Hemingway CA, Parker DM, Addy M, Barbour ME. Erosion of enamel by non-carbonated soft drinks with and without toothbrushing abrasion. Br Dent J. 2006; 201:(7)447-450
Nunn JH. Prevalence of dental erosion and the implications for oral health. Eur J Oral Sci. 1996; 104:(2 Pt 2)156-161
Lussi A, Jaeggi T. Erosion – diagnosis and risk factors. Clin Oral Investig. 2008; 12:S5-S13
Ten Cate JM, Imfeld T. Dental erosion, summary. Eur J Oral Sci. 1996; 104:(2 Pt 2)241-244
Setchell DJ. Conventional crown and bridgework. Br Dent J. 1999; 187:(2)68-74
Berry DC, Poole DF. Attrition: possible mechanisms of compensation. J Oral Rehabil. 1976; 3:(3)201-206
Saha S, Summerwill AJ. Reviewing the concept of Dahl. Dent Update. 2004; 31:(8)442-447
Crothers A, Sandham A. Vertical height differences in subjects with severe dental wear. Eur J Orthod. 1993; 15:(6)519-525
Evans RD. Orthodontic options. Br Dent J. 1999; 186:(12)605-608
Dyer K, Ibbetson R, Grey N. A question of space: options for the restorative management of worn teeth. Dent Update. 2001; 28:(3)118-123
Saunders WP, Saunders EM. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:(3)137-140
Valderhaug J, Jokstad A, Ambjornsen E, Norheim PW. Assessment of the periapical and clinical status of crowned teeth over 25 years. J Dent. 1997; 25:(2)97-105
Cheung GS, Dimmer A, Mellor R, Gale M. A clinical evaluation of conventional bridgework. J Oral Rehabil. 1990; 17:(2)131-136
Hemmings K, Howlett J, Woodley N, Griffiths B. Partial dentures for patients with advanced tooth wear. Dent Update. 1995; 22:(1)52-59
Hemmings K, Darbar U, Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293
Redman C, Hemmings K, Good J. The survival and clinical performance of resin-based composite restorations used to treat localised anterior tooth wear. Br Dent J. 2003; 194:(10)566-572
Mizrahi B. A technique for simple and aesthetic treatment of anterior toothwear. Dent Update. 2004; 31:(2)109-114
Bartlett D, Sundaram G. An up to 3-year randomized clinical study comparing indirect and direct resin composites used to restore worn posterior teeth. Int J Prosthodont. 2006; 19:(6)613-617
Bartlett D. Using composites to restore worn teeth. J Canad Dent Assoc. 2006; 72:(4)301-304
Spreafico RC. Composite resin rehabilitation of eroded dentition in a bulimic patient: a case report. Eur J Esthet Dent. 2010; 5:(1)28-48
Robinson S, Nixon PJ, Gahan MJ, Chan MF. Techniques for restoring worn anterior teeth with direct composite resin. Dent Update. 2008; 35:(8)551-558
Allen EP. Surgical crown lengthening for function and esthetics. Dent Clin North Am. 1993; 37:(2)163-179
Ziada H, Irwin C, Mullally B, Byrne PJ, Allen E. Periodontics: 5. Surgical crown lengthening. Dent Update. 2007; 34:(8)462-478
Dahl B, Krogstad O, Karlsen K. An alternative treatment in cases with advanced localised attrition. J Oral Rehabil. 1975; 2:209-214
Poyser NJ, Porter RW, Briggs PF, Chana HS, Kelleher MG. The Dahl Concept: past, present and future. Br Dent J. 2005; 198:(11)669-676
Chana H, Kelleher M, Briggs P, Hooper R. Clinical evaluation of resin-bonded gold alloy veneers. J Prosthet Dent. 2000; 83:(3)294-300
Poyser NJ, Briggs PF, Chana HS, Kelleher MG, Porter RW, Patel MM. The evaluation of direct composite restorations for the worn mandibular anterior dentition – clinical performance and patient satisfaction. J Oral Rehabil. 2007; 34:(5)361-376
Management of generalized erosive tooth surface loss can be challenging. Careful pre-operative assessment of the patient and treatment planning is essential. The aim of any treatment provided is to prevent further tooth surface loss, restore aesthetics and function, and provide a stable occlusal relationship. Whilst attempting to fulfil these goals, it is important to protect the remaining tooth structure by using restorations which are conservative and do not cause further damage to teeth which are already compromised. This paper aims to describe a conservative approach to restoring patients with generalized tooth surface loss.
