De Cleen M. Obliteration of pulp canal space after concussion and subluxation: endodontic considerations. Quintessence Int. 2002; 33:661-669
Andreasen JO, Andreasen FM.Copenhagen: Munksgaard; 2007
Feiglin B. Dental pulp response to traumatic injuries – a retrospective analysis with case reports. Endod Dent Traumatol. 1996; 12:1-8
Neville BW, Damm DD, Allen CM, Bouquot JE.Philadelphia, USA: WB Saunders Co; 1995
Ngeow WC, Thong YL. Gaining access through a calcified pulp chamber: a clinical challenge. Int Endod J. 1998; 31:367-371
Gopikrishna V, Parameswaran A, Kandaswamy D. Criteria for management of calcific metamorphosis: review with a case report. Ind J Dent Res. 2004; 15:54-57
Abbott PV, Yu C. A clinical classification of the status of pulp and the root canal system. Aust Dent J. 2007; 52:S17-S30
Amir FA, Gutmann JL, Witherspoon DE. Calcific metamorphosis: a challenge in endodontic diagnosis and treatment. Quintessence Int. 2002; 1:61-69
Chicago: AAE; 2003
Andreasen JO. Luxation of permanent teeth due to trauma: a clinical and radiographic follow-up study of 189 injured teeth. Scand J Dent Res. 1970; 78:273-286
Holcomb JB, Gregory WB. Calcific metamorphosis of the pulp: its incidence and treatment. Oral Surg Oral Med Oral Path. 1967; 24:825-830
Oginni AO, Adekoya-Sofowora CA. Pulpal sequelae after trauma to anterior teeth among adult Nigerian dental patients. BMC Oral Health. 2007; 7
Selden HS. Radiographic pulpal calcifications: normal or abnormal – a paradox. J Endod. 1991; 17:34-38
Andreasen FM, Yu Z, Thomsen BL, Andersen PK. Occurrence of pulp canal obliteration after luxation injuries in the permanent dentition. Endod Dent Traumatol. 1987; 3:103-115
Lundberg M, Cvek M. A light microscopy study of pulps from traumatized permanent incisors with reduced pulpal lumen. Acta Odontol Scand. 1980; 38:99-94
Robertson A. A retrospective evaluation of patients with uncomplicated crown fractures and luxation injuries. Endod Dent Traumatol. 1998; 14::245-256
Heithersay GS. Calcium hydroxide in the treatment of pulpless teeth with associated pathology. J Br Endod Soc. 1975; 8:74-93
Andresen FM. Pulpal healing after luxation injuries and root fracture in the permanent dentition. Endod Dent Traumatol. 1989; 5:111-131
Ten Cate AR.St Louis: Mosby; 1998
Avery J. Repair potential of the pulp. J Endod. 1981; 7:205-212
Torneck C. The clinical significance and management of calcific pulp obliteration. Alpha Omega. 1990; 83:50-54
Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontal bone assessment, and endodontic applications. Dent Clin North Am. 2008; 52:825-841
Patel S. New dimensions in endodontic imaging: Part 2. Cone beam computed tomography. Int Endod J. 2009; 42:463-475
Mazzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone–beam technique: preliminary results. Euro Radio. 1998; 8:1558-1564
Ludlow JB, Davies-Ludlow LE, Brooks SL., Howerton WB. Dosimetry of 3 CBcr devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac Radiol. 2006; 35:219-226
Ludlow JB, Lester WS, See M, Bailey LJ, Hershey HG. Accuracy of measurements of mandibular anatomy in cone beam computed tomography images. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2007; 103:534-542
Cotton TP, Geisler TM, Holden OT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007; 9:1121-1132
Macleod I, Heath N. Cone-beam Computed Tomography (CBCT) in dental practice. Dent Update. 2008; 35:590-598
Farman AG, Farman TT. A comparison of 18 different X-ray detectors currently used in dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2005; 99:485-489
Mora MA, Mol A, Tyndall DA, Rivera E. In vitro assessment of local tomography for the detection of longitudinal tooth fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2007; 103:825-829
Holan G. Tube-like mineralization in the dental pulp of traumatized primary incisors. Endo Dent Traumatol. 1998; 14:279-284
Nair M, Nair U. Digital and advanced imaging in endodontics: a review. J Endod. 2007; 33:1-6
Levin LG, Law AS, Holland GR, Abbott PV, Roda RS. Identify and define all diagnostic terms for pulpal health and disease states. J Endod. 2009; 35:1645-1657
Oginni AO, Adekoya-Sofowora CA, Kolawole KA. Evaluation of radiographs, clinical signs and symptoms associated with pulp canal obliteration: an aid to treatment decision. Dent Traumatol. 2009; 25:620-625
Jacobsen I, Kerekes K. Long-term prognosis of traumatized permanent anterior teeth showing calcifying processes in the pulp cavity. Scand J Dent Res. 1977; 85:588-598
Bauss O, Röhling J, Rahman A, Kiliaridis S. The effect of pulp obliteration on pulpal vitality of orthodontically intruded traumatized teeth. J Endod. 2008; 34:417-420
Patterson SS, Mitchell DF. Calcific metamorphosis of the dental pulp. Oral Surg Oral Med Oral Pathol. 1965; 20:94-101
Schindler WG, Gullickson DC. Rationale for the management of calcific metamorphosis secondary to traumatic injuries. J Endod. 1988; 14:408-412
Shuler SE, Howell BT, Green DB. Unusual pattern of pulp canal obliteration following luxation injury. J Endod. 1994; 20:460-462
Cvek M, Granath L, Lundberg M. Failures and healing in endodontically treated non-vital anterior teeth with post-traumatically reduced pulpal lumen. Acta Odontol. 1982; 40:223-228
Akerblom A, Hasselgren G. The prognosis for endodontic treatment of obliterated root canals. J Endod. 1988; 14:565-567
Patel S, Rhodes J. A practical guide to endodontic access cavity preparation in molar teeth. Br Dent J. 2007; 203:133-140
Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonics in endodontics: a review of literature. J Endod. 2007; 33:81-95
