Heasman PA, Ritchie M, Asuni A Gingival recession and root caries in the ageing population: a critical evaluation of treatments. J Clin Periodontol. 2017; 44:S178-S193 https://doi.org/10.1111/jcpe.12676
Romandini M, Soldini MC, Montero E, Sanz M. Epidemiology of mid-buccal gingival recessions in NHANES according to the 2018 World Workshop Classification System. J Clin Periodontol. 2020; 47:1180-1190 https://doi.org/10.1111/jcpe.13353
Beck JD, Koch GG, Offenbacher S. Attachment loss trends over 3 years in community-dwelling older adults. J Periodontol. 1994; 65:737-743 https://doi.org/10.1902/jop.1994.65.8.737
Pires IL, Cota LO, Oliveira AC Association between periodontal condition and use of tongue piercing: a case-control study. J Clin Periodontol. 2010; 37:712-718 https://doi.org/10.1111/j.1600-051X.2010.01584.x
Kapferer I, Benesch T, Gregoric N Lip piercing: prevalence of associated gingival recession and contributing factors. A cross-sectional study. J Periodontal Res. 2007; 42:177-183 https://doi.org/10.1111/j.1600-0765.2006.00931.x
Ainamo J, Löe H. Anatomical characteristics of gingiva. A clinical and microscopic study of the free and attached gingiva. J Periodontol. 1966; 37:5-13 https://doi.org/10.1902/jop.1966.37.1.5
Friedman N. Mucogingival surgery: the apically repositioned flap. J Periodontol. 1962; 33:328-340
Rosenberg NM. Vestibular alterations in periodontics. J Periodontol. 1960; 31:231-237
Corn H. Periosteal separation—its clinical significance. J Periodontol. 1962; 33:140-153
Bowers G. A study of the width of attached gingiva. J Periodontol. 1963; 54:201-209
Lang NP, Löe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol. 1972; 43:623-627
Abolfazli N, Saber FS, Lafzi A, Eskandari A. Evaluation of alteration in mucogingival line location following use of subepithelial connective tissue graft. Indian J Dent Res. 2010; 21:174-178 https://doi.org/10.4103/0970-9290.66628
Ainamo A, Bergenholtz A, Hugoson A, Ainamo J. Location of the mucogingival junction 18 years after apically repositioned flap surgery. J Clin Periodontol. 1992; 19:49-52 https://doi.org/10.1111/j.1600-051x.1992.tb01148.x
Miller PD A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985; 5:8-13
Cairo F, Nieri M, Cincinelli S The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study. J Clin Periodontol. 2011; 38:661-666 https://doi.org/10.1111/j.1600-051X.2011.01732.x
Agudio G, Nieri M, Rotundo R Periodontal conditions of sites treated with gingival-augmentation surgery compared to untreated contralateral homologous sites: a 10- to 27-year long-term study. J Periodontol. 2009; 80:1399-1405 https://doi.org/10.1902/jop.2009.090122
Mörmann W, Schaer F, Firestone AR. The relationship between success of free gingival grafts and transplant thickness. Revascularization and shrinkage – a one year clinical study. J Periodontol. 1981; 52:74-80 https://doi.org/10.1902/jop.1981.52.2.74
Kao RT, Curtis DA, Kim DM American Academy of Periodontology best evidence consensus statement on modifying periodontal phenotype in preparation for orthodontic and restorative treatment. J Periodontol. 2020; 91:289-298 https://doi.org/10.1002/JPER.19-0577
Chambrone L, Sukekava F, Araújo MG Root-coverage procedures for the treatment of localized recession-type defects: a Cochrane systematic review. J Periodontol. 2010; 81:452-478 https://doi.org/10.1902/jop.2010.090540
Zucchelli G, Mele M, Stefanini M Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: a comparative randomized-controlled clinical trial. J Clin Periodontol. 2010; 37:728-738 https://doi.org/10.1111/j.1600-051X.2010.01550.x
Han TJ, Takei HH, Carranza FA. The strip gingival autograft technique. Int J Periodontics Restorative Dent. 1993; 13:180-187
Cortellini P, Tonetti M, Prato GP. The partly epithelialized free gingival graft (pe-fgg) at lower incisors. A pilot study with implications for alignment of the mucogingival junction. J Clin Periodontol. 2012; 39:674-680 https://doi.org/10.1111/j.1600-051X.2012.01896.x
Gandara-Rey JM, Diniz-Freitas M, Gandara-Vila P Lesions of the oral mucosa in cocaine users who apply the drug topically. Med Oral. 2002; 7:103-107
Professor/Honorary Consultant in Periodontology; Centre for Host-Microbiome Interactions, Faculty of Dentistry, Oral and Craniofacial Sciences, King's College London
Recession defects are widely prevalent in the adult population, with some patients being impacted by complications, including the difficulty of cleaning such sites and the risk of continued recession progression. The free gingival graft (FGG) is a form of mucogingival surgery that attempts to improve the height of the keratinized tissue (KT), as well as augment the thickness of the gingival phenotype to facilitate meticulous oral hygiene. This article discusses the indications for the surgery, the procedure, including post-operative care, and possible modifications of the technique.