Clinical Relevance: To highlight conservative treatment options available for the management of generalized erosive tooth surface loss and show how they contrast with other destructive irreversible conventional techniques.
Article
Acid erosion is defined as the dissolution of dental hard tissues by acid derived from extrinsic and intrinsic sources (Tables 1 and 2) but not from bacteria which are part of the intra-oral flora.1 Erosive tooth surface loss is highly prevalent and a growing problem in terms of management.2 The 2003 survey of Children's Dental Health in the UK3 showed that 53% of 5-year-olds and a third of 12–15 year-olds showed signs of tooth surface loss which was predominantly erosive in nature. This was a 1–5% increase from the 1993 survey.4 The Adult Dental Health Survey in 19985 also showed that two-thirds of adults examined had signs of tooth surface loss into dentine on their anterior teeth and this was shown to increase with age. Tooth surface loss, which develops slowly with increasing age, is considered to be physiological, however, if a patient presents with tooth surface loss that is disproportionate to his/her age, or if the vitality of the tooth is threatened, then it is considered to be pathological and some intervention may be necessary to prevent further tooth surface loss or to restore the worn teeth.
Intrinsic Acid (Reflux of gastric acid)
Common causes:
Increased pressure on stomach from pregnancy, obesity or increased gastric volume from over eating or eating late at night
Voluntary repeated induced vomiting often associated with eating disorders such as bulimia nervosa and anorexia nervosa
Rumination syndrome – reflux of swallowed food for further mastication
- Hiatus hernia (weakening of lower oesophageal sphincter)
- GI tract disturbances (duodenal ulcer, chronic constipation)
- Chronic alcoholism
Side-effects of certain medications may induce vomiting or decrease buffering capacity of saliva due to drug-induced xerostomia
Vomiting caused by chemotherapy and radiotherapy treatment for cancer
Athletica nervosa – voluntary regurgitation in athletes to maintain body weight, eg race jockey
Extrinsic Acids
Alcohol
Wine, Beer, Alcopops, Cider, Spirit mixers
Soft drinks
Fruit juicesFlavoured waterCarbonated drinks (NB Carbonic acid is weak acid and itself does not cause erosion: it is other acids in soft drinks such as citric acid which cause erosion)Fruit flavoured teas/Herbal teasSports/Energy drinks, eg Lucozade sport, Red Bull, Maxim
Food stuff
PicklesFruits, eg oranges and lemonsVinegar-based foodsYoghurt-based foods
Medication
Vitamin C, Iron tablets
Environmental
Chlorine from swimming pools
Occupational
Working in acid environment
Erosive tooth surface loss
Management of tooth surface loss can be challenging, especially if extensive tooth tissue has been lost. An accurate diagnosis of the aetiology is important in identifying the causative factors and providing preventive advice to the patient prior to any restorative treatment being carried out. In most cases, there are often small elements of attrition and/or abrasion also present, making it a condition of multifactorial aetiology.6,7
A significant number of patients with erosive tooth surface loss will have no complaints or may be unaware of it. If the patient is unaware of the tooth surface loss, it is the responsibility of the dentist to make him/her aware of it and identify the cause at an early stage. Where the tooth surface loss is minimal and the patient has no complaints, management can be kept simple with preventive advice and monitoring using silicone indices, photographs and study models. Patients with more advanced tooth surface loss may present with an aesthetic concern or complaining of functional problems due to the loss of stable occlusal contacts. The majority of these patients do not complain of sensitivity, but those that do may have ongoing erosive tooth surface loss where the teeth are being exposed to a highly frequent rate of acidic challenge.8 Patients with advanced tooth surface loss will require some form of intervention to protect the remaining tooth structure and, in most cases, restore their worn dentition to improve the aesthetic appearance and provide a stable occlusal relationship in order to improve function. The extent of tooth surface loss can be either localized to a few teeth or generalized to involve most of the teeth in both the maxilla and mandible.
