Pitts NB, Chestnutt IG, Evans D, White D, Chadwick B, Steele JG The dentinal caries experience of children in the United Kingdom, 2003. Br Dent J. 2006; 200:313-320
London: Department of Health; 2005
King NM, Shaw L, Murray JJ Caries susceptibility of permanent first and second molars in children aged 5–15 years. Community Dent Oral Epidemiol. 1980; 8:151-158
Carvalho JC, Ekstrand KR, Thylstrup A Dental plaque and caries on occlusal surfaces of first permanent molars in relation to stage of eruption. J Dent Res. 1989; 68:773-779
Chestnutt IG, Schafer F, Jacobson AP, Stephen KW Incremental susceptibility of individual tooth surfaces to dental caries in Scottish adolescents. Community Dent Oral Epidemiol. 1996; 24:11-16
Edinburgh: SIGN; 2000
Ekstrand KR, Christiansen J, Christiansen ME Time and duration of eruption of first and second permanent molars: a longitudinal investigation. Community Dent Oral Epidemiol. 2003; 31:344-350
Quaglio JM, Sousa MB, Ardenghi TM, Mendes FM, Imparato JC, Pinheiro SL Association between clinical parameters and the presence of active caries lesions in first permanent molars. Braz Oral Res. 2006; 20:358-363
Zenkner JEA, Alves LS, Oliveira de RS, Bica RH, Wagner MB Influence of eruption stage and biofilm accumulation on occlusal caries in permanent molars: a generalized estimating equations logistic approach. Caries Res. 2013; 47:177-182
Carvalho JC, Ekstrand KR, Thylstrup A Results after 1 year of non-operative occlusal caries treatment of erupting permanent first molars. Community Dent Oral Epidemiol. 1991; 19:23-28
Carvalho JC, Thylstrup A, Ekstrand KR Results after 3 years of non-operative occlusal caries treatment of erupting permanent first molars. Community Dent Oral Epidemiol. 1992; 20:187-192
Nourallah AW, Splieth CH Efficacy of occlusal plaque removal in erupting molars: a comparison of an electric toothbrush and the cross-toothbrushing technique. Caries Res. 2004; 38:91-94
Ekstrand KR, Christiansen ME Outcomes of a non-operative caries treatment programme for children and adolescents. Caries Res. 2005; 39:455-467
Goncalves AF, de Oliveira Rocha R, Oliveira MD, Rodrigues CR Clinical effectiveness of toothbrushes and toothbrushing methods of plaque removal on partially erupted occlusal surfaces. Oral Health Prev Dent. 2007; 5:33-37
Ahovuo-Saloranta A, Forss H, Walsh T, Hiiri A, Nordblad A, Mäkelä M, Worthington HV Sealants for preventing dental decay in the permanent teeth. Cochrane Database Syst Rev. 2013; 3
Deery C Caries detection and diagnosis, sealants and management of the possibly carious fissure. Br Dent J. 2013; 214:551-557
Beauchamp J, Caufield PW, Crall JJ, Donly K, Feigal R, Gooch B, Ismail A, Kohn W, Siegal M, Simonsen R Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008; 139:257-268
Antonson SA, Antonson DE, Brener S, Crutchfield J, Larumbe J, Michaud C, Yazici AR, Hardigan PC, Alempour S, Evans D, Ocanto R Twenty-four month clinical evaluation of fissure sealants on partially erupted permanent first molars: glass ionomer versus resin-based sealant. J Am Dent Assoc. 2012; 143:115-122
Kuhnisch J, Mansmann U, Heinrich-Weltzien R, Hickel R Longevity of materials for pit and fissure sealing – results from a meta-analysis. Dent Mater. 2012; 28:298-303
Mickenautsch S, Mount G, Yengopal V Therapeutic effect of glass-ionomers: an overview of evidence. Aust Dent J. 2011; 56:10-15
ten Cate JM Contemporary perspective on the use of fluoride products in caries prevention. Br Dent J. 2013; 214:161-167
Marinho VC, Worthington HV, Walsh T, Clarkson JE Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013; 7
Department of Health and British Association for the Study of Community Dentistry.London: Department of Health; 2009
Alanen P, Holsti ML, Pienihakkinen K Sealants and xylitol chewing gum are equal in caries prevention. Acta Odontol Scand. 2000; 58:279-284
Cochrane NJ, Reynolds EC Calcium phosphopeptides – mechanisms of action and evidence for clinical efficacy. Adv Dent Res. 2012; 24:41-47
Forgie AH, Paterson M, Pine CM, Pitts NB, Nugent ZJ A randomised controlled trial of the caries-preventive efficacy of a chlorhexidine-containing varnish in high-caries-risk adolescents. Caries Res. 2000; 34:432-439
Hiiri A, Ahovuo-Saloranta A, Nordblad A, Makela M Pit and fissure sealants versus fluoride varnishes for preventing dental decay in children and adolescents. Cochrane Database Syst Rev. 2010; 3
de Oliveira DC, Cunha RF Comparison of the caries-preventive effect of a glass ionomer sealant and fluoride varnish on newly erupted first permanent molars of children with and without dental caries experience. Acta Odontol Scand. 2013; 71:972-977