CPD/Clinical Relevance: Professional intervention involving a free gingival graft may be the only way to empower patients to clean the recession site without discomfort.
Article
Gingival recession can be defined as the exposure of the root surface due to apical migration of the gingival margin.1 Such defects can be localized or generalized, being present interproximally and/or labially/lingually. The latest NHANES data suggest that recession sites are widely prevalent, with 91.6% of the adult population presenting with the condition. Presence of gingival recession is associated with older age, female gender, European ethnicity and the mandibular arch.2
Aetiology
Recession can have a multifactorial aetiology and, therefore, a careful history and examination are required, as well as appropriate investigation of the affected sites (Table 1). The mechanism of recession is not fully understood, but the presence of persistent inflammation is required to lead to recession. Such inflammation can lead to the breakdown of the underlying connective tissue, which eventually leads to gingival tissue recession. Causes of inflammation can be mechanical, such as overzealous brushing3 or the use of overly hard bristles. Traumatic occlusion can also lead to recession in cases of a deep overbite in incisal Class 2 or 3 relationships where the incisal edges can directly contact the soft gingival tissues. Inflammation can also be attributed to a bacterial aetiology, where persistent plaque presence can lead to an inflammatory host response and, if left untreated, may develop into periodontitis.4 Tongue studs and lip piercings are also associated with recession. Individuals with tongue studs can have up to an 11-times greater chance of lingual recession of the mandibular incisors compared to non-users.5 Meanwhile, lip piercings that are positioned close to the cemento-enamel junction (CEJ) are associated with buccal/labial recessions.6 Both objects increase the risk of recession with long-term use.
Physical: lack of adequate cooling from ultrasonic irrigation
Bacterial: periodontitis
Autoimmune
Occlusal trauma
Deep overbite (Class 2 or 3)
Iatrogenic
Restorative treatment
Orthodontic treatment
Poorly fitting prosthesis
Risk factors
Thin periodontal phenotype
Prominent frenal attachment
Smoking
Malocclusion
Bony dehiscence
Age
Presence of keratinized tissue
Keratinized tissue (KT) is the part of the oral mucosa that covers the gingiva and hard palate, extending from the gingival margin to the mucogingival junction. It is composed of the free and attached gingiva. The gingival width varies throughout the oral cavity, with the buccal gingiva generally widest at the incisors and narrowest in the premolar region,7 while for the lower lingual aspect, it is narrowest at the lower incisors and widest at the molar region. It was previously thought that an adequate amount of KT around a tooth was important to maintain gingival health and prevent recession. The argument was that a narrow zone of KT would be less resistant to frictional forces during mastication, and a moveable gingival margin can result in inadequate pocket closure with eventual formation of subgingival plaque.8 Furthermore, the presence of a shallow vestibule would favour food-particle accumulation and impede a patient's oral hygiene.9 There were various opinions on the necessary amount of KT needed for the prevention of recession, ranging from more than 3 mm,10 to <1 mm11 with the most popular opinion being at least 2 mm.12
More recent studies have suggested that this may not be true. In 1980, Dorfman and colleagues reported results of a split-mouth study of 92 patients with bilateral sites with inadequate KT.13 One side had a free gingival graft (FGG) placed, while the contralateral side was treated as the control and monitored. After 2 years of close follow-up, no difference in the presence of recession between the experimental and control side was reported. Hence, it was concluded that gingival health can be maintained regardless of the dimensions of the gingival unit, and it is not linked to KT. The patients in the study were followed for up to 6 years and the initial findings were confirmed.14 In summary, it is not essential for KT to be present to maintain gingival health, but it is easier to maintain plaque control around teeth and implant sites with adequate KT because patients may experience discomfort when only lining mucosa is present.
