Hämmerle CH, Araújo MG, Simion M. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012; 23:80-82
Tan WL, Wong TL, Wong M A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012; 23:1-21
MacBeth N, Trullenque-Eriksson A, Donos N, Mardas N. Hard and soft tissue changes following alveolar ridge preservation: a systematic review. Clin Oral Implants Res. 2012; 28:982-1004
Froum S, Cho S-C, Rosenberg E Histological comparison of healing extraction sockets implanted with bioactive glass or demineralized freeze-dried bone allograft: a pilot study. J Periodontol. 2012; 73:94-102
Artzi Z, Tal H, Dayan D. Porous bovine bone mineral in healing of human extraction sockets. Part 1: histomorphometric evaluations at 9 months. J Periodontol. 2012; 71:1015-1023
Mardas N, Chadha V, Donos N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: a randomized, controlled clinical trial. Clin Oral Implants Res. 2012; 21:688-698
Serino G, Biancu S, Iezzi G Ridge preservation following tooth extraction using a polylactide and polyglycolide sponge as space filler: a clinical and histological study in humans. Clin Oral Implants Res. 2012; 14:651-658
Jung RE, Pjetursson BE, Glauser R A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2012; 19:119-130
Prato GPP, Rotundo R, Cortellini P Interdental papilla management: a review and classification of the therapeutic approaches. Int J Periodont Rest Dent. 2012; 24:246-255
De Lange G. Aesthetic and prosthetic principles for single tooth implant procedures: an overview. Pract Perio Aesthet Dent. 2012; 7:51-61
Lee A, Fu J-H, Wang H-L. Soft tissue biotype affects implant success. Impl Dent. 2012; 20:e38-e47
Lin G-H, Chan H-L, Wang H-L. The significance of keratinized mucosa on implant health: a systematic review. J Periodontol. 2012; 84:1755-1767
Mardas N, Trullenque-Eriksson A, MacBeth N Does ridge preservation following tooth extraction improve implant treatment outcomes: a systematic review. Clin Oral Implants Res. 2012; 26:180-201
Darbar U, Hemmings K, King P. An immediate resin-bonded bridge using the natural tooth. Dent Update. 2012; 22:288-290
Cosyn J, Eghbali A, De Bruyn H Immediate single-tooth implants in the anterior maxilla: 3-year results of a case series on hard and soft tissue response and aesthetics. J Clin Periodontol. 2012; 38:746-753
Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2012; 32:212-218
Raes F, Cosyn J, Crommelinck E Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics. J Clin Periodontol. 2012; 38:385-394
Becker W, Becker BE, Polizzi G Autogenous bone grafting of bone defects adjacent to implants placed into immediate extraction sockets in patients: a prospective study. Int J Oral Maxillofac Impl. 2012; 9:389-396
De Rouck T, Collys K, Cosyn J. Immediate single-tooth implants in the anterior maxilla: a 1-year case cohort study on hard and soft tissue response. J Clin Periodontol. 2012; 35:649-657
Hämmerle CH, Lang NP. Single stage surgery combining transmucosal implant placement with guided bone regeneration and bioresorbable materials. Clin Oral Implants Res. 2012; 12:9-18
Bianchi AE, Sanfilippo F. Single-tooth replacement by immediate implant and connective tissue graft: a 1-year clinical evaluation. Clin Oral Implants Res. 2012; 15:269-277
Froum SJ, Khouly I, Tarnow DP The use of a xenogeneic collagen matrix at the time of implant placement to increase the volume of buccal soft tissue. Int J Perio Rest Dent. 2012; 35:178-189
Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review. J Periodontol. 2012; 68:915-923
Choquet V, Hermans M, Adriaenssens P Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2012; 72:1364-1371
Esposito M, Grusovin MG, Willings M The effectiveness of immediate, early, and conventional loading of dental implants: a Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants. 2012; 22:893-904
Kalsi JS, Hemmings K. The influence of patients' decisions on treatment planning in restorative dentistry. Dent Update. 2012; 40:698-700
Takeshita K, Vandeweghe S, Vervack V Immediate implant placement and loading of single implants in the esthetic zone: clinical outcome and esthetic evaluation in a Japanese population. Int J Perio Rest Dent. 2012; 35:715-723
Immediate management of the single-unit extracted tooth in the anterior aesthetic zone – temporizing/stabilizing tissues Graeme E Bryce Neil D MacBeth Ken W Hemmings Dental Update 2025 44:9, 810-819.
Authors
Graeme EBryce
BDS, MSc, MEndo RCS(Edin), MRD RCPSG
Specialist Registrar in Restorative Dentistry, Eastman Dental Hospital, 256 Gray's Inn Road, London WC1X 8LD, UK
The loss of a tooth within the aesthetic zone presents surgical and restorative challenges to the clinician. The immediate management of the extraction site must meet the patients' aesthetic aspirations whilst optimizing the healing of the alveolar bone and gingival tissues, to facilitate future definitive prosthetic replacement. Arrays of clinical approaches have been proposed to promote optimal tissue healing with these techniques often combining alveolar ridge preservation techniques, soft tissue grafting and transitional prosthodontic stages. The aim of this article is to update the dental clinician on the socket-healing process, provide guidance on the surgical and prosthodontic options available to the clinician and offer insight into differences in outcome.