Erosive tooth surface loss can affect any tooth surface.9 Early erosive lesions may show smooth silky-glazed or dull enamel surfaces with the absence of perikymata. Moderate cases often show cupping defects and advanced lesions present with most of the enamel being lost, however, there is often an intact ring of enamel which remains around the gingival margin.8 These lesions are usually well into dentine, often into tertiary dentine.
Patients with generalized tooth surface loss rarely appear to have lost any occlusal vertical dimension, despite the significant generalized loss in clinical crown height.10 This is often due to the fact that erosive tooth surface loss is usually a slowly progressing condition which allows time for compensatory alveolar down growth of the maxilla to occur.11 In patients where the tooth surface loss is active and rapidly progressing, this compensation may not be fast enough and can result in the patient presenting with a reduced lower face height due to loss in occlusal vertical dimension.12 Patients with localized tooth surface loss also maintain their occlusal vertical dimension, but often lose interocclusal space between the worn teeth through localized alveolar compensation11 and over eruption of the worn and opposing teeth. This is often seen in patients who have wear of their anterior teeth.13,14
Treatment options
Various restorations are available for restoring teeth with tooth surface loss. Traditionally, a combination of metal ceramic crowns, porcelain veneers and gold crowns have been shown to be successful in restoring function, aesthetics and occlusal stability.15 The biggest disadvantage of these cast restorations is that they are comparatively destructive to the already worn teeth and can also result in the loss of vitality of these teeth.16-18 It is often difficult to explain to the patient that treatment of his/her tooth surface loss will involve further removal of healthy tooth tissue.10 In severe cases of erosion, a removable prosthesis may be considered.19 This can be in the form of complete or partial overdenture, onlay denture or overlay denture. Whilst these are non-destructive to tooth tissue, they can be technically difficult to make and patients may prefer to have a fixed replacement. With advances in bonding techniques, the use of composite resin has recently become popular, particularly for the restoration of localized anterior tooth surface loss,20-22 however, there is very little literature on the use of composite for building up posterior worn teeth.23-25 This article presents a case of generalized tooth surface loss which has been predominantly restored with composite resin and minimal preparation gold onlays on the lower first molars.
Case report
A 26-year-old male presented to the clinic with an aesthetic concern and also complained of sensitivity to hot and cold from his teeth. Following history and clinical examination, a provisional diagnosis of active erosive tooth surface loss was made. Further investigation with a diet sheet highlighted that the primary aetiological factor was the consumption of a litre of carbonated Cola per day. There was also some history of previous acid reflux and heartburn.
From the extra-oral examination it was noted that the patient showed none of the upper anterior teeth with the upper lip at rest but, when the patient smiled, the gingival margins were slightly visible around the anterior teeth due to some alveolar compensation (Figure 1). The horizontal incisal plane appeared flat (Figure 2) and no longer followed the curvature of the lower lip.
Figure 1. Patient with high lip line which shows the entire tooth and some of the gingival tissues.Figure 2. Patient's incisal plane is flat (red line) and does not follow curvature of the lower lip. Increased gingival display suggests that there has been some alveolar compensation in the upper arch.
