Periodontal disease has a wide spectrum of presentation, any of which can have an effect on the patient's dental well-being and overall quality of life. This sporadic but sometimes rapidly progressing condition can easily be missed in a busy general practice setting. It is essential that the correct diagnosis is made and our duty of care to the patient fulfilled. If the condition, along with the treatment options and appropriate advice, is not explained to the patient, the individual may well feel that he/she has been let down by the professional person trusted over many years.
Clinical Relevance: This article discusses the screening and referral of periodontal patients, taking into account the medico-legal challenges that are currently faced by general dental practitioners (GDPs).
Article
As dental health professionals, we have a duty of care to our patients. A breach of this can result in a claim of negligence. Should the matter progress to a court appearance, it is likely that the patient would be given credence over a practitioner whose notes were unable to support any recall of the events in question.
Periodontal litigation is on the increase;1 undiagnosed and untreated periodontal disease in particular. People are living longer, and more people are retaining their teeth into later life. Consequently, the overall potential periodontal risk is rising. But what drives patient claims? Failure to diagnose is the most common reason. A patient may potentially be unaware of the presence or extent and severity of the disease. Periodontal disease left untreated may result in tooth loss, which would then be grounds to seek a claim of clinical negligence. Therefore, failure to explain the implications and possible sequelae of the condition may also initiate a claim. This may occur when the patient sees a new dentist for the first time. Sometimes the patient attends a different dentist in an emergency situation. On other occasions, of course, a patient will seek a second opinion because he/she already has concerns about the treatment being provided by an existing dentist. It is therefore clear that accurate periodontal diagnosis and the communication of key messages to the patient is absolutely imperative. Furthermore, failure to document essentially means a failure to diagnose; good contemporaneous clinical records are fundamental.
GDPs should always listen to their patients. Most of the time, patients will give clues that will contribute in making the diagnosis. Asking open-ended questions initially can help to start a more detailed conversation. The British Society of Periodontology (BSP) suggests asking the following seven questions:2
Do your gums bleed on brushing or overnight?
Are any of your teeth loose?
Can you chew everything you want to?
Do you have a bad taste or smell from your mouth?
Do you suffer from pain, swelling, gumboils or blisters?
Do you smoke?
Is there anything else you would like to tell me?
Periodontal probing
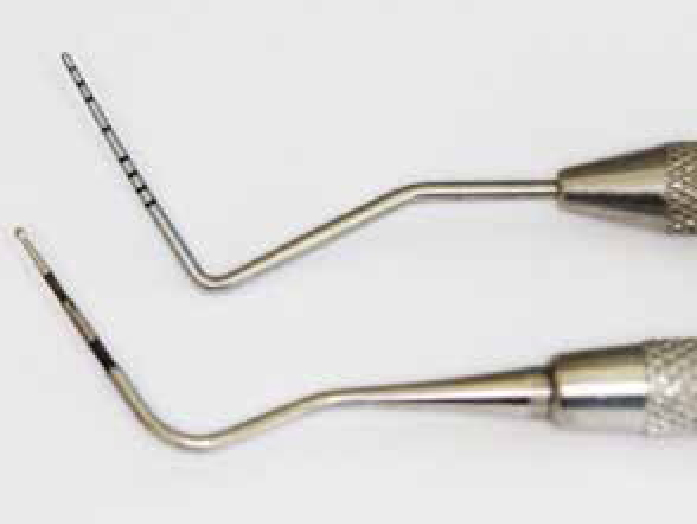
Periodontal probing is crucial for periodontal diagnosis and monitoring. Periodontal probing can indicate the pocket depth as well as the presence of bleeding, suggesting the presence of inflammation. A number of different probes are available (Figure 1). A Basic Periodontal Examination (BPE) probe is used for screening. The standard periodontal probe is necessary for more detailed data collection, examples include the 10 mm Williams probe and the 15 mm UNC probe. The BPE is used to screen patients for periodontal disease. This enables one to screen patients quickly and simply for periodontal disease. It is used to indicate the level of examination required and provides a basic guidance on treatment need. In October 2011,3 the BSP published updated guidelines on the BPE. The main changes were that the use of the asterisk symbol (▪) should now be used to denote only the presence of a furcation, and that both the number code and the ▪ should be recorded for each sextant where furcation involvement is found. It is also imperative to remember that full probing depths (six sites per tooth) are required for any sextants where code 3 is recorded; if a code 4 is present, full probing depths throughout the entire dentition is required. In order that the BPE should be used as a universal standardized tool for screening for periodontal disease, it is imperative that all dental practitioners follow the same guidelines.