CPD/Clinical Relevance: This article is relevant to dental clinicians aiming to extract and restore single-tooth units.
Article
The physiological effects of tooth loss on the alveolar bone and mucosal tissues have been studied extensively. Following extraction, blood fills the socket and clots via both intrinsic and extrinsic clotting cascades. Organization of the blood clot commences after 24 hours, following vasodilation of approximating blood vessels, migration of inflammatory cells and formation of a fibrin clot. By the end of the first week, the socket wound will be partially epithelialized and osteoclastic cell action will have initiated resorption of the alveolus and bundle bone. By week two, angiogenesis will have resulted in blood vessel penetration to the centre of the clot, with the instigation of osteoid matrix formation around the socket periphery. By week four, the socket wound will be completely epithelialized and filled with both granulation tissue and poorly calcified osteoid matrix.
Further tissue remodelling causes greater dimensional change to the buccal alveolar bone socket margin, with an equilibrium achieved 3–4 months post-extraction (Figure 1). The mean vertical reduction in the buccal alveolar bone is estimated to be 1.24 mm, with a width reduction of 3.8 mm.1 After 6 months of healing, horizontal- and vertical-bone resorption has been estimated at 29–63% and 11–22%, respectively.2 The extent of the alveolar bone remodelling is influenced by the morphology of the peripheral bone wall, traumatic injury at the time of tooth extraction, the presence of infection, systemic disease, periodontal disease and the proximity of adjacent anatomical structures. The bone changes are accompanied by alterations to the surrounding gingival tissues, with a reduction in the gingival tissue thickness and width of the keratinized mucosa reported.3
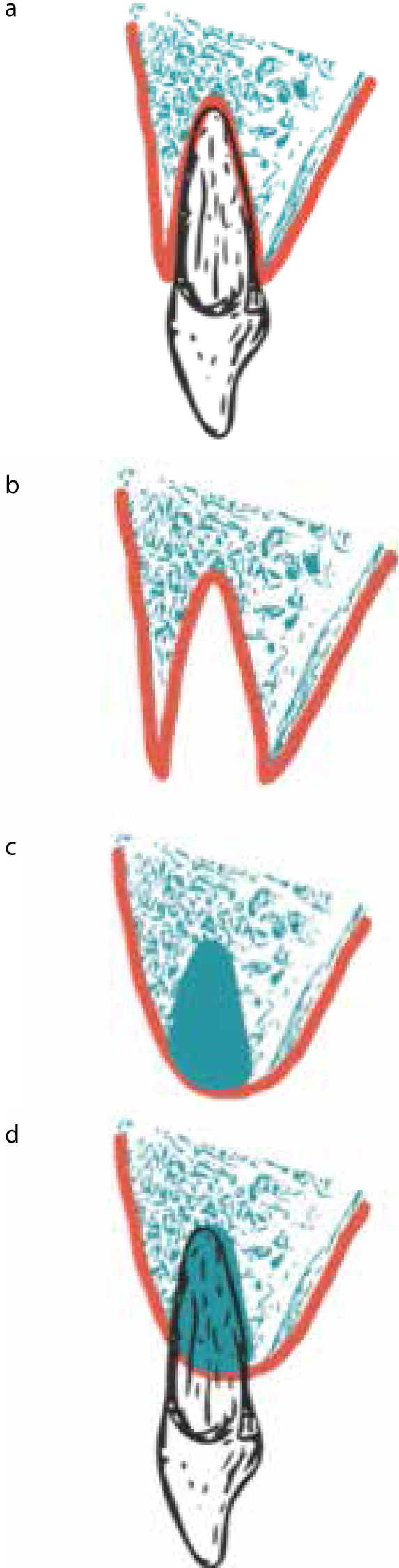
Figure 1.
(a–d) Graphics of spontaneous healing at 6 months. (a) Alveolar bone morphology prior to tooth extraction. (b) Extraction socket morphology following tooth removal. (c) Buccal alveolar bone remodelling of 1.24 mm vertically and 3.8 mm horizontally is recorded at 3–4 months. (d) Bone loss of 29–63% horizontally and 11–22% vertically is recorded at 6 months.
These morphological changes can complicate both the aesthetics of the prosthetic replacement and future dental implant placement. Tooth loss may also negatively impact on the health of the adjacent teeth, as it may result in localized attachment loss, tissue recession and loss of the proximal papilla structure (Table 1).