Khabbaz MG, Serefoglou MH. The application of the buccal object rule for the determination of calcified root canals. Int Endo J. 1996; 29:284-287
Weine FS. Periapical surgery; intraoral imaging and its use with surgery and other procedures. In: Weine FS (Ed). St Louis, USA: Mosby-Year Book Inc; 2004
Calcific metamorphosis (CM) is a commonly observed phenomenon following traumatic injuries like concussion, subluxation and luxation. Depending on the severity of the injury and the developmental stage of the tooth, there can be either complete or partial obliteration of root canals. However, histologically, there is always persistence of fine residual filaments of pulp tissue or tracts of organic material without the presence of any inflammatory component. A periodic clinical and radiographic follow-up examination is preferred and usually, for cosmetic reasons, only a conservative aesthetic treatment is required. Endodontic treatment is only advocated if there is development of apical periodontitis and, if executed properly, can be highly successful.
Clinical Relevance: Appropriate management of calcific metamorphosis can present a clinical dilemma to the clinician. Thus a judicious and prudent decision should be made between endodontic intervention for the involved tooth and other available restorative (and/or aesthetic) treatment options.
Article
Traumatic injuries to the teeth affect both the hard tissues (enamel, dentine and cementum) and the soft tissues surrounding the teeth (periodontal tissues). Following trauma, commonly encountered moderate injuries affecting the periodontium include concussion and subluxation and attenuated injuries include luxation:1,2
Concussion is an injury to the supporting apparatus of the tooth that does not cause increased (non-physiologic) loosening or displacement of the tooth but that does result in clear sensitivity to percussion.
Subluxation is an injury to the supporting apparatus of the tooth that results in increased mobility but does not cause displacement of the tooth.
Luxation is an injury that causes displacement of the tooth in the coronal, apical or lateral direction. Moderate injuries, in a majority of cases, are associated with minor symptoms and, therefore, go unnoticed both by the patient and/or by the clinician.1
Pulpal reactions to traumatic injuries can vary from immediate pulpal death to long-term slow pulp canal mineralization.3 The prognosis of pulpal healing and survival, following trauma, depends on the degree and type of trauma, age of the patient and the condition of the tooth in the post-traumatic period.3 The pulpal reactions to traumatic injuries, based on the prognosis of pulpal healing, are classified into three main categories:3
Category 1. Pulp with very poor prognosis for healing: In these cases, the traumatic incident results in pulpal necrosis in a matter of days to a month and thus requires endodontic therapy soon thereafter. It is usually seen in cases of an extensive crown fracture together with subluxation, an extrusive luxation, an intrusive luxation or a lateral luxation.3
Category 2. Pulp with a moderate prognosis for healing: In these cases, the tooth shows rapid pulpal mineralization within a period of 18–24 months. Subluxation injury, concussion injury and lateral luxation injury are the main types of traumatic injuries in this category.3 In some cases, the pulp canal remains open and unchanged coronally, ie the pulp appears necrotic, whereas apically the pulp canal is nearly closed, suggesting the presence of vital pulp.
Category 3. Pulp with a very good prognosis for healing: These teeth show slow pulp canal mineralization, and rarely require endodontic therapy.3 They usually contain vital pulp tissue and undergo very slow mineralization of the pulp canal, over a period of five years or more.
As discussed (in categories 2 and 3), the obliteration of the pulp chamber and canal following traumatic injury to the affected tooth is termed as Calcific Metamorphosis (CM) or Pulp Canal Obliteration (PCO) or Pulp Canal Calcification (PCC).4–7Calcific metamorphosis is a pulpal response to trauma characterized by rapid deposition of hard tissue within the root canal space.8,9 There can be either partial or complete pulp canal obliteration. The frequency of this obliteration depends on the extent and severity of the luxation and the stage of the root development at the time of injury.1,2,10,11 Calcific metamorphosis has been found to develop more in teeth with concussion and subluxation injuries, whereas pulpal necrosis occurred more often in traumatized teeth with fractures.10,12 The incidence of obliteration following concussion is 3% in teeth with incomplete roots and 7% in teeth with completely formed roots. Following subluxation, it is 11% in teeth with incomplete root formation and 8% in teeth with completed root formation.1 Pulpal necrosis occurs in 3% of concussion and 6% of subluxation cases. In luxation injuries, CM is more prevalent in teeth with incomplete root formation.1,8,10
Successful management of these cases may be a clinical challenge. Depending on the clinical appearance of the tooth, current pulpal status and present periapical condition, an array of different treatment modalities (aesthetic, restorative, endodontic and prosthodontic treatment) may be required for a complete and successful, aesthetic and functional restoration of such teeth. Thus, the clinical management of CM can range from a simple conservative restorative procedure (veneering) to a more complex endodontic treatment of the calcified pulp chamber (access opening and location of canal orifice) and narrow root canals (cleaning, shaping and obturation of canals).