Complications of recession
Patients can complain of, or have several, complications as a result of the presence of a recession defect. Some patients are concerned that the recession defect will continue to progress and accelerate, although evidence shows that this is unlikely to lead to tooth loss.15 Patients can also be concerned with poor aesthetics with interdental recession leading to the formation of black triangles, and labial recession leading to root exposure. The increase in crown height may affect a patient's appearance, particularly for those with a high smile line. Furthermore, sensitivity to hot and cold temperatures can develop as a result of exposure of the cementum and dentine. There can also be discomfort and difficulty brushing such areas because the more apical gingival margin can be difficult to access with the loss of KT. Overzealous brushing of the root can then lead to non-carious cervical lesions (NCCL) because the cementum/dentine surface is less resistant compared to the enamel surface of the crown.
Management of recession defects
Management of recession includes the following steps:
Aetiological assessment of the defect, without which, recession is likely to continue and develop.
Identification of patient concerns and expectations to ensure that the patient's expectations are realistic and can be met.
Removal of the aetiological factors can lead to stabilization of the defect without the need for invasive management.
Adjustment of brushing, which can include the correct bristle stiffness and an atraumatic technique, can reduce marginal inflammation, whereby no graft is required.
Management of complications, such as the removal of caries before any mucogingival surgical intervention is a prerequisite to ensure the surgery is successful. In cases of NCCL, it is easier to build up the missing root surface with composite prior to surgery rather than intra-operatively, where moisture control may be difficult.
When indicated, gingival recession can be corrected with mucogingival surgical procedures. There are a variety of techniques available and each has specific uses (Table 2).
Grafting procedure
Example
Pedicle grafts: blood supply is maintained from donor site after placement at the recipient site
Rotational flap procedures
Coronally advanced flap procedures
Regenerative procedures: use of EMD and membrane
Free grafts: the graft is completely derived from the donor site
Allogenic grafts: acellular dermal matrix or mucograft
Combination of the above
For example, coronally advanced flap with connective tissue graft
The free gingival graft
Introduced by Bjorn in 196316 and refined by Sullivan and Atkins in 1968,17 the free gingival graft technique was indicated for covering recession defects. Its success in covering recession varies from 11% to 100%.18 The main advantages of such a technique were to increase the vestibular depth and KT, as well as to increase the gingival thickness. This ameliorates the ability of the patient to access and clean the gingival margin comfortably. This technique has several disadvantages. There is a poor aesthetic appearance owing to the mismatch in the colour of the graft, which is usually more pale and pink compared to the adjacent tissues, and the misalignment of the mucogingival junction (MGJ) following surgery; however, over time the tissues align,19 as it is thought that the MGJ position is genetically predetermined.20Table 3 gives a summary of indications and contraindications.
