Walmsley DA. Acrylic partial dentures. Dent Update. 2003; 30:424-429
Jacobson TE, Krol AJ. A contemporary review of the factors involved in complete dentures. Part III: Support. J Prosthet Dent. 1983; 49:306-313
Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers. A mixed longitudinal study covering 25 years. J Prosthet Dent. 1972; 27
Bergman B, Hugoson A, Olsson CO. A 25 year longitudinal study of patients treated with removable partial dentures. J Oral Rehab. 1995; 22:595-599
Orr S, Linden GJ, Newman NH. The effect of partial denture connectors on gingival health. J Clin Periodontol. 1992; 19:589-594
Stafford GD, Bates JF, Huggett R, Handly RW. A review of the properties of some denture base polymers. J Dent. 1980; 8:292-306
Nishii M. Studies on the curing of denture base resins with microwave irradiation: with particular reference to heat-curing resins. J Osaka Dent Univ. 1968; 2:23-40
Yannikakis S. Evaluation of porosity in microwave-processed acrylic resin using a photographic method. J Prosthet Dent. 2002; 87:613-619
Baemmert RJ, Long BR, Barco MT, Billy EJ. Effects of denture teeth on the dimensional accuracy of acylic resin denture bases. Int J Prosthodont. 1990; 3:528-537
Braden M. The absorption of water by acrylic resins and other materials. J Prosthet Dent. 1964; 14:307-316
Kalachandra S, Turner DT. Water sorption of plasticized denture acrylic lining materials. Dent Mat. 1989; 5:161-164
Woelfel JB, Paffenberger GC, Sweeney WT. Some physical properties of organic denture base materials. J Am Dent Assoc. 1963; 67:499-504
Pryor WJ. Injection moulding of plastics for dentures. J Am Dent Assoc. 1942; 29:1400-1408
Grunewald AH, Paffenbarger GC, Dickson G. The effect of moulding processes on some properties of denture resins. J Am Dent Assoc. 1952; 44:269-282
Nogueria SS, Ogle RE, Davis EL. Comparison of accuracy between compression – and injection-molded complete dentures. J Prosthet Dent. 1999; 82:291-300
Parvizi A, Lindquist T, Schneider R, Williamson D, Boyer D, Dawson D. Comparison of the dimensional accuracy of injection-molded denture base materials to that of conventional pressure-pack acrylic resin. J Prosthodont. 2004; 13:83-89
Cornell JA, Tucker JL, Powers CM. Physical properties of denture base materials. J Prosthet Dent. 1960; 10
Stafford GD, Huggett R, Cawston BE. Fracture toughness of denture base acrylics. J Biomed Mat Res. 1980; 14:359-371
Jagger DC, Harrison A, Jandt KD. Review. The reinforcement of dentures. J Oral Rehab. 1999; 26:185-194
Narva KK, Lassila LV, Vallittu PK. The static strength and modulus of fiber reinforced denture base polymer. Dent Mat. 2005; 21:421-428
Vallittu PK. Flexural properties of acrylic resin polymers reinforced with unidirectional and woven glass fibres. J Prosthet Dent. 1999; 81:318-326
Sung-Hun Kim, Watts DC. The effect of reinforcement with woven E-glass fibres on the impact strength of complete dentures fabricated with high-impact acrylic resin. J Prosthet Dent. 2004; 91:274-280
Vallittu PK. Acrylic resin fibre composite. Part II: The effect of polymerisation shrinkage of poly methylmethacrylate applied to fibre roving on transverse strength. J Prosthet Dent. 1994; 71:613-617
Vallittu PK. Glass fibre reinforcement in repaired acrylic resin removable dentures: preliminary results of a clinical study. Quintessence Int. 1997; 28:39-44
Provision of partial and complete dentures constructed from resin is commonplace and a satisfactory outcome requires the consideration of the properties of the resin, the oral tissues and prosthodontic principles. Conventional acrylic resin has been widely adopted as a popular denture base material since the 1930s. In this first of a two-part series, the benefits and shortcomings of acrylic resin are discussed alongside contemporary ‘enhancements’ to the material which can improve its properties. In the second part of the series, flexible and other alternative denture base resins, soft-linings, adverse effects of denture base materials and maintenance will be discussed.
Clinical Relevance: Knowledge of contemporary denture base resin systems will help to achieve optimal outcomes in removable prosthodontics.