The following review describes the clinical, radiographic and histological characteristics of CM and applied clinical aspects in the management of such cases.
Pathogenesis
The literature is clear that calcific changes may be a response to a wide range of stimulants: operative procedures, restorative materials, caries, tooth abrasion, periodontal disease, pulp inflammation, pulp capping, trauma and ageing. Some may be idiopathic.13 CM usually occurs following trauma from a fall while playing sports or suffering assaults.1,2 A significant relationship has also been observed between the type of splint (fixation) and this complication of healing. Use of fixed splints like orthodontic bands/acrylic fixation can cause additional trauma to the already traumatized periodontal ligament due to forceful placement of the bands.2 Up to 24% of traumatized teeth develop varying degrees of calcific metamorphosis.6,8,10–11,12,14 It is characterized by the deposition of an osteoid-like tissue that is either produced by the odontoblasts at the periphery of the pulp space or by undifferentiated pulpal cells that undergo differentiation as a result of the traumatic injury.8,15 This results in simultaneous deposition of a dentine-like tissue along the periphery of the pulp space (root canal walls) and within the pulp space proper (root canal). The accelerated rate of hard tissue formation can lead to the entrapment of some pulpal cells, giving the histologic appearance of osteodentine with an irregular tubular pattern. The cells constituting this hard tissue can be either undifferentiated perivascular cells, pulpal fibroblasts, or cells formed from the odontoblast lineage, but not exposed to the final epithelial influence.
Several hypotheses have been proposed to explain this phenomenon:
The obliteration of the pulp space can be seen as a response to a more or less marked restriction of the pulp's neurovascular supply which, after healing, leads to an increased deposition of dentine.1,8,16
It can be due to uncontrollable mineralization because of the failure of normal functioning of self-limiting pyrophosphatase enzyme.17 A reduced capillary permeability following the increased number of calcium ions could reduce serum flow within the dental pulp, resulting in a low concentration of inhibitory pyrophosphate ions.
A loss of the parasympathetic inhibition could cause a reduction in pulpal blood supply that could result in cellular respiratory depression, leading to pathological mineralization of the pulp and, eventually, obliteration of the root canal.18
Ten Cate19 identified this process as the deposition of tertiary or reparative dentine in response to irritation or trauma.
Avery20 postulated that this could be caused by a reduced vascular flow in the pulp, which has been observed during sympathetic nerve stimulation. This could then result in pulpal respiratory depression, ultimately leading to pathological mineralization and obliteration of the pulp canal.
Torneck21 hypothesized that the deposition of hard tissue is either a result of stimulation of the pre-existing odontoblasts or by loss of the regulatory mechanism.
Although the exact mechanism of CM is still unknown, it can be related significantly to the damage caused, following trauma, to the neurovascular supply of the pulp, as suggested by the first hypothesis.8,16 This, as a pulpal response to trauma, may lead to an increased deposition of dentine.
Clinical findings
Calcific metamorphosis is seen commonly among young adults, in the anterior region of the mouth8 and can be recognized clinically as early as 3 months after the trauma, but is usually detected after one year or so.2,8
Clinical appearance
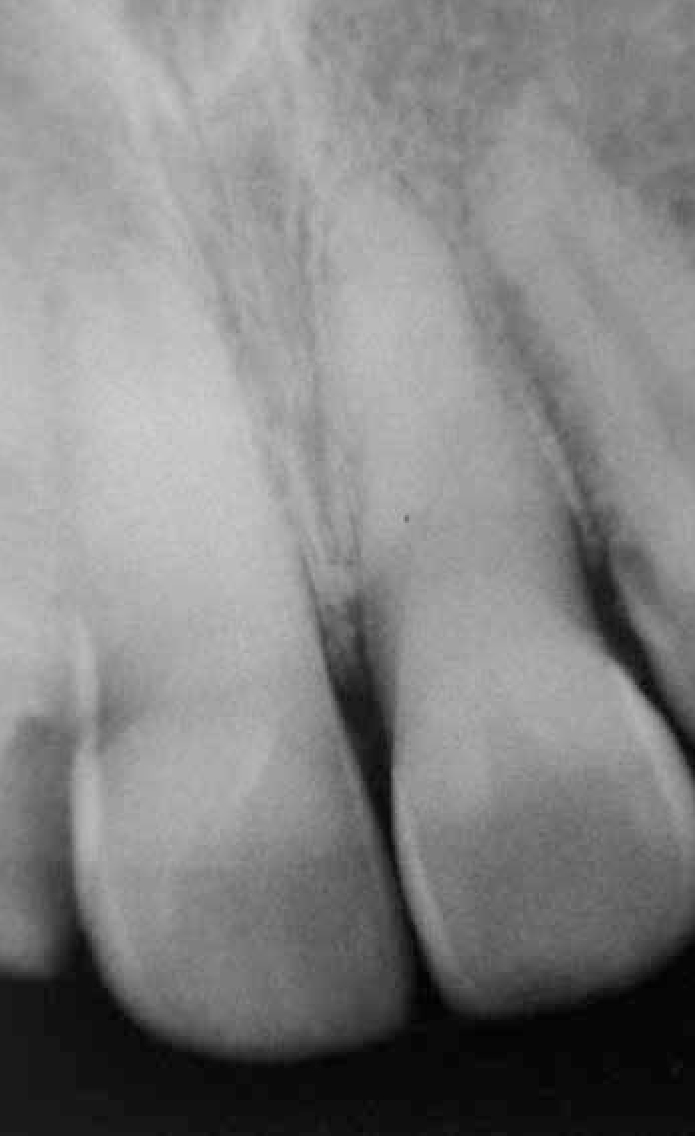
The tooth affected by CM is usually discoloured and may exhibit a darker yellow colour than the adjacent teeth (Figure 1). This may be due to the obliteration of the pulp canal space, the pulp cavity being filled with dark tertiary dentine, resulting in a tooth with a less translucent appearance.6,8,12
Figure 1. View showing the dark yellow colour discoloration of UL1.