Madahar A, Deery C Acceptability of fissure sealants from a child's perspective: a service evaluation. Int J Paediatr Dent. 2012; 22:(Suppl s2)2-3
Morgan AG, Bailey JR, Rodd HD, Deery C Acceptability of fluoride varnish from the child's perspective. Dental Health. 2012; 51:6-9
Chestnutt IG, Chadwick BL, Hutchings S, Playle R, Pickles T, Lisles C Protocol for “Seal or Varnish?” (SoV) trial: a randomised controlled trial to measure the relative cost and effectiveness of pit and fissure sealants and fluoride varnish in preventing dental decay. BMC Oral Health. 2012; 12
Academic Clinical Fellow in Paediatric Dentistry, Unit of Oral Health and Development, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield, S10 2TA, UK.
Senior House Officer in Paediatric Dentistry, Department of Paediatric Dentistry, Charles Clifford Dental Hospital, 76 Wellesley Road, Sheffield, S10 2SZ
This article aims to update the practitioner on the various techniques and interventions available to prevent or control caries during this high-risk period. The evidence to support provision of toothbrushing advice, placement of fissure sealants and fluoride varnish application is considered, along with more novel methods. An evidence-based protocol is suggested to help the practitioner determine when further intervention is required and what action to undertake.
Clinical Relevance: This article aims to reinforce the need for rigorous caries prevention in an erupting permanent molar and provides an update on the evidence behind a range of clinical techniques used for this purpose.
Article
The overall prevalence of caries in permanent teeth of children and young people in the UK has reduced considerably over the past 30 years.1 However, there is no room for complacency as there are still certain groups within the child population, notably those living in social and economic deprivation, who have a high caries experience.2 To put this into context, a staggering 1 in 7 children by 8-years-old, and 1 in 3 children by 12-years-old, have experienced decay in at least one permanent tooth.1 When considering caries risk at a tooth level, the most susceptible site has been identified as the occlusal surface of molars, with teeth most vulnerable to caries initiation during the period of eruption.3,4,5 Therefore, there is considerable scope for dental professionals to intervene to control caries development and the young patient entering a lifelong cycle of needing restorative treatment.6Figure 1 shows a first permanent molar which has become carious. This article explores the scientific rationale behind the treatment options available to dental professionals to protect an erupting tooth in a young patient at risk of caries.
Figure 1. Early caries affecting a first permanent molar.
Toothbrushing advice
The reason that erupting teeth are more vulnerable to developing caries is not complicated. Carvalho and colleagues suggested it is simply that plaque accumulates more readily on occlusal surfaces because the teeth are easily missed during toothbrushing, and they are not fully subjected to oral functional forces (Figure 2).4 This presence of undisturbed plaque is then associated with the occurrence of active, rapidly-progressing carious lesions.7,8 Once a tooth erupts, the progression rate of an occlusal lesion slows or even arrests, but it can take an average of 15 months for full eruption to be completed.7 Zenkner and co-workers have demonstrated, on a large sample of 1,779, that teeth with visible plaque present are 14.5 times more likely to have active caries than those without a visible biofilm.9 The carious lesion forms at the entrance to the fissure and is therefore accessible to biofilm removal by a toothbrush. A straightforward, quick and evidence-based intervention available to dental professionals to address this plaque accumulation seen on partially erupted teeth is to teach children and parents just to change the position of their toothbrush so it is held in a buccal-lingual direction instead of the conventional mesial-distal placement.10,11,12,13,14 It is helpful to disclose the plaque present to help the child and parent understand the issue and what is required in terms of biofilm removal. For young children under eight years, it is important that the parent or carer assists with toothbrushing, until the child has adequate understanding and manual dexterity. Figure 3 shows a child who has been taught to brush his/her erupting tooth with the modified technique from the side. Additionally, fluoride in toothpaste would then be able to reach the tooth surface directly.