Article
Luke J Rickman, Pavinee Padipatvuthikul and Julian D Satterthwaite
Despite increased oral health awareness amongst patients, acceptance of the ‘shortened dental arch’ concept,1 and technological advances such as implant therapy, there remains a demand for simple removable dentures in general dental practice. Complete dentures are conventionally constructed in acrylic resin and, although cobalt chromium partial dentures have many advantages in a variety of clinical situations, all-acrylic removable partial dentures are frequently provided by, and appear to be preferred by, many practitioners.2 Alongside conventional simple acrylic, many commercial laboratories offer ‘upgrades’, such as flexible, injection-moulded, high-impact and fibre-reinforced dentures. This two-part series offers a guide to when the selection of these options may be useful and discusses underlying factors influencing choice.
The ideal denture base material should:
Be biocompatible with the oral tissues;
Satisfy aesthetic demands;
Have sufficient mechanical strength to resist fracture under repeated occlusal and masticatory forces;
Be dimensionally stable to maintain fit and occlusion;
Resist abrasion and erosion;
Have colour stability;
Be radio-opaque so that they can be detected if some part of the denture is accidentally swallowed or inhaled;
Bond to artificial teeth;
Be rigid enough to distribute forces without damaging the supporting tissues and to maintain the occlusion;
Be easy to process, adjust and repair.
Underlying tissues
Maintenance of the supporting tissues in a physiologic condition is a priority when constructing complete or partial dentures, and changes can be caused by unequal and inappropriate distribution of normal functional forces and plaque accumulation around remaining teeth.
Edentulous areas
Certain areas of the edentulous arches, with heavy layers of cortical bone and resilient mucosa, are considered primary support areas, their characteristics resisting denture base movement, soft tissue trauma, and long-term resorptive changes (for example, the hard palate and buccal shelves of the mandible) (Figure 1). The remaining areas are designated secondary or non-support areas because of their decreasing ability to support the functional loads exerted upon them, owing to their progressively thinner cortical plate covered with soft tissue.3 The problems associated with ridge resorption have been studied extensively;4 minimizing the pressures in those regions most susceptible to resorption and directing the forces towards those regions best suited to support can help to maintain healthy residual ridges. Uncontrolled distribution of forces may result in point loading and loading of the tissues that are less able to tolerate the forces than those planned as primary support areas. Any method of reducing stress on the residual ridge is desirable and common methods are: correct extension of denture bases, reducing denture deformation by using a rigid material, and using tooth rests in partial denture designs (Figure 2).
Figure 1.
(a) Regions of the maxilla suited to denture support as described by Jacobson and Krol3: green = the hard palate is suited to primary support; yellow = the ridge crest is suited to secondary support; red = the peripheral tissues do not contribute to support; white = the midline suture usually requires slight relief (adapted from Jacobson and Krol 19833). (b) Regions of the mandible suited to denture support as described by Jacobson and Krol3: green = the buccal shelf and pear-shaped pad are suited to primary support; yellow = the ridge crest and genial tubercles are suited to secondary support; red = the ridge inclines do not contribute to support and may require relief (adapted from Jacobson and Krol 19833).Figure 2. Tooth support offered by occlusal rests on a cobalt chromium framework.
Teeth and periodontium
Partial dentures have an intrinsic potential for damage to the remaining teeth and periodontium. Classic studies have resulted in cobalt chromium dentures (with acrylic saddles) being considered the gold standard.5 When planned carefully, obtaining support from the teeth or both teeth and mucosa and, where possible, keeping gingival margins free, there is limited long-term alteration to the periodontium and natural teeth, and maintenance of good plaque control becomes the most important factor in success.
In reality, acrylic resin partial dentures are regularly prescribed in general dental practice because they are relatively cheap, easy to construct and adjust. However, acrylic is weak compared to cobalt chromium, and non-rigid and, therefore, must be bulky for strength. Unfortunately, this bulk often results in coverage of the marginal gingivae with the component parts of the denture, resulting in an increased area for plaque accumulation compared to the more skeletal metal frame designs. Additionally, acrylic is not suitable for occlusal rests to gain optimum support from abutment teeth, causing most all-acrylic dentures to be mucosa-borne. Therefore acrylic partial dentures carry a higher potential for soft tissue damage and periodontal breakdown due to both plaque formation and physical stripping. To limit the potential for damage, acrylic partial dentures should be kept free of the gingivae, where possible, and some tooth support can be obtained by finishing the acrylic above the survey line where it contacts teeth. Unfortunately, avoiding gingival contact by blocking out the dento-gingival junction does not appear to protect against deterioration of the periodontium.6 Components contacting the teeth, which are finished below the survey line and interdental acrylic wedges, can increase periodontal destruction owing to lateral forces on teeth and, therefore, although they may increase retention, should generally be avoided. This can be achieved efficiently if unwanted undercuts are blocked out, by the technician, on the master cast and wrought clasps are utilized for retention (Figure 3).
