Rudolphy MP, van Amerongen JP, ten Cate JM. Radiopacities in dentine under amalgam restorations. Caries Res. 1994; 28:240-245 https://doi.org/10.1159/000261972
Rudolphy MP, Gorter Y, van Loveren C Progression of radiopacities and radiolucencies under amalgam restorations on bite-wing radiographs. Caries Res. 1997; 31:19-23 https://doi.org/10.1159/000262368
Mua B, Barbachan E, Silva B Radiolucent halos beneath composite restorations do not justify restoration replacement. Am J Dent. 2015; 28:(4)209-13
Fröhlich TT, Nicoloso GF, Lenzi TL The Thickness of the adhesive layer increases the misdiagnosing of the radiolucent zones and restoration replacement indication. J Esthet Restor Dent. 2017; 6; 29:193-200 https://doi.org/10.1111/jerd.12297
Kidd EA, Joyston-Bechal S, Beighton D. Marginal ditching and staining as a predictor of secondary caries around amalgam restorations: a clinical and microbiological study. J Dent Res. 1995; 74:1206-1211 https://doi.org/10.1177/00220345950740051001
Kidd EA, Beighton D. Prediction of secondary caries around tooth-colored restorations: a clinical and microbiological study. J Dent Res. 1996; 75:1942-1946 https://doi.org/10.1177/00220345960750120501
Lino JR, Ramos-Jorge J, Coelho VS Association and comparison between visual inspection and bitewing radiography for the detection of recurrent dental caries under restorations. Int Dent J. 2015; 65:178-181 https://doi.org/10.1111/idj.12172
Hewlett ER, Atchison KA, White SC, Flack V. Radiographic secondary caries prevalence in teeth with clinically defective restorations. J Dent Res. 1993; 72:1604-8 https://doi.org/10.1177/00220345930720121301
Burke FJT, McKenzie L. Bonding to dentine: an update on universal adhesive. Dent Update. 2021; 48:620-631
Mercer J, Bloom R. Fools rush in. Recorded by Rick Nelson1940.
Grey Areas in Restorative Dentistry: Part 4. Mind the Gap 1: The Radiographic Space between Restoration and Tooth Robert L Caplin Dental Update 2025 52:2, 148-150.
Authors
Robert LCaplin
BDS, MSc, DGDP (RCS Eng), Dip Teach Ed (King's), Retired Senior Teaching Fellow, Faculty of Dentistry and Oral and Craniofacial Sciences, King's College London; General Dental Practitioner, London
Radiopacities and radiolucencies beneath restorations provide the dental practitioner with diagnostic challenges as to the nature of such findings. Understanding the possible aetiologies of these radiographic appearances is essential for their subsequent management to avoid unnecessary intervention.
CPD/Clinical Relevance: Radiographic changes around restorations are a relatively common finding and require the practitioner to decide whether to supervise or intervene.
Article
Those familiar with the London underground system might be aware of announcements at some stations to ‘mind the gap’. This occurs at curved stations where a gap will exist between the stationary carriage and the platform, posing a potential threat of harm by falling into the space if the danger is not recognized.
The dental ‘gap’ is the one that is visible on radiographs between a restoration and tooth tissue and which, without thought by the practitioner, can lead to harm for the patient: the dentist can ‘fall’ into the apparent space.
The practitioner must determine, as best possible, what is going on beneath the restoration, i.e. what is the nature of the radiographic change, and should be aware that active caries is not the only conclusion at which to arrive. The actual radiographic appearance of an area varies from grey to black to white, as radiolucencies or radiopacities, and this should be taken in tandem with the clinical findings. The radiopacities are caused by tin or zinc deposits in partially demineralized dental tissue and may be seen under amalgam restorations. These radiopaque zones consist almost entirely of irreversibly demineralized dentine.1
Rudolphy et al,2 when looking at the progression of radiopacities and radiolucencies under amalgam restorations on bite-wing radiographs, found the following:
Over a 6-year period, all radiopacities remained the same;
Some radiolucencies enlarged, but a substantial number did not;
Some combinations of radiolucencies and radiopacities enlarged, but a number did not.
The clinical implications of this study are:
Radiopaque areas are not a reason for replacement of fillings;
There should be a radiographic review every 6 years;
One should be aware of any radiolucency between a restoration and a radiopaque area, because of possible caries progression;
Fillings with radiolucencies beneath them need not necessarily be replaced.