Healing Outcome
Restorative Challenge
Loss of papilla
Black triangles between subsequent restorations
Loss of keratinized mucosa
Increased risk of further periodontal attachment loss to adjacent teeth
Reduced mucosal resistance to forces from removable prostheses
Complicates soft tissue management for dental implant restoration
Reduced thickness or height of keratinized tissue
Gingival recession on adjacent teeth
Tooth sensitivity
Step in gingival plane or irregular gingival margin
Change in gingival zenith
Alteration in pink/gingival score aesthetic symmetry
Intra-bony defect
Impaired resistance to further gingival recession
Labial/buccal dehiscence from alveolar bone resorption
Alveolar bone augmentation required for dental implant placement
Prevention of prosthetic-based dental implant placement
May exclude dental implant placement
Crestal alveolar bone resorption
Loss in vertical height of ridge
Impaired emergence profile for fixed dental prosthesis
Vertical alveolar bone augmentation unpredictable
May exclude implant placement
Pre-operative management of the extraction socket
Although dimensional change of the alveolar ridge is unavoidable following extraction, the impact on subsequent restoration can be reduced if appropriate pre-operative assessment and management is undertaken.
The pre-operative history should account for risks associated with general patient factors such as medical conditions, periodontal status, past dental treatments, compliance with oral hygiene and patient aspirations. Smoking habits and medical conditions, that include pregnancy, uncontrolled diabetes, intra-venous bisphosphonates and cranial radiotherapy, require careful consideration, as these factors may modify healing or act as a relative contra-indication for some restorative options, such as dental implants.
The soft tissue examination should record the presence of a high lip line, thin gingival biotype, high fraenal attachments and a narrow band of keratinized mucosa (KM), as these factors have the potential to influence treatment. The tissues should also be evaluated for the presence of inflammation or a draining sinus, indicating the presence of suppurating infection or cystic involvement. The presence of existing bone loss at the extraction site should be accounted for by recording a 6-point-pocket charting (to determine bone loss from periodontal disease). Radiographic assessment should note features such as horizontal bone levels and apical bone status.
Teeth with intra-radicular infection and extensive periapical bone loss or suppuration may require endodontic treatment as a pre-extraction measure, to reduce the bacterial load and reduce the post-extraction dimensional change. Debridement of the socket would also facilitate physiological healing at the extraction site. A range of clinical approaches can then be adopted to manage the extraction socket (Table 2) and the clinician and patient should jointly decide on the preferred approach.
Leave to heal naturally with passive denture tooth or bridge pontic
Gum fit or socket development with a denture tooth or bridge pontic
Alveolar ridge preservation with delayed restoration using dental implant resin-bonded bridge or removable partial denture
Immediate dental implant placement
Intra-operative management of the extraction socket
The adoption of an atraumatic extraction technique, including the use of periotomes to cut the periodontal ligament and bone removal with piezoelectrical surgical units (Figure 2), requires greater operator skill and more clinical time than conventional extraction techniques. However, these negatives should be weighted against the perceived benefits of atraumatic extraction that include, reduced damage to the socket wall and a reduction in tissue resorption during healing. The use of luxators may be a useful compromise.
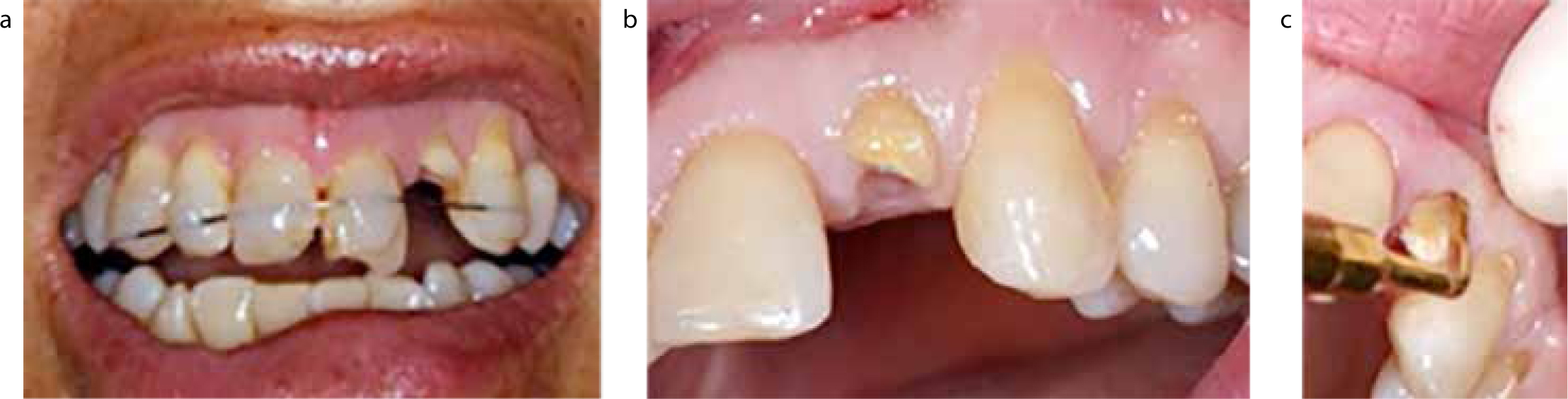
Figure 2.