Figure 1. BPE probe (below) and Williams Probe (above).
When recording the full findings, the BSP suggests that, as a minimum, plaque scores, probing pocket depths, recession, bleeding on periodontal probing and mobility need to be recorded. This will be used to monitor oral hygiene compliance, guide therapy to affected sites and monitor treatment. It will, moreover, resist a complaint that you did not diagnose and treat properly.
Periodontal radiographs
Appropriate radiographs are an important part of the clinical records. Appropriate radiographs should follow initial clinical examination and need to be selected according to the clinical presentation. As a general guide, the BSP suggest that radiographs will be needed for BPE codes 3, 4 or ▪.2 Radiographs are similarly helpful to monitor stability of the periodontal condition during recall or maintenance appointments. Clinical need should determine the frequency of repeat radiographs. Bone loss is slow to become apparent on radiographs and this factor needs to be balanced with the need for adequate monitoring of sites that may not be stable or if more complex restorative treatment is under consideration. Horizontal bitewings are routinely taken for assessing caries; these may also give an early warning of localized bone loss as well as the presence of subgingival calculus. Vertical bitewings provide greater information on the bone level for cases with moderate to severe bone loss, but these can only be positioned accurately in patients with quite tall palatal vaults. Paralleled perapicals are the ‘gold standard’ radiograph for periodontal cases. Periapicals allow visualization of the entire root anatomy; this can be very useful in assessing the bone level in relation to total root length for determining prognosis, assessing furcation involvements and identifying possible endodontic complications. A panoramic radiograph might be necessary if there are symptomatic third molars. However, the dosage from a single panoramic radiograph is greater than the dosage produced by a full mouth set of periapical radiographs and panoramic radiographs are not as accurate in showing bone defects and periapical pathology. When providing a radiographic report, it is important to include the degree of bone loss, type of bone loss and make a note of any other features such as perio-endo lesions.
Periodontal treatment
It is the responsibility of the dentist to screen patients for periodontal disease, to make a diagnosis and institute a treatment plan with defined therapeutic goals. Often, there may be cases that we feel uncomfortable in managing alone, either because of the extent or complexity of the problems. As part of patient management and with an aim to achieve predictable outcomes, one should then consider referring such patients to a specialist for help and support. It is important to bear in mind that in cases of severe periodontal disease, it is easier for patients to allege, after the event, that they would have preferred a referral for specialist care.
The BSP has created guidelines for referral4 which are summarized below:
Complexity 1 cases may be treated in general practice – BPE scores 1–3 in any sextant;
Complexity 2 cases can either be referred or treated by the general practitioner – BPE score of 4 in any sextant or surgery involving the periodontal tissues;
Complexity 3 cases should be mostly referred. It is worthy to note that apparently simple periodontal treatment may have to be delivered by specialists as part of a more complex integrated treatment strategy. Complexity 3 includes a BPE score of 4 in any sextant, as well as one or more of the following factors:
A concurrent medical/oral factor that is affecting the periodontal tissues, such as diabetes;
Complicating root morphologies and anatomical factors that adversely affect prognosis;
Diagnosis of aggressive periodontitis as assessed either by severity of disease for age (under 35 years) or based on rapid periodontal breakdown (>2 mm attachment loss in any one year);
Non-response to previous optimally carried out treatment;
Patients requiring surgical procedures involving tissue augmentation or regeneration, including surgical management of mucogingival problems;
Patients requiring surgery involving bone removal such as crown lengthening;
Patients requiring surgery associated with osseointegrated implants;
The presence of a relevant modifying factor increases the complexity by 1 increment, and is not cumulative.
Modifying factors that are relevant to periodontal treatment
Co-ordinated medical or dental multi-disciplinary care;
Medical history that significantly affects clinical management;
Regular tobacco smoking (10+ cigarettes a day);
Special needs for the acceptance or provision of dental treatment;
Concurrent mucogingival disease such as erosive lichen planus.
Medical history that significantly affects clinical management
Patients with a history of head or neck radiotherapy or intravenous bisphosphonate therapy;
Patients who are significantly immunocompromised or immunosuppressed;
Patients with a significant bleeding dyscrasia or disorder;
Patients with a potential drug interaction.