Vital pulp testing
There are usually no responses to thermal testing (heat, cold) but the electrical test may elicit a delayed or, at times, normal response.1,7 Sensitivity to percussion is generally absent.
Symptoms
Teeth with CM may or may not have symptoms, depending on the status of pulp tissue within the mineralized canals (ie normal or infected). The latter case may eventually lead to apical periodontitis and the development of symptoms as it progresses.1,3,6,7,8
Radiographic features
The radiographic appearance of CM is obliteration of the pulp canal space with a normal periodontal membrane space and intact lamina dura (Figure 2).1,7,8 In cases associated with apical periodontitis, a thickening of the periodontal ligament space or peri-radicular radiolucency may be observed, with or without subjective symptoms.
Figure 2. Intra-oral periapical radiograph showing total pulp canal obliteration without any associated periapical changes.
Generally, the obliteration of the pulp canal spaces advances in a corono-apical direction. The first radiographic sign of obliteration is the decrease in the size of the pulp chamber, with no evidence of the usual chamber outline. This is followed by a gradual narrowing of the whole root canal. At times the canals may not be evident at all.7
Partial pulp canal obliteration (limited to the coronal part of the tooth).
Total pulp canal obliteration (extended to the coronal and radicular pulp canal spaces).
However, the differences in the frequency of partial or total obliteration of the pulp canal space are not statistically significant in relation to the injury type.12
Cone Beam Computed Tomography (CBCT)
Conventional radiographic examinations have inherent limitations, such as non-availability of 3D information and anatomic noise, which limit their use and relevance in endodontics. Among the various newly introduced technologies, CBCT has shown a promising use and application for endodontic purposes and management of endodontic problems.22,23
Working mechanics
CBCT utilizes an extra-oral imaging scanner to produce three-dimensional scans of the maxillofacial skeletal region. The synchronized 1800–3600 rotation of the sensor and the source around the patient's head acquires the 3D volume of data in a single sweep of the scanner.24 The X-ray beam is cone-shaped and captures a cylindrical or spherical volume of data. The large volume CBCT scanners can capture the entire maxillofacial skeleton, whereas the limited volume CBCT scanners capture a volume of data equivalent to the height and width of a periapical radiograph. Thus the limited volume CBCT scanners are best suited for endodontic imaging of only one tooth or two neighbouring teeth.23 Images can be displayed either in the three orthogonal planes (axial, sagittal and coronal) or as multiplanar reconstructions allowing virtual viewing of any view.
Advantages
The advantages of CBCT are as follows:
Accurate reproduction and measurement in 2D and 3D (voxels are isotropic);
Image accuracy;
Rapid scans; and
Area specific scanning for small regions.
It is simpler, less complicated and less expensive than CT scanners.23,25–28
Disadvantages
Disadvantages of CBCT images include:
A resolution less than conventional radiographs;
Increased radiological dose (equivalent to 2–3 periapical radiographs);
Scattering;
Beam hardening; and
Streak artefacts in the presence of metallic restorations (amalgam), metal posts and other prosthetic restorations.23,28–30
Therefore endodontic cases should be judged individually and until further evidence is available. CBCT should only be considered in situations where conventional imaging systems do not yield an adequate amount of information to allow appropriate endodontic treatment.
Diagnosing CM cases
As the image quality of CBCT scans are considered superior for assessing periodontal ligament, enamel, dentine and pulp, it is invaluable for the diagnosis and management of teeth with unusual root canal anatomy and conditions like calcific metamorphosis. CBCT has proved to be highly useful for localization and characterization of root canals, and the identification of untreated canals and unusual numbers of roots.22,30,31 Thus CBCT has a potential and promising role in the diagnosis and management of CM, as the exact location and anatomy of the root canal system can be assessed easily and accurately.32
Histological evaluation
It is not possible to determine the extent of mineralization from a clinical or radiographic examination.7 Complete radiographic obliteration of the root canal space does not necessarily mean the absence of the pulp or canal space. In the majority of cases, histologic evaluation of pulp canals that have been radiographically diagnosed as being totally obliterated almost always confirm the existence of a narrow pulp canal with pulp tissue.3,7,8 Hence the term mineralization is preferred to obliteration.7,33
Histological features
The histopathologic appearance of pulp canal obliteration shows three types of calcific tissue: dentine-like (49%), bone-like (19%), and fibrotic (9%).12,15
Holan31 observed tube-like structures extending along the entire length of the pulp canal and separated from the root dentine by normal pulp tissue but connected to the dentine in some of the sites evaluated. The structures had a histologic appearance of osteodentine, with cellular inclusions in ring-like formations.