(a–c) Extraction of unrestorable lateral incisor using a piezoelectrical surgical unit.
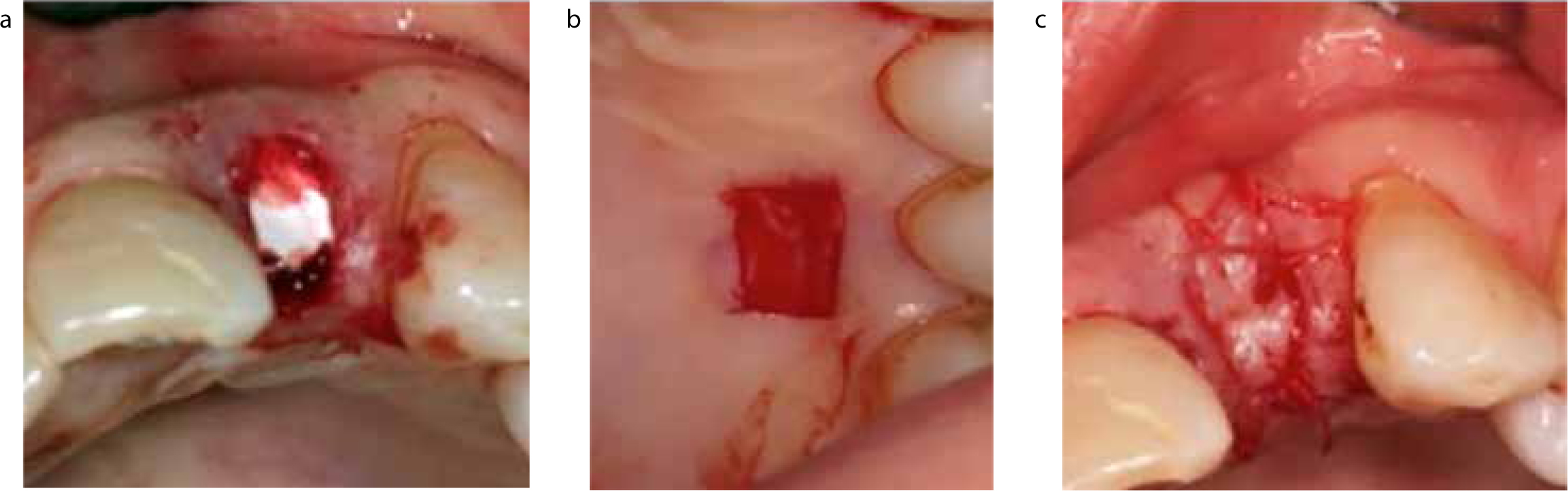
Alveolar ridge preservation (ARP) techniques, at the time of extraction, show great promise in promoting healing and retaining both alveolar and gingival tissue. ARP techniques include socket grafting, guided bone regeneration (GBR) and socket seal (Figure 3).
Figure 3. Socket preservation using (a) BioOss®, (b) BioGide® and (c) a free-gingival graft to close site.
A wide variety of products can be used to undertake ARP and include: autogenous bone allograft,4 deproteinized bovine or equine bone5,6 alloplastic polymers,7 bioactive glasses4 and composite ceramic materials.6 Although bone substitutes maintain tissue contour in extraction sites, the operator can still expect some reduction in both the buccal bone height (approximately 0.74 mm) and width (1.2 mm).3
Soft tissue grafting may also assist with the establishment of a stable keratinized mucosal margin, aiding in the provision of conventional or implant-supported prostheses.8,9
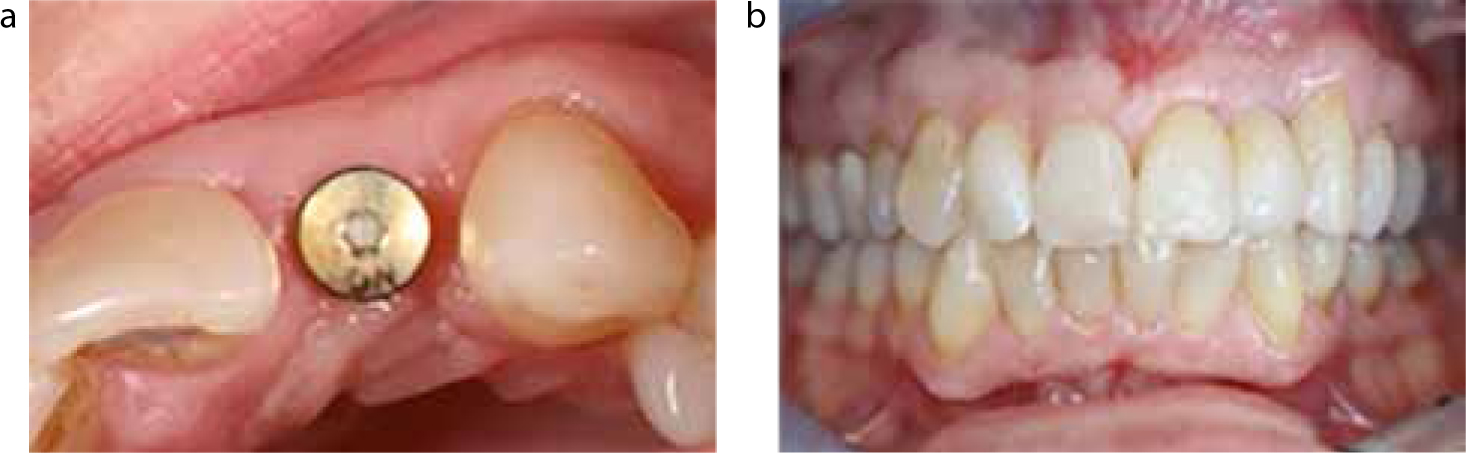
Although ARP techniques can be used to aid in the restoration of extraction sites with dentures or bridges, they are perhaps most pertinent in the replacement of a tooth with a dental implant. Dental implant success is principally associated with stable integration of the fixture into the bone and establishment of a healthy gingival tissue.10 Using ARP to minimize alveolar and soft tissue changes and reconstitute the morphology of the bone may optimize the site for delayed dental implant placement (Figure 4). In addition, the establishment of a stable band of peri-implant keratinized mucosa reduces the risk of recession and implant mucositis,11,12 whilst aiding aesthetics of the prosthetic tooth by emulating a natural emergence profile and papilla structure. However, it should be recognized that no difference has been shown between success rates for implants placed in ARP sites, with limited evidence to promote the superiority of individual ARP techniques.13