Figure 2. Plaque accumulation on the surface of a first permanent molar.Figure 3. Demonstrating the buccal-lingual toothbrushing technique.
Fissure sealants
There is an overwhelmingly strong evidence base to support the use of sealants (Figure 4) as an intervention that works to reduce dental caries.15 To quantify the considerable benefits, it has been shown that sealed occlusal surfaces in permanent molar teeth of children aged 5 to 10-years-old have over a 50% reduction in decay compared to teeth without sealants over approximately 4 years. Importantly, sealant use is within the hands of dental professionals, and does not depend on a lifestyle change by the patient and his/her family for results. Sealant placement essentially creates a barrier which removes the biofilm from the occlusal surface.15 This can prevent the initiation of a new carious lesion, and arrest an established, non-cavitated lesion into enamel or dentine.16 Consequently, sealing pits and fissures of permanent molars has been recommended in a number of UK national clinical guidelines.17
Figure 4. A first permanent molar with a resin fissure sealant.
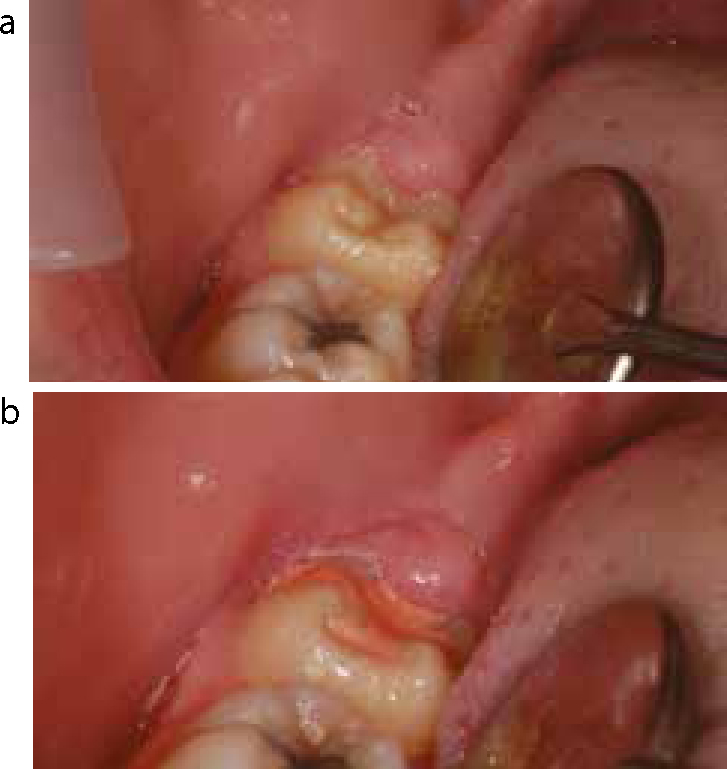
The most commonly used sealant materials available to dental practitioners are: resin-based and glass-ionomer cements.15 Resin sealants have been shown to have the best clinical effectiveness and should be considered the sealant-material-of-choice.15 However, a key requirement for effectiveness with all sealants is retention, and successful retention of resin sealants depends on the clinician being able to achieve adequate isolation during their placement. Regrettably, this can present a prohibitive clinical challenge in the case of a partially erupted tooth, where salivary contamination is a concern and maintaining a dry field becomes difficult. One strategy to enhance retention of resin sealants is the use of a bonding agent after acid-etching.18 However, this will increase the total treatment time, and could ultimately be counter-productive. Rather than waiting for full eruption to place a sealant, which might then be too late to prevent caries, glass-ionomer cements, which do not require acid-etching, could be used as a valuable interim option (Figures 5a and b).19 A meta-analysis of the retention rates of various sealant materials found that glass-ionomer cements had a 2-year retention figure of only 12%.20 However, this is not an issue in reality because the glass-ionomer sealant can be maintained at review appointments and replaced by a resin material when isolation is possible. Furthermore, this low retention rate may be pessimistic. Antonson and colleagues compared resin and glass-ionomer cement sealants on partially erupted teeth, and concluded that, at 24 months, the two types of sealants had similar retention rates.19 Additionally, the fluoride released from glass-ionomer cements may provide further protection, although the strength of evidence to support this is limited.21
Figure 5.
(a) An erupting molar prior to glass-ionomer cement sealant placement. (b) An erupting molar after glass-ionomer cement sealant placement.