Also, teeth with CM have failed to show any inflammatory component indicative of a pathologic process6,8,21 and the histological changes are characterized by an increase in collagen content and a varying decrease in the number of cells.2,15 Thus, based on these histopathological studies, teeth with CM do not indicate the necessity for root canal treatment.2,8,14,15
Complications
As, histologically, a narrow pulp canal almost always exists in a radiographically totally obliterated canal, a late complication after the obliteration of the pulp canal space is necrosis of the pulp.1,2 Though the exact pathogenesis of this complication is still not clear, caries, restorative treatment, inadequate crown restorations, new (secondary) trauma or other minor injuries can sever the already vulnerable vascular supply at the constricted apical foramen, along with continuous progressive occlusion of pulp vessels due to hard tissue formation.1 Several clinical investigations have recorded secondary pulp necrosis following pulp canal obliteration in 1–16% of cases.1,2,7,8,14 It has been reported that the incidence of pulpal necrosis increases over the course of time.12 In a recent clinical study, a higher incidence of pulp necrosis following CM has been reported.34 According to the study, 33% of pulp canal obliteration cases have been shown to develop periapical lesions with a negative reaction to sensibility testing.34 All cases of pulpal necrosis following CM are significantly related to teeth that were severely injured and to teeth with complete root formation at the time of injury.1,35
Earlier studies indicated that secondary pulp necrosis is more commonly observed in traumatized teeth with total pulp obliteration, and especially in those teeth which showed rapid obliteration after injury (ie total canal obliteration within two years after injury).1,35,36 However, a recent study by Oginni and Adekoya-Sofowora12 observed that teeth with partial obliteration (70%) of the pulp canal space are more likely to be symptomatic than those with total obliteration (21%).
Management
Management of CM involves the following treatment strategies:
Monitoring and observation: The advisable initial management of cases with CM is through periodic observation and endodontic examination. Regular monitoring of the traumatized tooth for at least five years is advocated.3
Aesthetic treatment: Usually, only bleaching of the involved tooth (one/single) can effectively resolve the discoloration issue in these cases. However at times, to obtain a more aesthetic outcome, veneers may be recommended for discoloured anterior teeth with large restorations (old), fractures or defects.
Endodontic treatment: As indicated by the histological studies, no significant inflammation has been observed in cases with CM that would warrant endodontic treatment. Endodontic intervention is only advised and indicated if peri-radicular pathosis is detected, or if the involved tooth becomes symptomatic.
Endodontic treatment
Based on the histological evaluation and considering the low incidence of pulp necrosis in teeth displaying CM, as opposed to old beliefs,37 routine endodontic intervention on teeth with CM is not recommended.1,38 Therefore, rather than considering it a prophylactic measure, endodontic treatment should be performed only in those cases where signs or symptoms of apical periodontitis appear.11,14,16 It should be initiated in teeth with tenderness to percussion, PAI (periapical index) scores ≥3 and a negative response to sensibility testing.35 Endodontic treatment can also act as a basis for internal bleaching (walking-bleaching) of discoloured teeth with or without apical periodontitis.1 Success in root canal treatment is based on proper debridement, cleaning and disinfection of root canal space of microbial contaminants and pulpal debris and their obturation (Figures 3–5). This may be clinically difficult to achieve in these cases owing to calcified pulpal space and root canals and the presence of the unusual canal morphology created by the calcification process.39 The prognosis of teeth with CM treated with non-surgical endodontic treatment has shown an overall success rate of 80–89%.1,40,41 The success rate for roots without periapical radiolucencies is reported to be 98% and with pre-operative periapical radiolucencies is 63%.41
Figure 3. Pre-operative radiograph showing calcified canals.Figure 4. Canal negotiation and working length determination.Figure 5. Post-operative radiograph – obturation.