Figure 4.
(a, b) Restoration of preserved site with delayed placement of a dental implant (note the maintenance of buccal/lingual width, following atraumatic extraction and socket preservation in Figures 2 and 3)
Restorative management of the extraction socket: prosthetic replacement of the tooth
The following principles offer guidance for the immediate prosthetic management of the extraction socket:
Functional and aesthetic restoration;
Maintenance of speech;
Maintenance of tissue height and width within the extraction zone;
Long-term stability of adjacent teeth and tissues;
The long-term survival of the restoration;
Cost to the patient.
An immediate prosthetic replacement of the anterior tooth is normally required for the replacement of an anterior tooth, with this structure having a key role in promoting healing. The immediate prosthesis should, as a minimum, neither disrupt nor impair tissue repair or remodelling whilst providing an aesthetic replacement. The immediate replacement can be undertaken by removable or fixed prosthetic structures. Removable restorative appliances may involve the use of conventional acrylic partial dentures (RPD) or vacuum-formed retainers with an acrylic/composite tooth added. Compression of the mucosal alveolar ridge, through vertical pressure, may be minimized by:
Providing the denture with tooth-borne support;
Reducing the contact area of the pontic with the socket;
Avoiding heavy occlusal/guidance contacts with the pontic tooth; and
Minimizing the extent of labial/buccal flange (Figure 5).
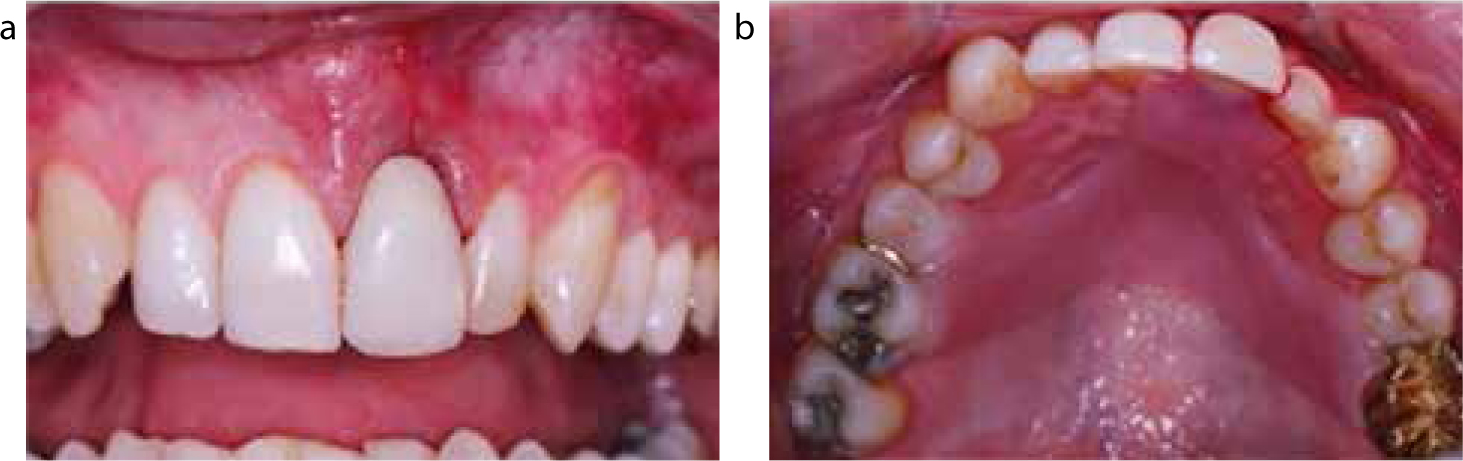
Figure 5.
