Duncan HF, Galler KM European Society of Endodontology position statement: management of deep caries and the exposed pulp. Int Endod J. 2019; 52:923-934 https://doi.org/10.1111/iej.13080
Mathur VP, Dhillon JK, Logani A, Kalra G Evaluation of indirect pulp capping using three different materials: a randomized control trial using cone-beam computed tomography. Indian J Dent Res. 2016; 27:623-629 https://doi.org/10.4103/0970-9290.199588
Lipski M, Nowicka A, Kot K Factors affecting the outcomes of direct pulp capping using Biodentine. Clin Oral Investig. 2018; 22:2021-2029 https://doi.org/10.1007/s00784-017-2296-7
Sabeti M, Huang Y, Chung YJ, Azarpazhooh A Prognosis of vital pulp therapy on permanent dentition: a systematic review and meta-analysis of randomized controlled trials. J Endod. 2021; 47:1683-1695 https://doi.org/10.1016/j.joen.2021.08.008
Careddu R, Duncan HF A prospective clinical study investigating the effectiveness of partial pulpotomy after relating pre-operative symptoms to a new and established classification of pulpitis. Int Endod J. 2021; 54:2156-2172 https://doi.org/10.1111/iej.13629
Taha NA, Abuzaid AM, Khader YS A randomized controlled clinical trial of pulpotomy versus root canal therapy in mature teeth with irreversible pulpitis: outcome, quality of life, and patients' satisfaction. J Endod. 2023; 49:624-631.e2 https://doi.org/10.1016/j.joen.2023.04.001
Consensus Conference on Diagnostic Terminology. J Endod. 2009; 35:(12)
Bjørndal L, Simon S, Tomson PL, Duncan HF Management of deep caries and the exposed pulp. Int Endod J. 2019; 52:949-973 https://doi.org/10.1111/iej.13128
Shahi P, Sood PB, Sharma A Comparative study of pulp vitality in primary and young permanent molars in human children with pulse oximeter and electric pulp tester. Int J Clin Pediatr Dent. 2015; 8:94-98 https://doi.org/10.5005/jp-journals-10005-1291
Ghouth N, Duggal MS, Kang J, Nazzal H A diagnostic accuracy study of laser doppler flowmetry for the assessment of pulpal status in children's permanent incisor teeth. J Endod. 2019; 45:543-548 https://doi.org/10.1016/j.joen.2019.01.017
Patro S, Meto A, Mohanty A Diagnostic accuracy of pulp vitality tests and pulp sensibility tests for assessing pulpal health in permanent teeth: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022; 19 https://doi.org/10.3390/ijerph19159599
Ricucci D, Siqueira JF, Li Y, Tay FR Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J Dent. 2019; 86:41-52 https://doi.org/10.1016/j.jdent.2019.05.022
Chua SKX, Sim YF, Wang WC One-year outcome of selective caries removal versus pulpotomy treatment of deep caries: a pilot randomized controlled trial. Int Endod J. 2023; 56:1459-1474 https://doi.org/10.1111/iej.13978
Maltz M, Garcia R, Jardim JJ Randomized trial of partial vs. stepwise caries removal: 3-year follow-up. J Dent Res. 2012; 91:1026-1031 https://doi.org/10.1177/0022034512460403
Davaie S, Hooshmand T, Ansarifard S Different types of bioceramics as dental pulp capping materials: a systematic review. Ceramics International. 2021; 47:20781-20792 https://doi.org/10.1016/J.CERAMINT.2021.04.193
Hashem DF, Foxton R, Manoharan A The physical characteristics of resin composite-calcium silicate interface as part of a layered/laminate adhesive restoration. Dent Mater. 2014; 30:343-349 https://doi.org/10.1016/j.dental.2013.12.010
Falacho RI, Melo EA, Marques JA Clinical in-situ evaluation of the effect of rubber dam isolation on bond strength to enamel. J Esthet Restor Dent. 2023; 35:48-55 https://doi.org/10.1111/jerd.12979
MDS, Senior Lecturer; Department of Conservative Dentistry and Endodontics Manipal College of Dental Sciences Mangalore, Affiliated to Manipal Academy of Higher Education, Karnataka, Manipal, India
Preserving pulp vitality is paramount in endodontics, necessitating a conservative and systematic approach. In the first case, a 48-year-old woman complained of pain on cold stimuli and food lodgement in the upper left posterior tooth region. Following thorough clinical and radiographic examination, the UL7 was diagnosed with reversible pulpitis and normal peri-apical tissues. Upon caries removal, pulp exposure occurred and was treated with direct pulp capping with Biodentine. A successful outcome was observed at 12-month follow-up. In the second case, a 26-year-old woman complained of food lodgement in a upper left posterior tooth region for 2 months. Subsequent clinical and radiographic examination confirmed deep caries in the UL4 with normal peri-apical tissues. Indirect pulp capping was performed, followed by 12-month follow-up.
CPD/Clinical Relevance: This case report underscores the management of deep caries, emphasizing the importance of following correct protocols, including isolation, use of bioceramic materials and adhering to proper bonding protocols to ensure maximum success.
Article
Vital pulp therapies have been gaining momentum since bioceramic materials were introduced, especially in the past decade. The main aim of carrying out vital pulp therapy is to ensure the pulp is healthy and reduce complications, such as tooth fractures resulting from root canal treatment.