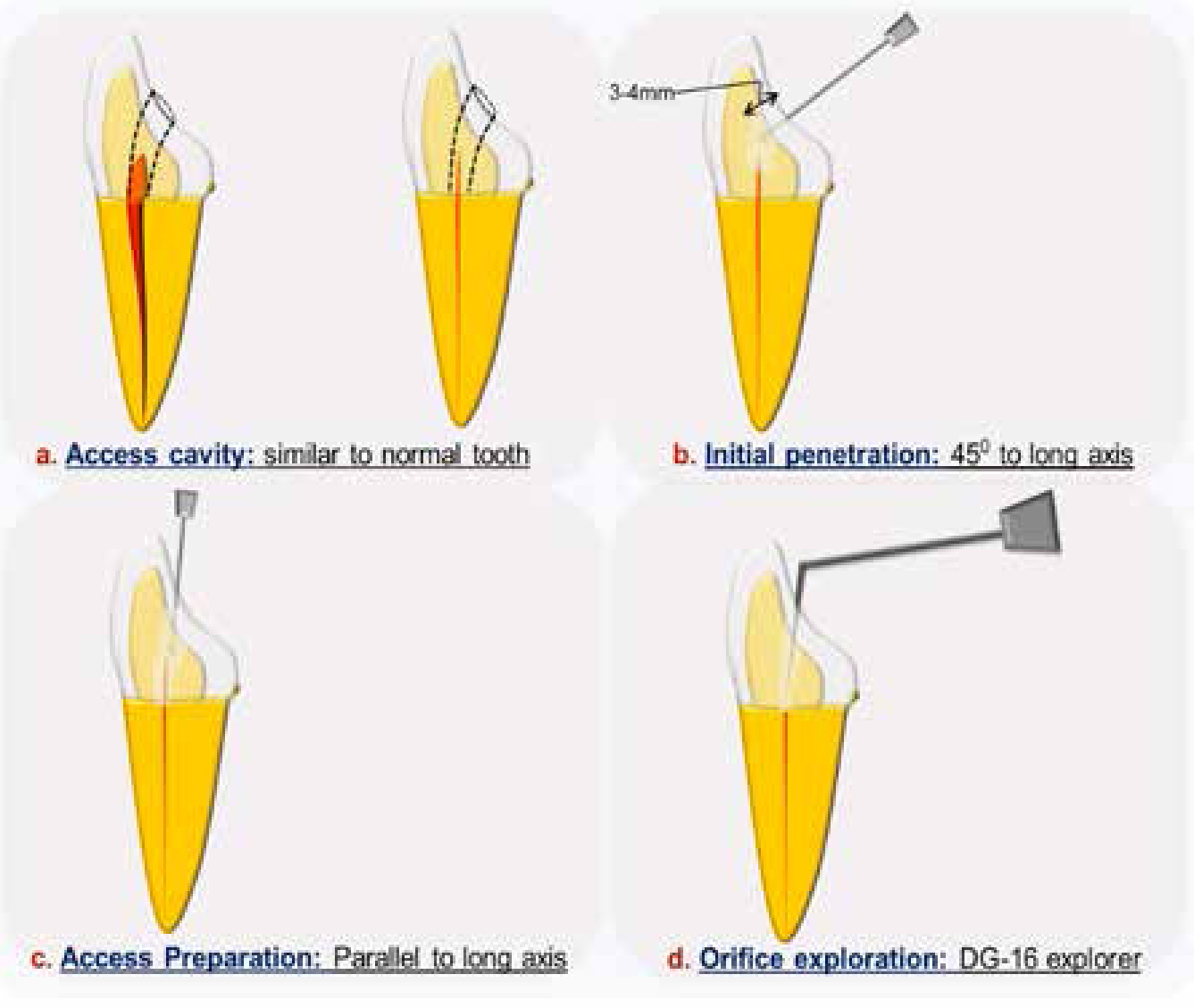
Figure 6. Schematic diagram depicting the steps in access opening.
The access cavity in these teeth should be of normal size and shape, similar to that opened in teeth with normal pulpal extension1,2,5,8 (Figure 6a). This helps to remove the dark tertiary dentine, thereby contributing to the translucency of the crown1 and an access cavity can be prepared in the crown to a depth equal to that of the pulp chamber floor in a non-calcified tooth. Secondly, it is equally important to be thorough with the normal root canal anatomy, geometric pattern of canal orifices, and their potential variations.8 If necessary, rubber dam should not be applied until the canal(s) have been identified to ensure that access cavity preparation is following the long axis of the roots.
Penetration
Long-necked round drills (LN-drill, Dentsply Maillefer, Oklahoma, USA) or long shank burs (tapered diamond) (LeBlond, FG burs, A&M Instruments, Inc, GA, USA) may be used with a gentle brush stroke action.5,8 Small long shank excavators or ultrasonic endodontic tips are also effective in removing the pulp mineralization and stones.42 An access cavity is started by penetration at 45° to the long axis (Figure 6b). However, continued penetration at the same angulations in calcified canals will result in perforation of the labial root surface below the gingival attachment. Therefore, if the canals are not located after 3–4 mm of penetration, the bur must be rotated parallel to the long axis of the tooth in order to prevent perforation (Figure 6c). In deep excavations, the bur may be changed to a long-shank No 2 round bur.8
Canal orifice exploration and identification
The most important instrument for orifice location and exploration is the DG-16 endodontic explorer (Hu-Friedy, Chicago, IL) (Figure 6d). Sometimes, a change in the colour of dentine in the centre of the root will indicate the position of the canal. Tertiary dentine overlying the canal entrances may be differentiated from physiological secondary dentine by its whiter/opaque appearance, compared to the yellow/grey colour of secondary dentine. Use of magnification devices (loupes and microscopes), transillumination, ultrasonics, contrast media, etc are equally helpful for locating the root canal orifices.1,2,5,8,43 An advantage of using ultrasonic tips (Figure 7) over burs for the location of mineralized canals is that they maintain high cutting efficiency without rotation, enhancing the safety and control over the instrument and reducing the risk of perforations. During the initial phase, larger size troughing tips with a limited diamond-coated extension should be used. Subsequently, thinner and longer tips should be used in deeper areas so as to maintain a clear vision. Sometimes a contrast medium can be used to disclose a root canal which was not seen in earlier radiographs. A cotton pellet soaked in contrast medium (10% potassium iodide) is placed in the access cavity and sealed with zinc oxide-eugenol cement. This facilitates penetration and easy visualization of canal orifices. Compared to unaided vision, the use of a magnification device, especially microscopes, enhances the visibility of the canal orifice and the root canal to a much greater depth, avoiding the unnecessary removal of tooth structure and chances of perforations. It is an easier and more precise method of locating the canal orifices.