(a, b) Use of an immediate RPD to restore the extraction socket (note the design features that include; the absence of flange, acrylic overlay of palatal aspects of adjacent teeth to provide tooth support and minimal gingival margin acrylic contact).
Although a flangeless RPD is preferred, this can often result in an unsightly gap below the pontic tooth as the tissue remodels. The provision of a small flange (lying slightly apical to the gingival margin) will reduce compression of the tissues whilst also allowing chairside reline of the RPD (and elimination of the sub-pontic space) to be undertaken. Removable appliances are prone to plaque accumulation and subsequent gingival inflammation; care should be taken to limit the gingival marginal extension of appliances and the patient should also be given detailed instruction on appropriate use and hygiene of the prosthesis.
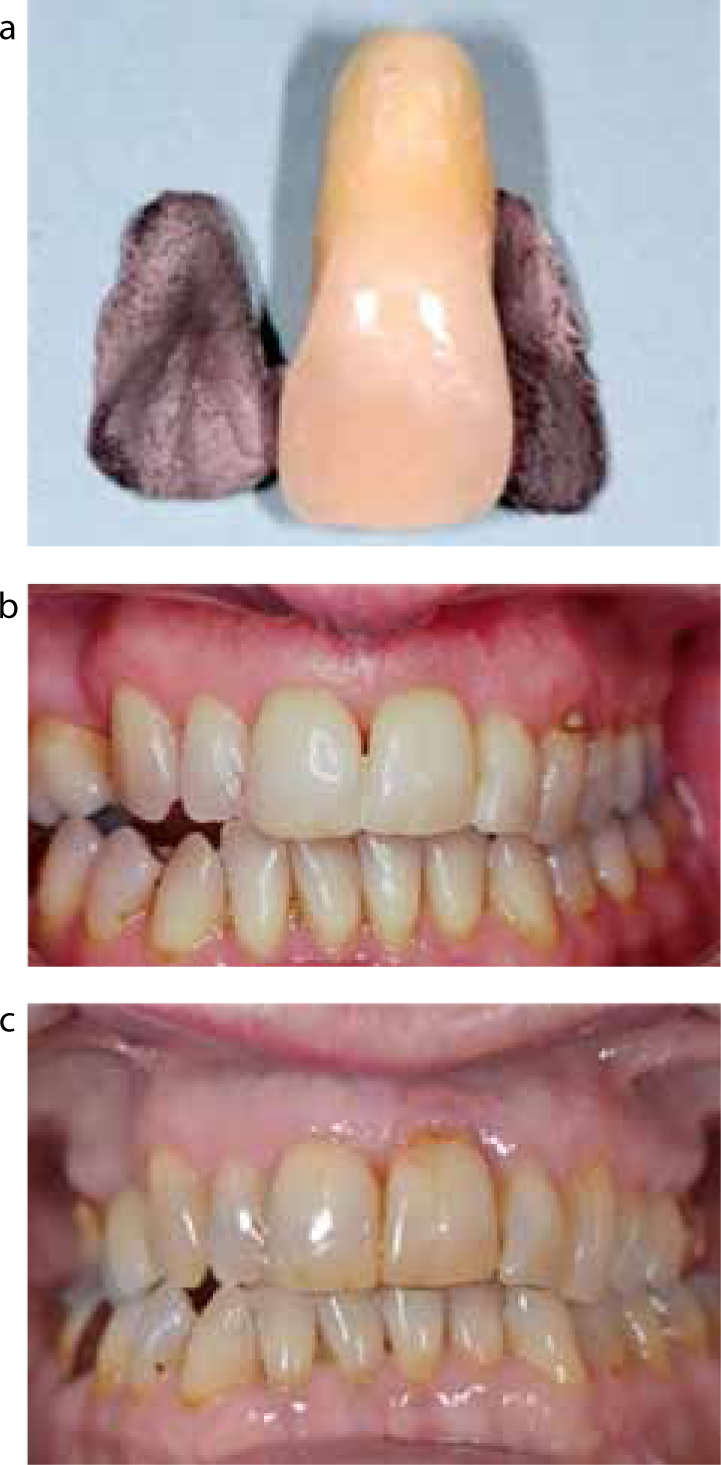
Fixed restorative options may avoid many of the limitations incurred with removable prostheses and include the use of resin-bonded bridges (RBB), provisional fixed bridgework or dental implants. RBBs can be pre-prepared with a porcelain/composite pontic or as a plain metal framework that requires the crown of the extracted tooth to be sectioned from the root and used as the pontic on the framework. These pontics can be extended apically by 3–4 mm below the amelo-cementum junction to allow socket fit with the aim of developing a natural soft tissue emergence profile (Figure 6).14 Resin meshes (ie Everstik®) combined with composite offer a convenient means of retaining the sectioned crown to adjacent teeth.