Indications
Contraindications
No keratinized tissue present
Unpredictable root coverage
Shallow vestibule
Aesthetics compromised
Sensitivity to brushing
Patient tolerance for a donor site
Pre-operative preparation
Following a full history and examination, as well as a discussion of patient expectations, several factors should be covered concerning the clinical recession of the associated teeth (Table 4). Originally, recession defects were classified using the Miller index.21 However, there are several shortcomings. These include the lack of information on soft-tissue thickness and hard-tissue characteristics, such as NCCL and the presence of a CEJ. Therefore, the authors recommend the use of the recession matrix, which incorporates the data needed, as well as the Cairo classification22 for recession defects.
Recession type
Gingival site
Tooth site
Recession depth
Gingival thickness
Keratinized tissue width
Cemento-enamel junction (A/B)
Step defect (+/-)
No recession
Type 1
Type 2
LR1: 3mmLL1: 6mm
LR1: ThinLL1: Thin
LR1: 1mmLL1: 0mm
LR1: ALL1: A
LR1: -veLL1: -ve
Type 3
The recession classification states that:
Recession type 1 (RT1): buccal tissue recession with no loss of interproximal attachment;
Recession type 2 (RT2): buccal tissue recession with loss of interproximal attachment less than or equal to the buccal attachment loss;
Recession type 3 (RT3): buccal tissue recession associated with loss of interproximal attachment greater than the buccal attachment loss.
Before placement of a free gingival graft, the patient should have a course of non-surgical therapy. This involves educating the patient on the correct atraumatic brushing technique where indicated, as well as the removal of any plaque-retentive factors that could cause chronic inflammation. This can lead to resolution in some patients, without the need for further surgery. Additionally, good oral hygiene is a prerequisite to ensure that the patient will be compliant and maintain the gingival site following grafting, thus reducing the risk of failure of the free gingival graft. A widely used threshold of a 20% plaque score is the minimum recommended before continuing to surgery (Figure 1).
Figure 1.
(a,b) Pre-operative photo of lower central incisors showing presence of calculus and marginal inflammation. There is a lack of KT present with a thin gingival phenotype, no step defect and the CEJ is present. Furthermore, the shallow vestibule present in such a scenario makes it even more difficult for the patient to clean.
If the marginal inflammation persists, or the patient continues to experience difficulty cleaning areas owing to brushing sensitivity, and provided all the alternative treatment options have been discussed, the patient can be considered for a free gingival graft. The authors recommend that such mucogingival surgery would require training before implementing in practice.
Moreover, before surgery, it is worth considering the construction of an upper palatal healing plate, which can be made following an upper arch impression of the palate and associated teeth (Figure 2). The plate acts to apply pressure to the donor site following grafting to provide blood clot stability, as well as to protect the wound area during the early stages of healing from changes in temperature and food debris. Lastly, splinting of the affected teeth is important particularly when grade 2 mobility is present to ensure the graft is stable during healing. Early movement of the graft can lead to failure and necrosis.
Figure 2. A healing plate is made with palatal coverage and placement of Adams cribs on the first molars for retention. Note that the healing plate extends to the second molars so that none of the donor site is exposed following grafting.
Free gingival graft technique
At the beginning of the procedure, the root surface should be thoroughly debrided to remove any plaque. This can be done intra-operatively once a recipient bed is made, but there is a risk of removing connective tissue fibres and healthy cementum, which can be useful in achieving creeping attachment in the long term.23 Hence, the operator should measure the clinical attachment loss present at the recession site prior to the recipient bed preparation and use the measurement to guide the level at which the professional mechanical plaque removal is provided.
A 3-mm wide lateral and apical incision to the recession defect is prepared with a scalpel blade using a split-thickness approach whereby connective tissue and periosteum remains without exposure to the underlying bone (Figure 3). This ensures that the epithelium is removed to allow acceptance of a graft from a recipient site and also provides a bed of blood supply for the graft to integrate. The horizontal level of the incision should be at the level of the mucogingival junction and in case of no KT remaining, the incision should be made around the level of the gingival margin. Any presence of frenal involvement that would impact the stability of the graft should be removed and underlying fibres scaled to ensure no frenal relapse.