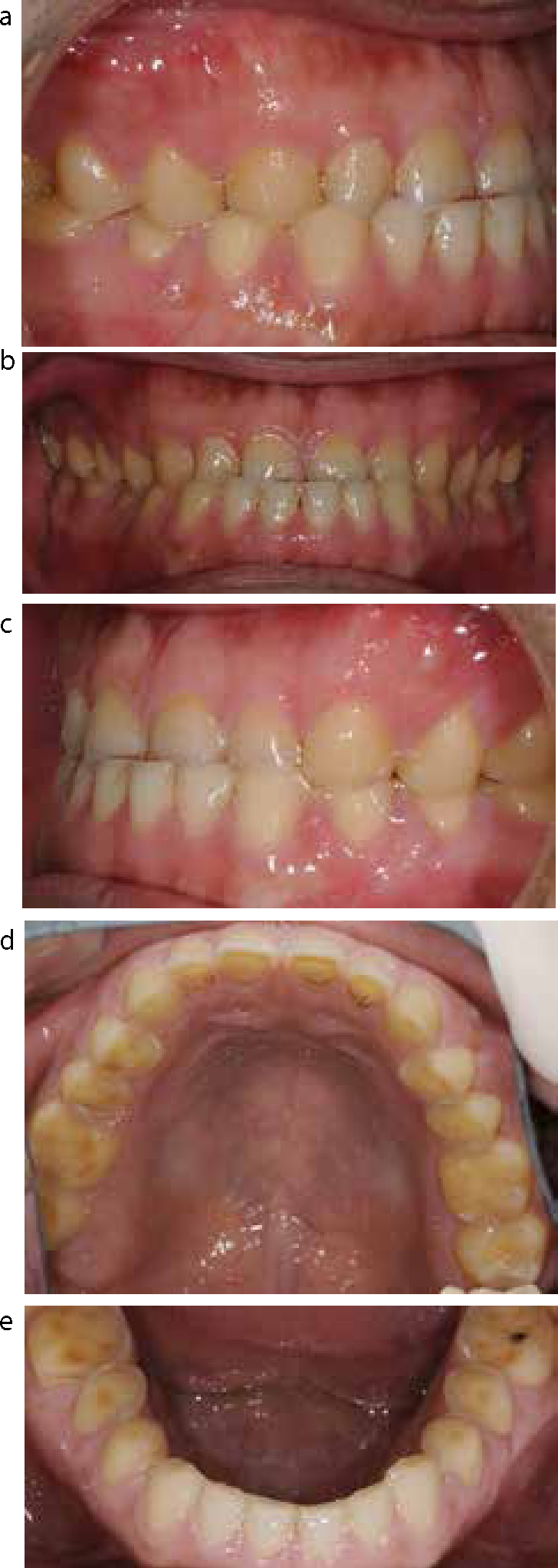
Intra-orally the tooth surface loss was generalized, involving all the teeth in both arches and extended into dentine (Figure 3). Anteriorly, there was also thinning and chipping of the incisal edge resulting in reduced clinical crown height (Figure 2). In occlusion, the patient appeared to have a very slight decrease in lower face height due to some loss in occlusal vertical dimension which had not fully been compensated for by alveolar down growth of the maxilla. This, along with the fact that the patient was getting sensitivity to hot and cold, suggests that there was some active erosion taking place which was resulting in rapid tooth surface loss. There was an obvious discrepancy noted between the patient's intercuspal position and the retruded contact position. In the intercuspal position, the patient had developed a Class III incisal relationship. This was due to the patient posturing the mandible forwards in order to maintain contact between the worn anterior teeth.
Figure 3.
(a–e) Pre-operative intra-oral views.
Case management
Initially, a discussion took place with the patient with regards to diet and prevention. The patient was advised to reduce the amount and frequency of carbonated drinks he was consuming, restrict them to meal times only and use a straw to prevent any further erosive tooth surface loss. Whilst the patient was not aware of any active heartburn or acid reflux taking place, owing to the past medical history, the patient's general medical practitioner was also contacted to investigate further the possibility of silent acid reflux.