Figure 7. Ultrasonic tips.
Radiographic confirmation of canal location
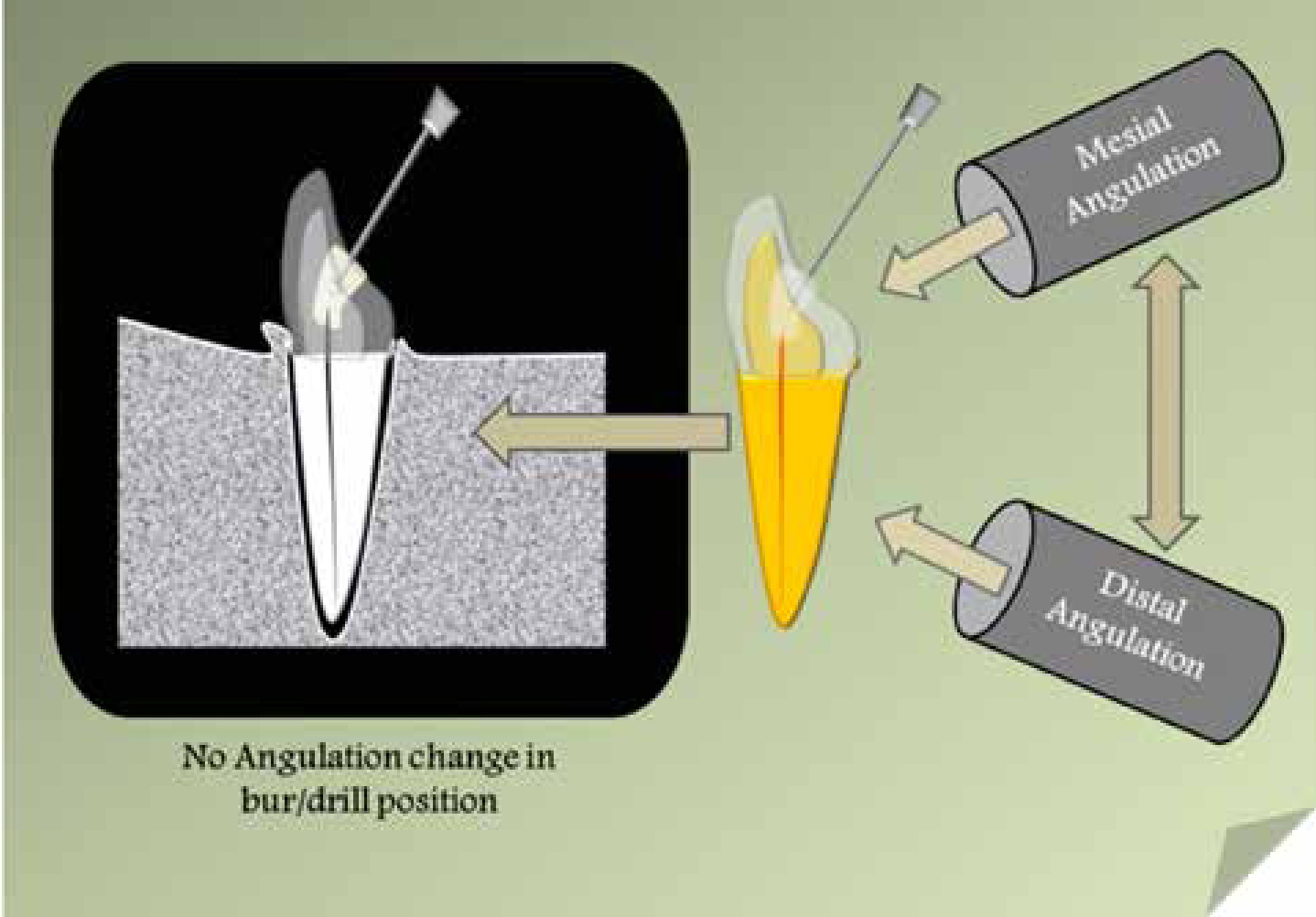
To reduce the chances of tooth perforation, it is proposed to take at least two radiographs at different angulations in order to establish and indicate the angulation of the bur/drill in the root and the position of the root canal (Figure 8). Usually, one straight angulation radiograph and another from either the mesial or the distal projection are taken. This is based on the hypothesis that the information provided by both distally and mesially shifted projections are identical. But this holds true only in cases where the bur head and the canal opening are farther apart. On deeper penetration of the bur, as the bur head becomes closer to the canal projection, the information gathered by considering only one projection, either mesial or distally, may be insufficient, misleading and incorrect.44 Therefore, in most of the cases, a third radiograph is obligatory.44 The first radiograph is straight-on, the second radiograph is taken with a 20° horizontal angle with the cone shifted distally, and the third radiograph also has a 20° horizontal angle with the cone directed mesially. The last two radiographs give information concerning the relation of the bur to the canal lumen in the bucco-lingual dimension. Using the information gathered by these radiographs, the bur is moved apically until the head of the bur and the orifice of the root canal being investigated come together. The problem of the large amount of radiation exposure involved in this method can be reduced by the use of fast films and the elimination of the exposure time.