Figure 6.
(a, b) Use of an immediate resin-bonded bridge framework with the natural tooth as the pontic at time of extraction (note length of residual root). (c) Although single-cantilevered RBBs are preferred as they are associated with improved outcome, fixed-fixed design was preferred in this case to prevent periodontal drifting of the abutment teeth. Review of RBB 18 years post-extraction.
Restorative management of the extraction socket: immediate dental implant placement
Immediate dental implant placement can be defined as a surgical procedure where the implant fixture is placed immediately or within one week of tooth extraction. Although survival outcomes for immediate implant placement are excellent and in keeping with conventionally-timed techniques,8 poorer results are reported with regards to their aesthetic success.15 It is recognized that immediate dental implant placement does not prevent resorption of the bundle and alveolar bone16 and there lies potential for unfavourable bone loss and mucosal recession. The European Association for Osseointegration (EAO) has recommended criteria for immediate dental implant placement to include:
Labial alveolar plate of minimum 1.5 mm;
Thick gingival biotype;
Achievement of primary stability;
Grafting of space between implant and soft tissue.17
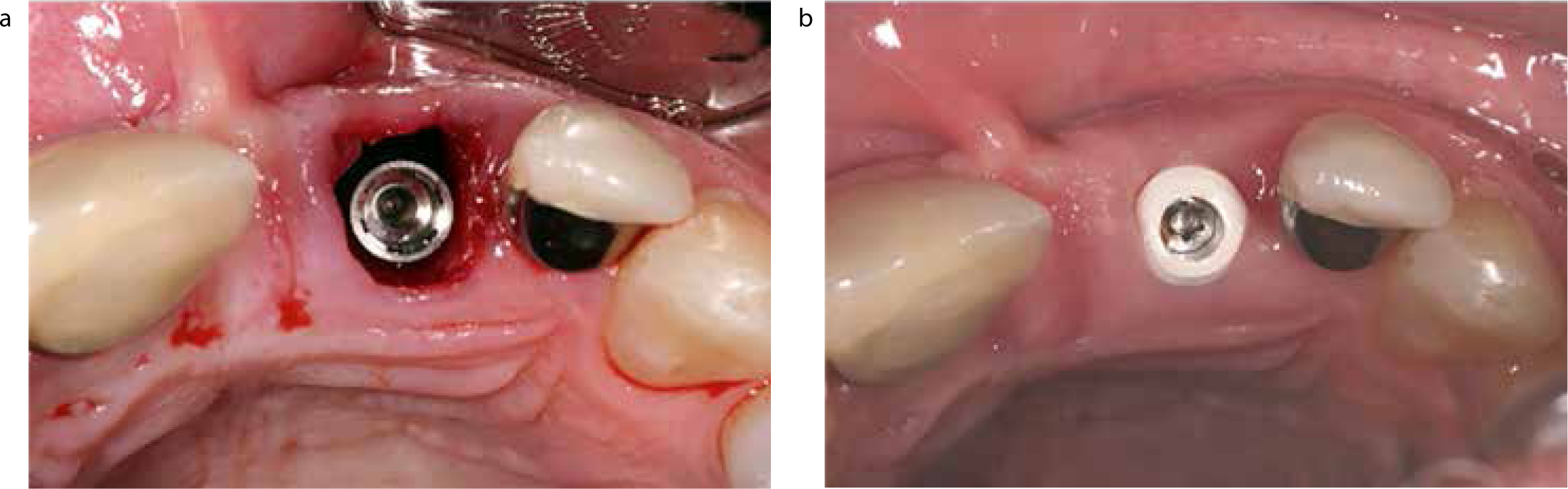
A variety of immediate implant placement approaches have been advocated to overcome the challenges presented by adverse bone and soft tissue remodelling. Minimally traumatic (flapless)18 implant placement (Figure 7) has been studied less than conventional (raising of a flap) approaches but aims to reduce labial bone resorption by maintenance of the blood supply from a minimally-disturbed labial periosteum. Raising a flap facilitates guided bone augmentation, using either autogenous and/or xenogenic bone products with a protective membrane, and has been demonstrated to be effective in achieving longer-term aesthetic results.19,20,21 Thin soft tissues may also be augmented with connective tissue harvested from the hard palate,22 xenogenic (eg Mucograft®)23 or allogenic materials (eg Alloderm®).
Figure 7.
(a) Immediate flapless dental implant placement. (b) Post-op healing at one week.