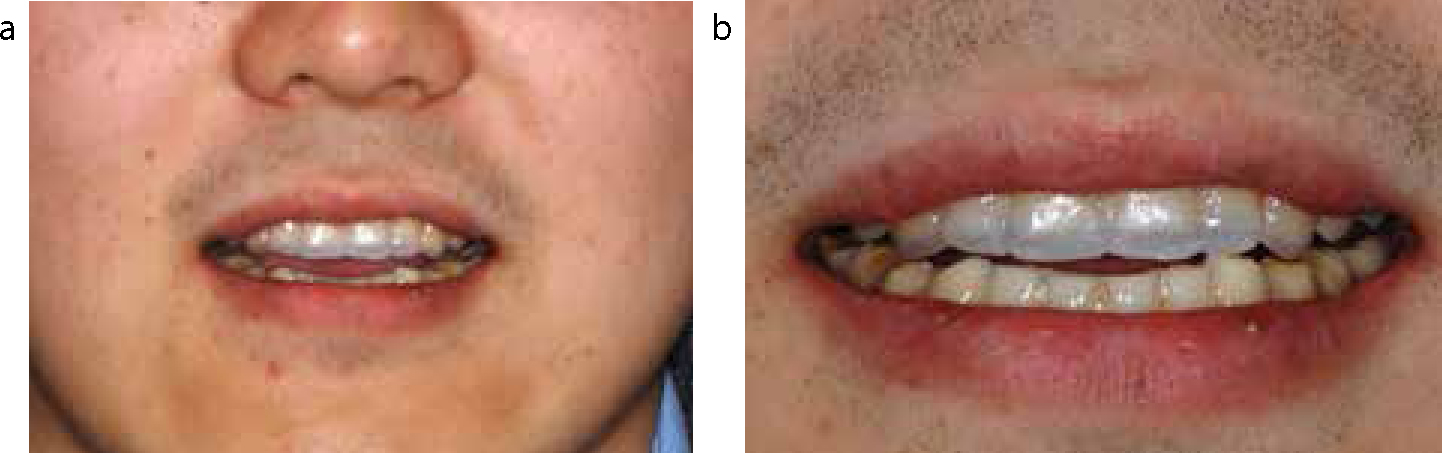
Following preventive advice, both the patient and clinician agreed that the tooth surface loss was advanced enough to consider some form of restorative treatment to restore the worn teeth and protect them from further tooth surface loss. Restorative treatment options were discussed with the patient which included, the use of direct and indirect composite resin, porcelain fused to metal crowns, all-ceramic and gold crowns or onlays. The patient's tooth surface loss was not extensive enough to consider a removable prosthesis. The use of composite resin to replace the worn tooth structure, restore aesthetics and function, whilst protecting the remaining tooth structure, was explained to the patient in detail. The patient was informed that this is the most conservative form of treatment and alternative treatment would involve crowning several teeth, which is more destructive. In order to explain the aim of the treatment visually, a chairside aesthetic preview was carried out using orthodontic wax (Figure 4). This technique involved adding orthodontic wax to the upper anterior six teeth to make them roughly the ideal size and shape, based on the clinician's experience and knowledge of average tooth dimensions. This allowed the patient to see what restorative treatment with composite resin could offer and also gave the clinician an idea of how much the anterior teeth needed to be built up to restore aesthetics, with teeth of ideal size and shape and the incisal plane following the lower lip line. This simple form of chairside aesthetic preview also helped in giving the laboratory a detailed prescription for the diagnostic wax-up in terms of how much each tooth needs building up and how much increase in occlusal vertical dimension is required to achieve this result. The patient was happy with the appearance of the mock up and was keen to go ahead with the composite build-ups to restore his worn dentition.
Figure 4.
(a, b) Chairside aesthetic preview created using orthodontic wax at initial assessment visit.
Impressions, facebow record and an interocclusal retruded arc of closure record was taken at the estimated increase in occlusal vertical dimension. Articulated study models and a diagnostic wax-up were made. This was shown to the patient and the final treatment plan agreed.