Figure 3. The recipient bed extended 3 mm mesial and distal from the LR1 recession defect. Apical extension was around 3–4 mm from the recession defect. The periosteum and part of the connective tissue was left.
Following bed preparation, a template is used to approximate the width and length of the FGG needed from the donor site. The template can be made of foil or the paper card of a sterile suture (Figure 4). The template should be adapted with suture scissors in a way that fits the recipient bed. A graft that is too small will mainly overlie the avascular surface of the root surface and risk necrosis, while one that is too large will lead to comorbidities for the patient and possible failure of integration of the graft if the donor tissue extends beyond the connective tissue bed.
Figure 4. Template adapted to the recipient bed. The measured template size on the recipient bed was approximately 15 x 7 mm.
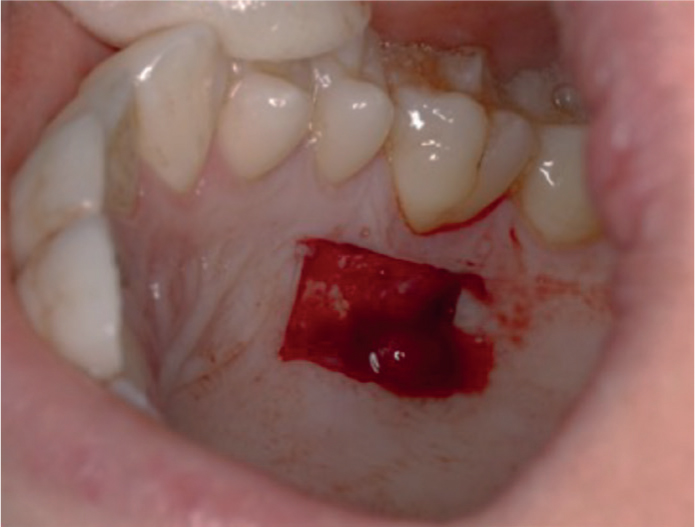
The template is transferred to the palate where the donor site is chosen and shallow incisions are demarcated to outline the graft. Ideally, the graft should be taken at least 2 mm away from the gingival margin of the maxillary teeth. Furthermore, the clinician should be aware of the position of the greater palatal foramen, which contains the greater palatine artery and nerve, as well as the path of these vessels in the palate, as iatrogenic damage to such sites can lead to severe bleeding and/or nerve damage. Lastly, the quality of the tissue should be considered and, therefore, rugae should be avoided when possible. Hence, the graft is normally taken using a new scalpel blade from the mesial line angle of the upper first premolar to the distal line angle of the first or second molar (Figure 5).
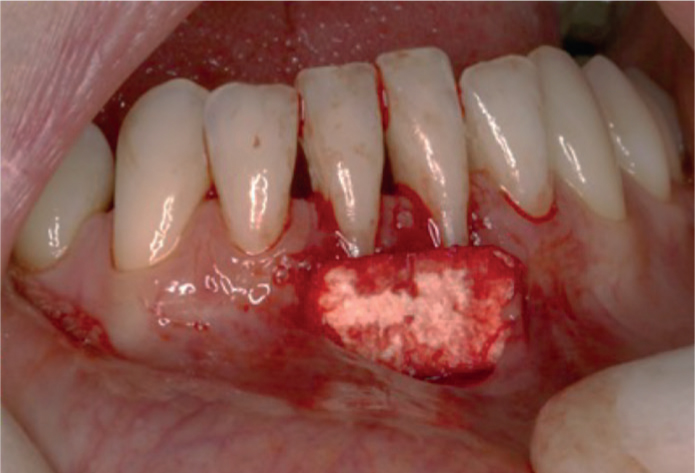
Figure 5. Free gingival graft extracted from palatal donor site.