Figure 8. Radiographic confirmation of canal location.
Canal negotiation
Once the orifice is exposed and the canal has been identified with a DG16 probe, a small file (06, 08 or 10 K file) with lubricant (Glyde, Dentsply Maillefer, Ballaigues, Switzerland) is placed into the orifice, and is used gently in watch winding action to negotiate the canal. Instruments like Canal Pathfinder (JS Dental, Ridgefield, CT), Pathfinder CS (Kerr Pearson Dental Supply Co. Sylmar, CA), or Canal Orifice Shapers (ProFile, Dentsply Maillefer, Ballaigues Switerzland) can also aid in canal negotiation as these can penetrate even highly mineralized canals. Rigid ‘C-Pilot’ hand files (VDW Endodontic Synergy, Munich, Germany) are also available that are specifically designed to negotiate mineralized canals. They have a cutting tip and are less likely to distort or buckle compared to regular stainless steel files.5
Though the use of chelating agents have been advocated for locating the difficult-to-find orifices by sealing them in the chamber between appointments,44 their clinical usefulness remains doubtful. These chelators fail to soften the mineralized pulp chamber for access to the patent root canal and can slightly alter the walls, thereby limiting the ability of instruments to be guided along the hard dentine. Thus, chelating agents are seldom of value in locating the orifice and can only be used to soften the canal after it has been located and during the canal preparation.5,8
Cleaning and shaping
Root canals may be cleaned, shaped and filled in the conventional manner.1 The following important points should be kept in mind during cleaning and shaping of mineralized canals:1,2,6,8
Use the thinnest possible file initially to negotiate the root canal up to the apical foramen. Too early a change to a larger file may lead to a false route or accumulation of dentinal debris in the root canal.
Advance instruments slowly in the calcified canals. Inspect before every re-insertion.
Irrigate copiously with 2.5–5.25% NaOCl (Oratech, LLC, Salt Lake City, Utah; NOVO, NOVO Dental Products Pvt Ltd, Mumbai, India). This lubricates the canal, dissolves the organic debris and keeps dentine chips suspended in the solution.
Use chelating pastes or solutions to assist in canal penetration, so as to facilitate widening of the canal. To avoid obturation of the canal with dissolved dentine, chelating agents (RC-Perp, Premier Dental Products, Plymouth Meeting, PA, USA) should be used only after the root canal has been reamed to the apical area.
Use ultrasonic instruments in the pulp chamber to loosen the debris.
Use a crown-down or hybrid technique to negotiate the canal space. This improves tactile perception in continued canal penetration.
The use of newer nickel-titanium rotary systems (ProFile, Dentsply Maillefer, Ballaigues Switerzland; Protaper, Dentsply Maillefer, Ballaigues, Switerzland) is highly useful and should be considered, when possible.
Surgical endodontics
Symptomatic teeth that exhibit complete CM radiographically, or cases in which the canals cannot be found and negotiated by routine endodontic treatment, are good candidates for peri-radicular surgery and subsequent retrofilling.45
Aesthetic/restorative treatment
As mentioned initially, a conservative aesthetic and/or restorative treatment is all that is required in most of the cases demonstrating CM. This includes procedures like bleaching, micro-abrasion and/or conservative veneer preparations. At times, a combination of two or more aesthetic procedures may be required to obtain the desired aesthetic outcome.
Discussion
Calcific metamorphosis or pulp canal mineralization is a clinically observed degenerative change in pulp following traumatic injuries like concussion and subluxation.7,8,34 This condition usually presents as dark discoloured teeth (yellow) with radiographic obliteration (total or partial) of the pulpal cavity (coronal and radicular). However, histologically, there is always the presence of some pulp tissue remnants, but without any inflammation. Thus, a routine endodontic intervention is not advocated for such cases and is only indicated in cases where the tooth is symptomatic with observed peri-radicular changes (16%).2,6,8 Location, negotiation, cleaning and shaping of these calcified canals is clinically possible. A proper use of long-shank burs, ultrasonic tips, endodontic explorer (DG 16), microscope or magnifying loupes, chelating agents (EDTA), hand and rotary endodontic instruments can yield an 80% clinical success rate for the endodontic treatment. In most of the cases, a conservative aesthetic and/or restorative treatment will be sufficient to restore the teeth and rehabilitate the dentition, both functionally and aesthetically. This usually includes bleaching, veneering or a combination of the two. It is advisable to do regular monitoring of a traumatized tooth for at least 5 years3 to assess and keep a check on the development of any new periapical changes in cases of recently traumatized teeth (1–2 years).
The most critical step in the treatment of such cases is thorough examination and a prudent diagnosis. This aids in planning a proper treatment protocol for the management of teeth involved with CM so as to achieve a clinically successful outcome.
Conclusion
As the incidence of pulpal necrosis following CM is quite low (1–16%), a conservative (aesthetic and/or restorative) approach is the preferred first line of treatment. Endodontic intervention is only required if the tooth becomes symptomatic with the development of peri-radicular pathosis.