A Memosil (Heraeus Kulzer, GMBH) index (Figure 5) was made from the diagnostic wax-up for each arch, which was used to help guide restoration of the anterior teeth with composite resin based on the matrix technique described by Robinson et al.26 Prior to restoring the teeth with composite resin, the teeth were bevelled and cleaned with pumice to remove the salivary pellicle. Initially, all four canine teeth were restored to establish the new occlusal vertical dimension and restore canine guidance in lateral excursions. This was immediately followed by restoration of the upper and lower incisor teeth and placement of temporary composite stops (Figure 6) on the premolars and molars to maintain the interocclusal space created by increasing the occlusal vertical dimension. The use of a matrix allowed the palatal contour and incisal length of the teeth to be mapped out accurately with enamel shade composite as per the diagnostic wax-up. This was then used to guide the subsequent placement of the dentine shade of composite. In order to prevent bonding composite to the adjacent teeth, the initial enamel composite layer on the palatal surface built using the matrix was kept shy of the contact points. Following placement of the dentine shade composite, the interproximal contact points were created using enamel shade composite and a cellulose strip wrapped over the palatal surface. The final enamel layer was then placed to finish the restoration. Using the matrix to recreate the contour of the palatal surface as per the diagnostic wax-up also helped in developing a stable occlusal relationship, which required minimal adjustment to ensure even occlusal contacts on all the restorations. Once the anterior teeth in both arches were complete, the premolars and the upper molar teeth were built up using a combination of the matrix technique and a free-hand build-up technique, also described by Robinson et al.26 The lower first molars were restored with lab-made gold onlays which were cemented using Panavia (Kuraray Dental). All the composite restorations were completed by maintaining moisture control using a combination of cotton wool rolls, a tongue guard salivary ejector and educating the patient on the importance of keeping the area dry. Maintaining adequate moisture control to build-up the lower molars in composite was difficult and therefore it was decided to restore these teeth with minimal preparation gold onlays. The direct composite used was Esthetix with Prime and Bond NT bonding agent (Dentsply, Germany). Figures 7 a–h show the post-treatment views of the final restorations.
Figure 5.
Memosil index made from the diagnostic wax-up to guide composite build-ups.Figure 6. Example of a composite stop placed on the posterior molars whilst the anterior teeth are being restored.Figure 7.
(a–h) Post-treatment views of the final restorations.
Discussion
Before any restorative treatment is commenced it is important to identify the cause of tooth surface loss as this can help when deciding how to restore the worn teeth. For example, patients who have worn their teeth through clenching or grinding (attrition) will need restorations that can withstand increased occlusal forces. These patients also need to understand that they are more likely to fracture or damage restorations compared to someone with erosive or abrasive tooth surface loss. For these reasons, these patients may be better treated with crowns or a combination of adhesive composite restorations with a few crowns or onlays on strategically selected teeth, such as canines, premolars and/or molars which may help to restore guidance and take excessive forces off the adhesive restorations. In comparison to this, someone who has lost tooth tissue through acid erosion can, theoretically, be restored using adhesive techniques and composite resin, as they are unlikely to generate increased occlusal forces which could shear off the restorations.
Clinical assessment
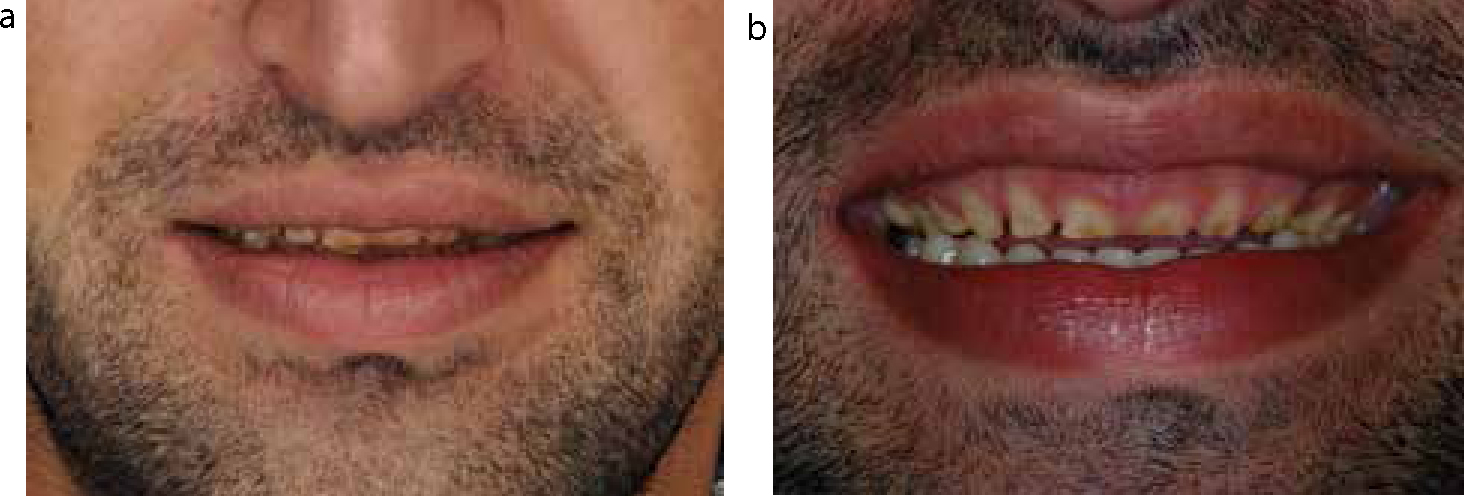