Figure 3. Acrylic partial denture kept free of the gingivae and retained by wrought clasps and guide planes.
Conventional acrylic
Polymethylmethacrylate (PMMA) resin has become the most popular material for denture bases, commonly utilizing a dough-moulding technique as introduced by Kulzer in the 1930s.7 PMMA is a glassy, hard, brittle acrylic. It is not an ideal material but has the following desirable properties:
It is colourless in its pure state, but easily pigmented and characterized;
It has adequate strength;
It has low water sorption and low solubility;
It is non-toxic;
It is easy to adjust, add to and repair; and
It is able to reproduce accurately, and retain indefinitely the features of a master cast, and is generally used with a simple moulding and processing technique.
Denture base acrylic (PMMA) is usually provided by manufacturers as a powder and a liquid which are mixed when ready for use: the liquid (monomer) plasticizes the powder (polymer) to a dough-like consistency which is packed into a mould prior to polymerization of the monomer by an addition reaction. Amongst other additives, the PMMA powder contains a copolymer (such as ethylacrylate) and a plasticizer (such as dibutylphthalate) that increase the solubility of PMMA pearls into the MMA liquid and, in high enough concentration, can yield soft acrylic for use as soft lining materials (discussed in the second part of this series).
Type of cure
Denture base acrylic (PMMA) is often categorized by method of curing. Light-cured, heat-cured (conventional or microwave) and cold-cured PMMA are available. In the UK, denture bases are commonly constructed from heat-cured PMMA, although cold-cured PMMA is more commonly used in some countries. In cold-cured PMMA the initiator (benzoyl peroxide) is activated by an amine accelerator found in the powder, at room temperature. In heat-cured PMMA the benzoyl peroxide initiator is activated by thermal decomposition at temperatures above 60°C. Typically, the heat-curing process takes approximately 7 hours in a water bath, although microwave polymerization, as first reported by Nishii in 1968,8 significantly reduces the processing time. Despite saving on time, the microwave process has not been widely embraced in the UK, owing to problems with increased porosity and reduced strength.9
Cold-cured PMMA has some disadvantages compared to heat-cured PMMA, such as significantly lower strength and oxidation of the amine accelerator, which results in reduced colour stability. However, cold-curing does have a few advantages: it may help to reduce the processing stresses introduced during heat-curing, thus resulting in improved accuracy, and also the processing time is considerably shorter, properties that make it the first choice for denture repairs. Light-cured PMMA is generally not used as a denture base material and is used for the production of items such as special trays.
Dimensional stability of acrylic (PMMA)
Heat-cured PMMA dentures undergo unavoidable dimensional changes during fabrication. Polymerization shrinkage has two main effects:
Slight distortion of the denture base (particularly the palate of maxillary complete dentures); and
Change in the position of the teeth, affecting the final occlusion.10
Closely following the manufacturer's processing instructions will keep the effects of polymerization shrinkage to a minimum and remounting of the dentures after processing will enable any new occlusal discrepancies to be corrected in the laboratory. As well as polymerization shrinkage, a further source of dimensional change in the conventional compression moulding and heat-curing process can be the flash resulting from overfilling of the mould. This is reduced by trial packing of the denture mould, but can result in a slight increase in the occlusal vertical dimension of the processed dentures.
Water uptake by processed denture base acrylic is facilitated by water storage, cleaning and the saliva of the oral environment. PMMA absorbs water slowly by imbibition and diffusion, until saturation (after around 17 days if stored in water at room temperature),11 resulting in an increase in weight of approximately 2%.12 Absorbed water can also plasticize PMMA, reducing its strength,13 however, these small changes in both dimension and strength appear to be of no clinical significance. Whilst water diffuses into denture base acrylic, residual monomer and additives can diffuse out. The consequences of this will be discussed in the second part of this series.