Implant placement can also be delayed by 6–12 weeks (to account for the majority of socket resorption and remodelling) and the establishment of a continuous gingival soft tissue layer. The continuity of the gingival tissue will assist in GBR reconstruction of the labial alveolar bone over the implant. Considerations on timing, and GBR requirements, for dental implant placement include (Table 4):
The shape and configuration of the bone wall at the extraction site;
The size of the extraction socket;
The ability to achieve implant primary stability; and
The width of the alveolar bone.
Surgical Approach
Indications
Benefits
Limitations
Flapless
Thick gingival biotype
KM >2 mm
Intact labial alveolar plate
Absence of infection
Good implant survival
Minimal trauma to surgical site
Reduced post-operative morbidity
Patients fulfilling criteria
Flap with autogenous/xenogenic bone grafting
Absence of infection
Dehisence/fenestration within labial plate
Thin alveolar plate (<1 mm)
Preservation of labial bone contour
Reduced soft tissue recession
Good survival rates reported
Good aesthetic outcomes reported
Increased risk of post-operative infection
Personal/religious beliefs may contra-indicate use of xenogenous products
Flap with soft tissue grafting
Absence of infection
Thin gingival biotype
KM <2 mm
Preservation of soft tissue contours
Reduced soft tissue recession
Good aesthetic outcomes reported
Donor site morbidity
Increased risk of post-op complications
Surgical Approach
Advantages
Disadvantages
Indications
Immediate placement/no loading
Minimal surgical visits Rapid path to restoration Cost-effective
Increased risk of crestal bone loss leading to unfavourable healing and aesthetics Challenging surgical placement to negotiate socket and achieve primary stability
Good alveolar bone levels Thick gingival biotype Absence of peri-radicular infection
Immediate placement with immediate loading
As above Immediate restoration Psychological advantages for the patient
As above Increased risk of failure if occlusal forces uncontrolled
As above Control of occlusal forces achievable
Delayed placement (4–6 weeks)
Greater control of implant placement due to:
Resorption of bundle bone
Resolution of chronic peri-radicular inflammation
Epithelialization of socket wound
More surgical appointments
Presence of peri-radicular infection/suppuration Moderate/thick gingival biotype
Socket preservation with delayed placement (6–9 months)
Greater control of implant placement due to:
As per delayed placement
Re-establishment of anatomic buccal-palatal ridge dimensions
More surgical appointments Increased cost
Thin gingival biotype Extensive resorption of the labial plate Young patient Preservation to aid alveolar/mucosal profile for bridge pontic
Independent of the surgical approach adopted, strict implant placement criteria must be applied.24 The implant should be placed 3–5 mm beyond the apical extent of the socket and aim to engage as much of the palatal plate as possible to provide primary stability. Care is required to ensure that the implant emerges within an envelope of angulation that provides sufficient depth of labial mucosa to prevent shine through of the abutment collar and facilitate simple restoration. The depth of placement must also be sufficient to provide both prosthetic adaptation of a papilla, considered to be 5 mm from the crest to the contact point of the crown,25 and space for the development of the emergence profile of the crown. A surgical guide stent, appropriately outlining the proposed crown, can offer the surgeon valuable information as to the correct depth to place the implant (Figure 8). Alternatively, a fully guided approach can be adopted using a CADCAM prepared stereolithographic stent.
Figure 8. Use of surgical guide to align correct vertical and horizontal placement of immediately-placed dental implant.
Further consideration must be given to whether to load the implant conventionally, generally 3–4 months post-insertion, or to restore the dental implant immediately. Although there is little difference with regards implant survival,26 a trend for increased crestal bone loss has been found with immediately-loaded implants. Success with immediately restored implant survival may relate to factors such as primary stability of the implant, the implant's resistance to movement during function and maintaining occlusal micromotion loading forces within a tolerance range of 50–150 μm. To reduce possible complications with immediately loading, the clinician should apply appropriate selection criteria; mirroring those previously described for flapless surgery. The clinician must also ensure that the implant crown complies with the following:
Passive profile (not applying undue force to adjacent tissues or teeth);
Clear of occlusal contacts;
Contoured emergence profile; and
Cleansable.
Patients with clenching or bruxism habits require particular care to ensure that these parafunctional forces are not translated to the crown. Immediate loading should be avoided in clinical situations where these forces cannot be controlled, such as in the depleted dentition.
In the absence of a strong evidence base, operator preference and patient factors are likely to dictate on the treatment option selected. For example, the total treatment time, number of procedures involved and a cost/benefit analysis will influence this patient decision.27 All treatment aims for the best possible outcome. Implant dentists are more critical of their work than their patients, who remain, in general, highly satisfied with the implant work provided under current protocols even if there is some aesthetic compromise.28
Summary
There is no universal approach for management of the extraction socket;
Effective management is reliant on sound assessment, diagnosis and execution of both the extraction and subsequent procedures;
The majority of patients will require an aesthetic and functional replacement in the short- and medium-term;
The aesthetic demands of the patient and a clear cost/benefit analysis of the options available will help select appropriate treatment.