During the clinical assessment it is important to assess the patient both extra-orally and intra-orally in detail. Extra-oral examination allows the assessment of the amount of incisal display with upper lip relaxed and while the patient is talking and smiling. If the patient has no incisal tooth display with upper lip relaxed then there may be some scope to increase the length of the incisor teeth with the final restoration. If there is already a few millimetres (mm) of incisal tooth display with the upper lip relaxed, as shown in the patient in Figure 8a, or significant soft tissue display when the patient smiles (Figure 8b) (often seen when there is alveolar compensation associated with tooth surface loss), then it may not be possible to increase the length of the teeth. Increasing the length of the teeth through the restoration in this scenario would result in too much incisal display when the lip is at rest, making the teeth appear as if they are too long, often giving a poor aesthetic appearance. Instead, it may be more appropriate to carry out crown lengthening surgery27,28 to lengthen the clinical crown height, reduce the ‘gummy’ nature of the smile and restore the teeth to the ideal length for the patient. In some cases, a combination of increasing the length of teeth by a few mm and a few mm of crown lengthening surgery may be necessary. The patient in the case presented here does have a high smile line with some gingival display (Figures 1 and 2). However, owing to the lack of incisal tooth display when the upper lip is at rest, it was possible to build the teeth up and avoid the need for crown lengthening surgery without making the teeth look too long. The pre-operative aesthetic preview which was carried out helped in making this decision. The post-operative view (Figure 7a) also shows that the incisal plane has been restored so that a line drawn along the incisal edges of the upper anterior teeth would be of a similar curvature to the lower lip, which appears more aesthetic when compared to the flat incisal plane seen in Figure 2.
Figure 8.
(a, b) Example of a clinical case where crown lengthening surgery is necessary.
Creating interocclusal space for restoration of worn teeth
The intra-oral examination will highlight if the wear is localized to a few teeth or generalized and whether interocclusal space is available or not. In localized wear of the anterior teeth, if space is available this can be used simply to restore the teeth without the need for tooth preparation or an increase in the occlusal vertical dimension. When interocclusal space is not available, usually due to a combination of alveolar compensation and overeruption of worn and opposing teeth, space needs to be created.
Tooth preparation is one method of creating space. However, this should be avoided as it is destructive to an already compromised tooth. Examination of the patient's occlusion should be carried out to see if the occlusion can be reorganized by manipulating the patient's mandible into a retruded contact positon.15 This can often create space anteriorly which can be used to restore the localized anterior wear. Creating even contacts between the restorations and opposing teeth will hold the mandible in the retruded contact position, making this the patient's new intercuspal position. In some cases where the retruded contact position is coincident with the intercuspal position, or if there is only a small difference between the two, it may not be possible to create space as described above. In these cases, space can be created using the Dahl principle.29 Originally, Dahl's work involved the use of an anterior cast cobalt chrome removable bite plane (Dahl appliance) which, when inserted, caused disclusion of the posterior teeth. Over an average of 6–9 months, the posterior teeth re-established contacts through a combination of relative intrusion of the anterior teeth and overeruption of the posterior teeth. As a result, interocclusal space was created anteriorly which could be used to restore the worn teeth. This technique, over time, has been described as the Dahl principle.30 The Dahl appliance itself has been developed since it was first described, with many authors advocating the use of direct composite restorations on the upper anterior teeth. These restorations are placed at an increased occlusal vertical dimension with even occlusal contacts with the opposing anterior teeth in the retruded arc of closure. This results in disclusion of the posterior teeth,12,21,22 which over an average of 4–9 months often come back into contact through relative tooth movements, as described above, avoiding the need for any further treatment.30
In cases of generalized tooth surface loss, restoring only the anterior teeth is generally not enough and restoration of the posterior worn teeth is also often required. In this situation, the patient may require complete reorganization of the occlusal scheme at an increased occlusal vertical dimension to create space in the retruded arc of closure. The case presented here has been restored in this manner with a combination of direct composites and gold onlays.