The graft thickness should be approximately 1–1.5 mm. A graft that is too thick can lead to delayed healing and poor circulation, while a graft that is too thin means there is little connective tissue present and necrosis can lead to graft failure.24
The assistant should use compressed gauze at the donor site to temporarily achieve haemostasis while the clinician ensures that the graft has any fatty tissue remnants removed, followed by careful placement at the recipient site.
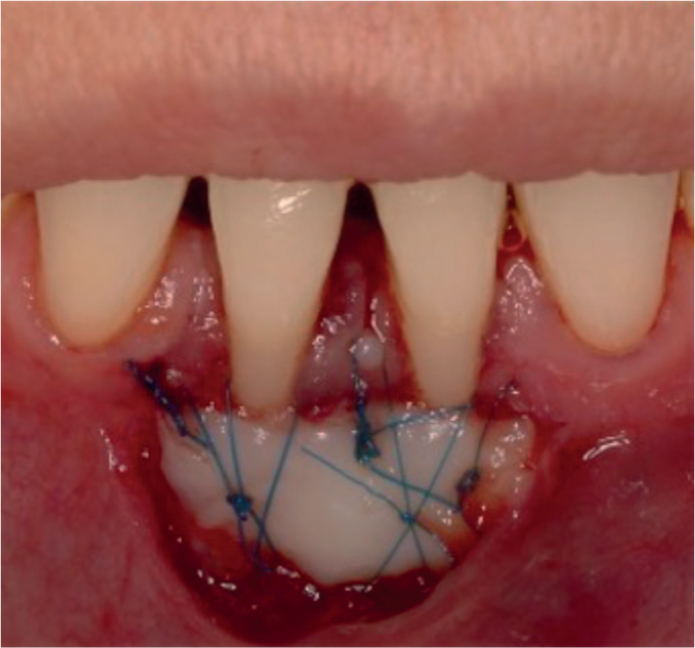
The graft is immobilized with simple interrupted sutures laterally followed by insertion of cross-sling sutures to compress the graft to the recipient site. Space between the graft and bed can lead to the formation of a blood clot that can inhibit the early stages of plasma circulation crucial for integration of the graft (Figure 6). Therefore, following successful suturing, a damp gauze is used to place firm pressure on the graft for 5 minutes.
Figure 6. The graft in place, two cross-sling sutures, as well as interrupted sutures to hold the graft in place. The lip was pulled to check for any mobility of the graft.
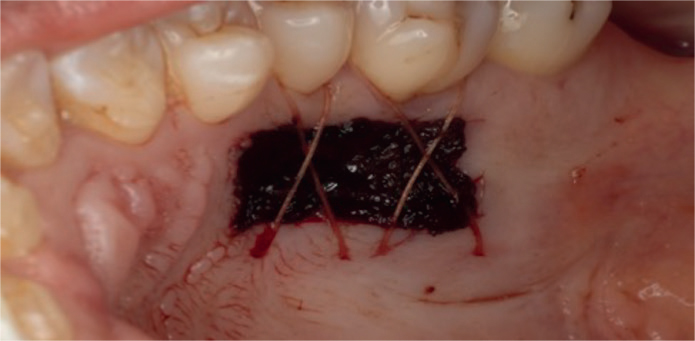
At this point, the donor site should be fully assessed for haemostasis (Figure 7). An absorbable haemostat and cross-sling sutures can be used to further promote haemostasis, as well as advising the patient to wear the healing plate for added support.
Figure 7. Donor site haemostasis achieved with an absorbable haemostat and cross sling sutures.
Post-operative care
The patient should avoid pulling the lip during the 2 weeks after surgery. This is to prevent mobility of the graft and loosening of the sutures. The sutures ideally should be removed 2 weeks after the surgery (Figures 8 and 9).
Figure 8. Two weeks post-operatively, prior to suture removal.Figure 9. Two weeks post-operatively, the donor site has almost healed fully.