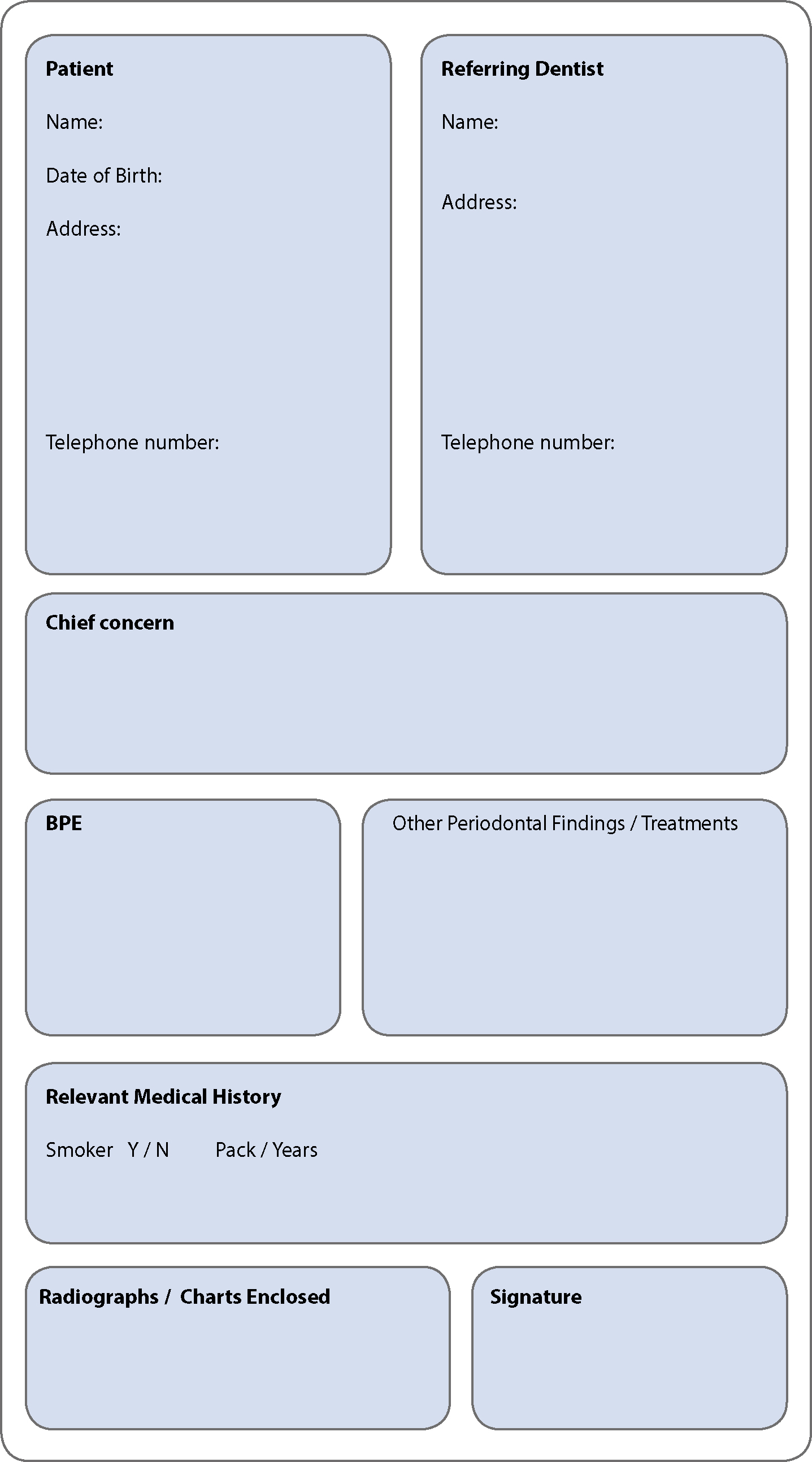
A referral letter should contain
The patient's personal details;
Reason for referral;
Any urgent problems;
Relevant medical history;
Smoking status;
Details of periodontal treatment completed; and
Relevant charts and radiographs.
Figure 2 shows an example referral proforma adapted from the BSP.2 Many NHS funded services have an enormous demand for services; the patient will have a greater chance of being accepted if as much relevant information as possible is provided. If the patient declines referral, details should be documented in the clinical notes and the option of referral should be discussed again at the next recall appointment.
Figure 2. Referral proforma.2
Conclusion
In summary, accurate diagnosis with appropriate care for a patient is critical in avoiding any initiation or progression of a litigious claim. Currently, there is a level of expectation that tooth loss is avoidable and there can be strong emotional implications to losing teeth. In many cases, the levels of periodontal disease present in a patient's mouth are due to factors beyond the dentist's control, and do not reflect any fault whatsoever on the part of the dentist. However, it is made much easier to demonstrate this fact when all the details have been recorded accurately.