Staging of treatment
When carrying out full-mouth rehabilitation, as shown in the case presented here, careful planning is important to ensure accuracy of the new occlusal scheme. In order to achieve this, it is important to carry out the treatment in stages over several visits in a short period of time. Building up strategic teeth (often the canines) in each quadrant initially is important to establish the new occlusal vertical dimension and a stable mandibular position. Once this has been done, the rest of the anterior teeth can be restored one by one as quickly as possible to prevent any uncontrolled/unfavourable tooth movement. Often, for the same reason, while the anterior teeth are being restored, it is worth placing temporary composite stops (Figure 6) on the posterior teeth to maintain the interocclusal space as it can be a while before the posterior teeth are restored. If the created space between the posterior teeth is not maintained, then restoration of these teeth may require preparation of the teeth to create more interocclusal space. As mentioned before, this is highly destructive to an already compromised tooth.
Composite resin and tooth surface loss
Indirect restorations are far more destructive to tooth tissue but less technique sensitive compared to composite resin. When using composite, the clinician needs to be able to maintain adequate moisture control as well as having the artistic flare to create tooth-like composite restorations. Although it would be desirable to use a rubber dam, it can be difficult when building up worn teeth with composite. Often, in the upper arch, moisture control is well maintained using cotton wool rolls, salivary ejectors, gauze squares and good patient co-operation. Maintaining moisture control in this way can be difficult in the lower arch, particularly the posterior parts in the lower arch. Where adequate moisture control cannot be achieved, either with the use of rubber dam or other techniques, composite resin should be avoided. Alternative indirect restorations should be considered where control of moisture is not required for such long periods of time. In this case, gold onlays with minimal preparation were placed on the lower molars. Chana et al31 showed that these restorations are often successfully used in the posterior parts of the mouth where aesthetics is not a priority and where moisture control can be difficult to achieve.
There is very little literature on the longevity of composite resins. The best available evidence shows that composite resin used to restore anterior worn teeth has a success rate of 89.4% over a mean 30-month follow-up period.20 Poyser et al32 also found only a 6% complete failure rate of composite restorations on worn lower anterior teeth over a 2.5 year follow-up period and Redman et al21 showed survival rates of over 4.5 years with direct anterior composites. The main causes of failure were due to the composite wearing away over time and marginal discoloration.
Conclusions
The aim of managing the worn dentition should be to protect the remaining tooth structure whilst restoring function, occlusal stability and aesthetics. From the patient's point of view, the most important factor is often the aesthetic appearance of his/her teeth. In order to achieve these goals, a minimally invasive approach is preferred and the use of direct composite restorations is well suited to this. Using composite to restore generalized erosive tooth surface loss early on in the treatment leaves the option of more invasive restorations for the future, if necessary. The use of composite resin, as shown in the case here, avoids, or at least delays, the patient entering a destructive restorative treatment cycle. Composite restorations also provide good aesthetics, are easy to repair if they fracture and can easily be refurbished by polishing if they discolour over time. Despite the lack of long-term evidence for longevity of these restorations, the abovementioned benefits should place composite towards the top of the list when planning treatment for patients with erosive tooth surface loss.