assessment and are becoming increasingly accessible in general dental practice. EBWs can be useful when intra-oral bitewing views are not possible or appropriate due to compliance issues. However, patient factors need to be taken into account when considering this radiographic view.