A similar conclusion was reached by Mua et al3 when assessing radiolucent halos beneath composite restorations. They concluded ‘radiolucent areas beneath restorations are not indicators for restoration replacement. When no clinical signs indicating a loss of marginal integrity are found, the better clinical decision would be no intervention and systematic prevention’. Furthermore, the practitioner should be aware that the presence and thickness of an adhesive layer beneath the composite can lead to a misdiagnosis of the radiolucent area, which can negatively influence the decision to replace the restoration.4
While there is a correlation between the presence of defective margins in restorations and recurrent caries, it should be borne in mind that there will also be many such teeth that will not have evidence of recurrent caries. Kidd et al5 examined amalgam restorations and found that plaque samples from margins with ditches greater than 0.4 mm harboured significantly more bacteria (mutans streptococci and lactobacilli) than did clinically intact margins and margins with narrow ditches. Another study6 examined the prediction of secondary caries around tooth-coloured restorations. Grading the margins as either intact, having a narrow ditch, or having a wide ditch, it was found that less than 25% sites without frankly carious cavities had soft dentine at the EDJ and that none of the clinical criteria chosen would reliably predict the presence of this soft dentine. This further strengthens the view that the radiolucencies are less likely to be carious dentine. A visual inspection as well as radiographic examination will help the practitioner in arriving at a ‘best guess’ as to what is happening but will also pose diagnostic and treatment challenges.7–9
A radiopaque resin would certainly help reduce the uncertainty. With the introduction by 3M of Scotchbond Universal Plus, the radiopaque resin helps clinicians avoid any doubt regarding whether a radiolucent layer at the base of a posterior composite restoration is a pool of (non-radiopaque) resin or residual/secondary caries.10
The following should be considered when deciding on the management of such presentations.
Symptoms;
Reproducibility of the radiograph over time, ensuring angulation and exposure are consistent;
Inter-examiner variation is high;
Intra-examiner variation is high;
Consistency of assessment and decision making is not as good as we would like to think;
Radiographs do not indicate carious activity;
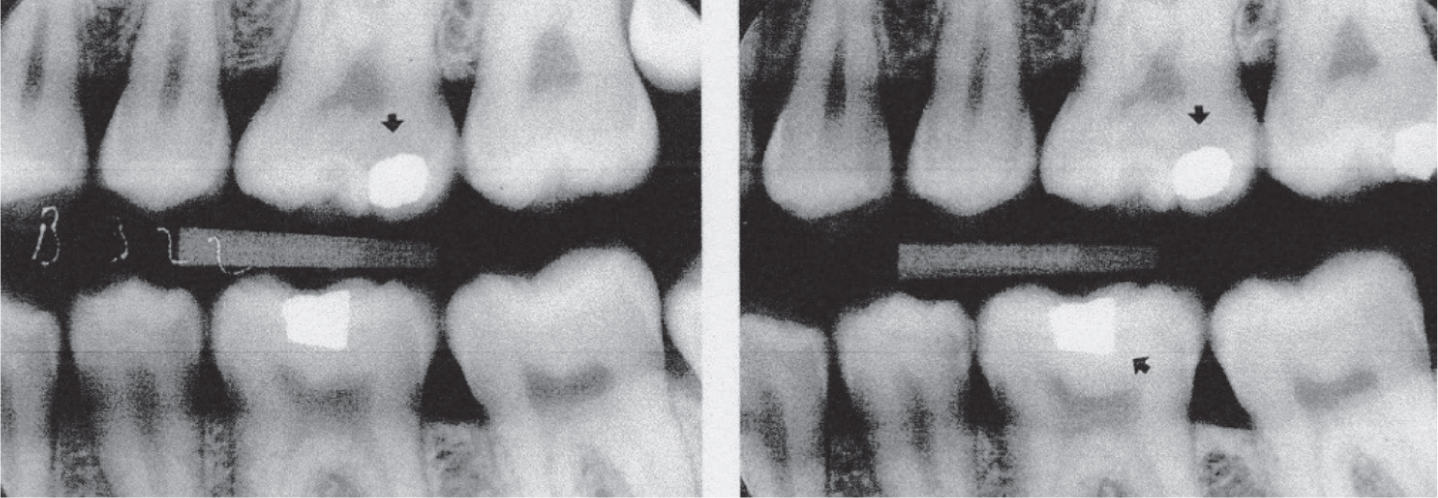
Recurrent caries is most frequently situated cervically to approximal restorations (Figure 3);
Integrity of a restoration's margin;
Repair/replacement of a restoration: what are the risks and/or benefits?
Easier to detect radiolucencies/opacities against metal restorations than composite;
Presence of radiolucent lining/bond.