Fluoride varnish
For dental professionals, fluoride is the key weapon in the war against caries.22 The most important mechanism through which fluoride acts is at the tooth/plaque interface, by inhibiting demineralization that would lead to caries initiation or progression, and promoting the remineralization of an initial lesion.22 Professionally applied fluoride varnishes contain a high concentration of fluoride (5% sodium fluoride) in a quick-setting form which tenaciously adheres to a tooth surface (Figure 6).23 The fluoride is then slowly released over a 12-hour period with prolonged effects.23 Interestingly, the released fluoride does not have to be present in high concentrations to continue to have an effect. Studies have demonstrated that, following a fluoride varnish application, globules of relatively insoluble calcium fluoride are formed on the tooth surface and in plaque, these then act as a slow-release fluoride reservoir whenever the oral pH falls.22 Like fissure sealants, there is a wealth of good evidence that fluoride varnishes are clinically effective, with a recently updated meta-analysis of 13 trials reporting a sizeable 43% reduction in caries in permanent teeth with its use.23 However, unlike fissure sealants, fluoride varnishes have the advantage of not being technique sensitive, although there is some evidence that drying the tooth first will optimize adhesion.17 The current recommendation is that high caries risk children and young people should have a fluoride varnish application at 3-monthly intervals.24 Given the previously discussed effectiveness of this simple and well accepted intervention, this population-centred approach appears correct.
Figure 6. Topical fluoride varnish applied to the tooth surface.
Novel interventions
Chewing gum
Chewing gum stimulates salivary flow and provides a degree of physical debridement of plaque on the occlusal surfaces. Gums containing xylitol may also provide an additional benefit by inhibiting Streptococcus mutans. One study has even shown regular use of gum containing xylitol to be as effective as sealing.25
Chewing gum has three main drawbacks:
Safety concerns regarding aspiration or swallowing the gum. For this reason manufacturers often recommend a minimum age of 6 years for use, hence the population of patients who can receive this treatment would be limited.
The environmental impact of spent chewing gum.
The level of compliance and regular use required to inhibit caries may not be practical for the majority of patients.
Case in Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP)
Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP) or casein phosphopeptide-amorphous calcium phosphate fluoride (CPP-ACPF) has been shown to aid enamel remineralization.26 When applied to a tooth surface, the casein degrades to release a phosphopeptide complex that readily binds to the enamel surface, delivering free calcium and phosphate ions to aid apatite reformation. CPP-ACP is most commonly used within sugar-free xylitol- or sorbitol-containing chewing gum, as well as dental creams and mouthrinses. There is not evidence to show an effect on occlusal lesions or any potential preventive effect from prophylactic application and, as such, it cannot yet be recommended for caries prevention for the erupting molar.
Chlorhexidine
There is no evidence to support the use of this antimicrobial to prevent occlusal caries, either as a varnish or mouthwash.27
Summary
So, at this point, for the majority of patients the practitioner is left with three options:
Toothbrushing;
Fissure sealants; or
Fluoride varnish?
The first part of the question is simple to answer; all children and parents/carers should be taught to brush erupting teeth with the modified from the side technique. Fissure sealants and fluoride varnishes both prevent caries development and inhibit caries progression at susceptible tooth sites, but should one treatment be used in preference to the other? Considering their clinical effectiveness, a systematic review found some evidence to support the superiority of fissure sealants, although only four trials were eligible for inclusion.28 In contrast, when de Oliveira and Cunha compared the effectiveness of glass-ionomer sealants and fluoride varnish on newly erupted first permanent molars in a split-mouth design, they found similar levels of success over 18 months.29 In terms of clinical use, fissure sealants are clearly the more demanding procedure, although child-centred service evaluations have identified surprisingly high levels of patient acceptability for both treatments.30,31 Morgan and colleagues did identify that nearly 20% of the participants expressed a strong dislike of the taste of fluoride varnish.31 Finally, to answer the fissure sealant or fluoride varnish question on a public health level, a large-scale randomized controlled trial has recently been conducted in primary schools in South Wales.32 This concluded that, for an individual high caries risk child in the dental surgery, both treatments should be fully utilized at all times. For the erupting tooth, the evidence is less clear yet, on the basis of current best evidence, the following appears to be an appropriate regime:
All children and parents/carers should be taught the modified side brushing technique;
All children should have fluoride varnish applied three to four times per year;
Teeth where the patient is failing to remove the plaque present adequately should have glass ionomer sealants placed;
Similarly, any occlusal surface demonstrating even the earliest stages of enamel caries should have a glass-ionomer sealant placed.
In conclusion, we understand why the occlusal surface of the erupting molar tooth is caries prone; similarly, we have effective interventions, which should be utilized.