For a few post-operative days, a soft diet and avoidance of spicy or salty food, which can exacerbate discomfort, is advised. The patient should avoid brushing the recipient site. Instead, they are recommended to rinse gently with chlorhexidine mouthwash twice daily until suture removal. Analgesics, especially for the first few days, can alleviate any pain. The patient should be given a contact for emergencies or when post-operative bleeding does not stop with local measures. Gentle brushing can resume around 2 weeks post-surgery, with interdental brushing at 3 weeks.
Clinical outcomes
If the graft successfully integrates at the recipient site, the patient should note a reduction in discomfort while brushing the gingival margin of the associated teeth. The patient would also have easier access to the gingival margin of the graft-associated teeth due to the increase in vestibular height and removal of any frenal involvement. In some cases, the graft may lead to creeping attachment, which can occur up to 12 months post-treatment (Figure 10). It is thought that the reason for this is due to coronal migration of the long junctional epithelium.23 The gingival phenotype in the grafted area could also change from thin to thick, which is associated with less gingival recessions (Figure 11).25
Figure 10. Creeping attachment at 9 months post surgery. The gingiva is healthier than pre-operatively with less bleeding on probing.Figure 11. Increased thickness of the gingival phenotype due to the free gingival graft.
In terms of root coverage, the available literature suggests that the results can be unpredictable, with the mean percentage root coverage ranging from 11% to 87%, with the greatest success in narrow and shallow recession defects.18 The results are generally inferior when compared to a coronally advanced flap alone, or when combined with a graft.26 Of 228 patients who underwent mucogingival procedures analysed by Griffin and colleagues,27 it was found that patients with FGG procedures were three times more likely to develop post-operative pain and bleeding compared to connective tissue graft (CTG) procedures. This is attributed to the donor site healing whereby FGG surgeries inevitably lead to secondary intention healing. Interestingly, Zucchelli28 suggested that there is no difference in post-operative pain for either FGGs or CTGs, and that the discomfort for patients corresponds to the remaining palatal tissue thickness of the donor site.
Modifications of the technique
Several modifications to the original technique have been made to attempt to improve on the technique's shortcomings. Bernimoulin and colleagues29 were the first to describe a two-stage technique in which a coronally advanced flap of the graft site was achieved 2 months post FGG placement. The technique attempted to improve on root coverage as the authors reported that part of the FGG covering the denuded root surface failed to survive. Another modification described by Rateitschak in 1985, described as the accordion technique, aimed to cover a wide recipient bed.30 The graft taken from the donor site is expanded in width with alternating incisions to allow it to cover a greater distance by changing the configuration of the graft. However, the new shape of the graft leads to areas with no coverage from the graft. A similar technique by Han and colleagues31 described obtaining minimum 2-mm wide strips of donor tissue, which are then sutured to the recipient site. The aim was to reduce the number of surgical procedures of gingival augmentation in cases of generalized lack of keratinized tissue.
Lastly, the partly epithelialized free gingival graft technique described by Cortellini and co-authors32 focused on bypassing the poor aesthetics of the free gingival graft, as well as the difficulty of coronally advancing the flap for a second stage owing to the relatively shallow vestibule in commonly indicated recipient sites for the lower incisors. The technique involves de-epithelializing the apical part of the graft, which is placed between the dissected alveolar mucosa and the periosteum of the recipient bed and extended 2–3 mm apical to the bone dehiscence. The epithelialized part is measured so that it extends from the CEJ to the position of the MGJ. Patient-reported outcomes from the case series are comparable to other well-founded mucogingival techniques.
Conclusion
The free gingival graft technique is a predictable procedure indicated for the patient who persistently finds it uncomfortable to effectively clean sites that lack KT on teeth and implants. General dental practitioners should be aware of such mucogingival procedures and it is a relatively simple technique for clinicians who are willing to undergo further training in mucogingival surgery.
Even with the introduction of techniques, such as tunnelling/rotational flap associated with CTG, the FGG is by no means an obsolete technique. The original technique and its variations could still be successfully used for recession cases, especially in those with a lack of keratinized gingiva, a prominent and thick associated frenal attachment and/or reduced vestibulum width.