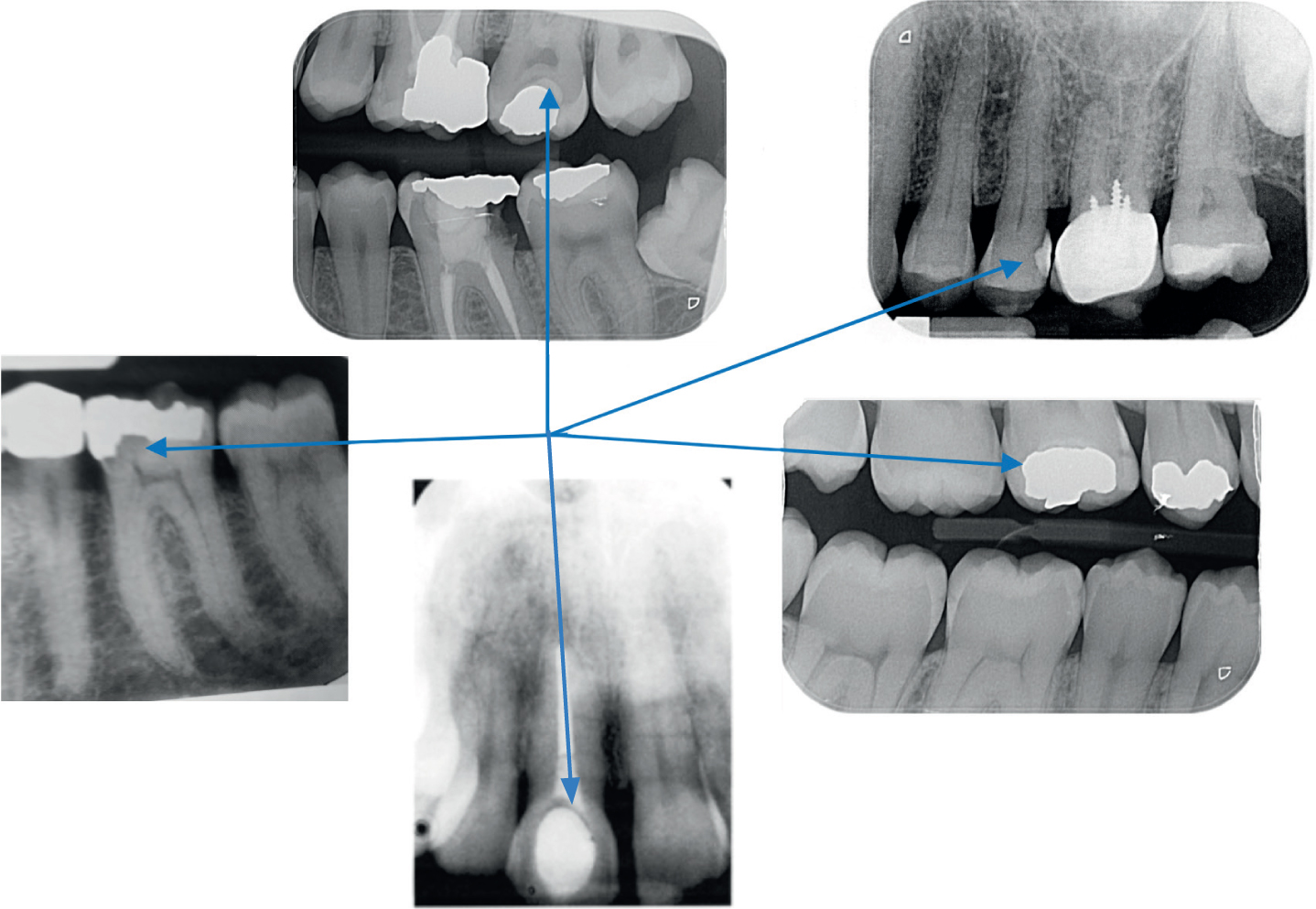
Figure 1. Examples of voids and opacities beneath restorations.Figure 2. 6 years follow up showing no change in progression of radiolucency at UL6. Note the size of the pulp chamber of UL6 in both radiographs: there has been no apparent change.Figure 3. Recurrent caries at the distolingual margin of the amalgam restoration.
Conclusion
Radiopacities and radiolucencies beneath restorations provide the dental practitioner with diagnostic challenges as to the nature of such findings. Understanding the possible aetiologies of these radiographic appearances is essential for their subsequent management to avoid unnecessary intervention.
It is essential to make detailed records of observations and decisions about the management of radiolucent and radiopaque areas so that subsequent reviews will have a base line to which to refer.
In the song ‘Fools rush in’, written in 1940 by Johnny Mercer and Rube Bloom,11 there are lyrics that resonate with the challenges presented to the practitioner by radiolucencies and radiopacities beneath restorations seen on radiographs:
‘Fools rush in where angels fear to tread And so I come to you, my love, my heart above my head.
Though I see the danger there. If there's a chance for me, then I don't care’.
Fool or angel? Heart or head? It's good to have a choice, but whatever decision is made about the management of such areas, it is essential to be aware of whose interests are being served by the decision. It must, first and foremost, be in the best interests of the patient.