Injection moulded dentures
In 1942, Pryor14 adapted the technique of injecting unpolymerized acrylic into a mould for denture fabrication. A spring mechanism applied continuous hydraulic pressure to a reservoir of unpolymerized resin, resulting in a constant flow of new material from the sprue theoretically compensating for polymerization shrinkage. Although Pryor's technique was found to offer no significant advantages over conventional packing,15 and did not gain popularity, it was the pre-cursor to today's injection moulded dentures. In the mid 1970s, Ivoclar (Schaan, Liechtenstein) introduced an injection moulding system that used an acrylic resin modified for the injection moulding process. There have been various studies carried out on the system, and the literature generally supports the claim that current injection moulded denture base acrylic systems result in negligible dimensional changes and vertical dimension of occlusion compared to conventional compression moulding.16,17 However, in terms of clinical significance, there appears to be little advantage in selecting injection moulded acrylic, although time savings at the laboratory remount and occlusal correction stage may be made.
‘High-impact’ acrylic
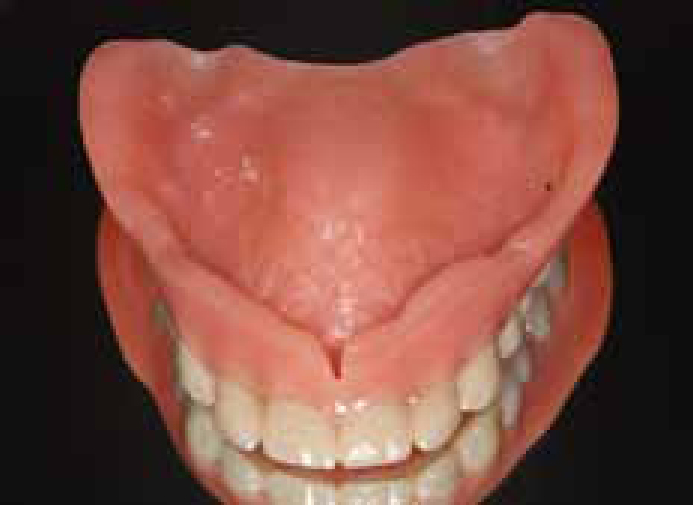
The cost to the NHS of repairing fractured dentures in England and Wales during 2004/05 (the most recent figures available) was over £3.6 million (Dental Practice Board Statistics, England and Wales). Perhaps this figure is slightly less surprising when considering that, owing to the forces of mastication, denture bases may flex close to 500,000 times per year,18 however, it is not clear whether most denture breakages occur during function or as a result of them accidentally being dropped. Deep notching at the mid-line labial fraenum and opposing natural teeth appear to be associated with an increased chance of fracture. Other risk factors include occlusal discrepancies, inaccurate fit, prominent tori, differential hardness of the supporting tissues, excessively thin sections of acrylic and processing errors. The brittle nature of conventional heat-cured PMMA can be modified by the incorporation of rubber to enhance its flexural properties.19 Since the flexure of denture bases is important, materials with enhanced flexural properties display greater survivability. Rubber-modified PMMA is known as ‘high-impact acrylic’: cracks in the material are difficult to initiate and their propagation is slow. Some commercial laboratories now provide ‘high-impact’ acrylic as standard, although this is not universal and many still consider ‘high-impact’ acrylic an ‘upgrade’ (Table 1) (Figure 4).
‘High-Impact’ Acrylic
Manufacturer
Enigma High-Base
Schottlander
Leucitone 199
Dentsply
Metrocryl HI
Metrodent
Figure 4. A maxillary complete denture with deep mid-line fraenum notch processed in ‘high-impact’ acrylic (Metrocryl HI, Metrodent).
Fibre-reinforced acrylic
The utilization of fibre reinforcements to improve the mechanical properties of denture base acrylic resin is well documented.20 Such fibres need to have good mechanical properties, be biocompatible, translucent and adhere well to denture acrylic so that forces can be effectively transmitted to them, otherwise the fibres act as inclusion bodies and essentially weaken the denture. Various types of fibre have been investigated as potential reinforcements for denture base acrylic, but glass and ultra-high molecular weight polyethylene (UHMWP) fibres have shown the most promise. UHMWP fibres are available in the UK as Ribbond (Ribbond, Seattle, USA), a fibre weave (Figure 5) that has been plasma-etched to improve wetting and adhesion to acrylic. However, the adhesion to PMMA remains relatively weak, which results in an insignificant increase in the mechanical properties of denture base acrylic.21
Figure 5. Ribbond (Ribbond) viewed under a light microscope.
Glass fibres can be adhered effectively to denture acrylic by silane coupling agents, resulting in significantly improved stiffness, flexural and impact strength.22,23 Good wetting of the fibres is essential for good adhesion, which can be compromised by polymerization shrinkage of the resin, leading to disruption of the fibres and decreased bond strength. Pre-treatment (‘impregnation’) of glass fibres with a thin PMMA–MMA slurry results in better wetting and, consequently, a greater reinforcing effect, yet avoids the exaggerated polymerization shrinkage and dimensional change that would occur if the fibres were wetted with monomer liquid alone.24
Position of fibre reinforcement
The concentration and position of fibres within the denture base are important. The concentration should be high for optimum strengthening. The high tensile strength of the reinforcing fibres causes them to be more effective when they are located close to the position of highest tensile stress under functional loading of a denture,21 for example, close to the oral surface of a maxillary complete denture and perpendicular to the midline. According to fibre geometries and ‘Krenchel's factor’, unidirectional reinforcement has the most efficient reinforcing effect.
Glass fibres are generally added to the polymer by hand, however, problems can arise with the lateral spreading of individual fibres (for example, Stick, StickTech, Turku, Finland) in the polymer matrix as acrylic resin is pressed in the mould causing an inhomogeneous distribution. Therefore, glass fibres are also available as woven sheets (for example, Stick PACK L, StickTech) which help to prevent drifting of the fibres (Figure 6). Distributing the fibres evenly throughout a denture is known as ‘total fibre reinforcement’ (TFR). Alternatively, a fibre-rich phase in the denture base polymer can form a separate structure known as ‘partial fibre reinforcement’ (PFR) which can be employed to strengthen dentures both during repair and in the manufacturing process.25 PFR facilitates easier placement of unidirectional fibres, which not only results in the most efficient reinforcing effect (see above), but also decreases the potential for fibre protrusion and tissue irritation.
Figure 6. Continuous and woven glass fibres.
Denture base aesthetics
Today's dental patients can have high aesthetic demands, and denture base resin systems are available which facilitate a closer match to patients' oral tissues than a ‘monoblock’ of conventional pink. The gingivae, mucous membranes, hard and soft palate, tongue and tissues of the floor of the mouth can exhibit pigmentation in people of all ethnic backgrounds. Conventional pink can sometimes be conspicuous, especially when patients have a high lip line. Some acrylic (PMMA) systems have colour tone kits (containing a range of finely ground pigments which can be chemically blended with the polymer powder) enabling characterization emulating both pigmentation and the subtle changes relating to the thickness and vascularity of the mucosa, for example Enigma Colour Tone Kit, Schottlander (Letchworth, England) (containing: ivory, light pink, natural pink, medium pink, dark pink, blue pink, light brown, dark brown) (Figure 7). Patient acceptability of upper complete dentures sometimes appears to be raised by the use of transparent acrylic over the vault of the palate, with pigment only incorporated in the ridges and flanges.
Figure 7. Characterization and pigmentation of acrylic gingivae.
Some manufacturers produce internally coloured denture base resins, for example, the flexible denture system Sunflex (Sun Dental Labs, Clearwater, FL, USA) has an accompanying shade guide allowing the clinician to match the denture base to the gingivae as closely as possible from a range of four shades or clear. Such flexible denture base resins have found popularity in the UK and will be discussed in part two of this series.
Summary
Before partial or complete denture provision, the underlying tissues and the properties of the material selected need to be carefully considered. Although acrylic does not perfectly match all of the properties of an ideal denture base material, it does have a good track record. Acrylic is hard enough to distribute loading evenly to the underlying tissues, is sufficiently dimensionally stable to produce dentures that fit accurately, and can be coloured and characterized to suit most patients' aesthetic demands. However, its brittle nature requires acrylic to be used in bulk which can raise the potential for damage to the periodontium when all-acrylic partial dentures are employed owing to limits that the material places on denture design. Whilst a chrome framework, with acrylic saddles, is the ‘gold standard’ of partial denture design, all acrylic partial dentures are common and careful planning can lead to designs which limit the risk of ‘gum-stripping’.
For both complete and partial acrylic dentures, ‘high-impact’ acrylic should always be preferred (over conventional PMMA) as it goes some way to resolving the problem of the brittle nature of PMMA. Practitioners with concerns regarding the increased cost of ‘high-impact’ acrylic could choose to employ it selectively in cases in which the risk of denture fracture is increased. Woven and unidirectional glass fibres can further improve the strength of acrylic, however, they are expensive, their addition by the technician is time consuming and their routine addition is largely unnecessary. However, for patients who repeatedly fracture their acrylic dentures, glass fibre reinforcement is worthy of consideration and ‘partial fibre reinforcement’ with longitudinal fibres is probably the most efficient and predictable method.