Vital pulp therapy (VPT) procedures include indirect and direct pulp capping (DPC), as well as partial and full pulpotomy. DPC entails applying a biomaterial directly onto the exposed pulp, whereas indirect pulp capping (IPC) involves applying a biomaterial onto a thin dentine barrier in a one-stage carious tissue removal technique, typically onto hard dentine.1 The success rate of IPC stands at 96.6%, while that for DPC is at around 82.6%.2,3 A recent systematic review by Sabeti et al found that the overall success rate of VPT, using modern capping materials, such as mineral trioxide aggregate or calcium silicate-based materials, was 93.2%.4 Although the success of these treatment modalities depends on various factors, such as the pulp capping material, the operator's experience and technique, as well as the intensity and location of the insult, one of the major factors determining success is the true state of the pulp.
The closest approximation to the true state of pulp is obtained through a comprehensive patient history, thorough clinical and radiographic evaluations, and specialized diagnostic procedures.5 VPT technically can be attempted for any tooth with pulpitis that still contains some vital tissue.6,7 The appropriate form of VPT (i.e. pulp capping or pulpotomy) usually depends on the level of disease and how much vital tissue remains.
The following case reports detail the approach for accurate case selection followed by the use of calcium silicate material, proper isolation techniques and carrying out deep margin elevation (DME) and proper bonding strategies to ensure success.
Case report 1
A 48-year-old female patient presented to the clinic with a chief complaint of food lodgement persisting for the previous 5–6 months, and pain upon consuming cold food in the upper left back tooth region over the preceding month.
Upon clinical examination, the tooth of interest was identified as the UL7, exhibiting a Class II carious lesion according to GV Black's classification of dental caries (Figure 1). The tooth showed no tenderness upon palpation or percussion, and was non-mobile. The bite test was negative, ruling out any possibility of fracture. Periodontal examination revealed no bleeding upon probing and normal sulcus depth.
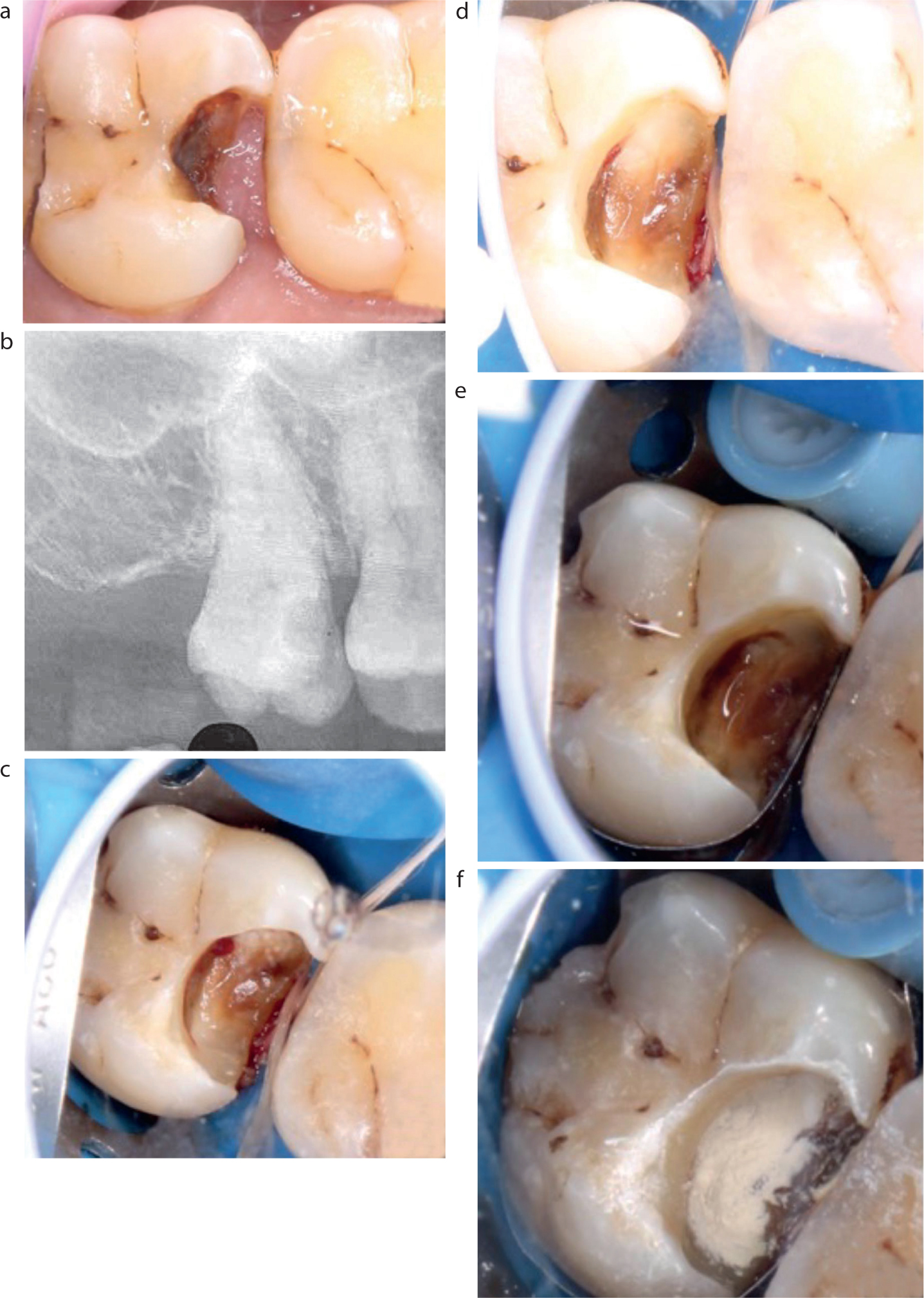
Figure 1. (a) Pre-operative image showing Class II caries. (b) Pre-operative intra-oral periapical radiograph. (c,d) Pulp exposure. (e) Pulpal haemostasis and soft caries excavation. (f) Biodentine application.
Pulp sensibility tests were performed, indicating a sharp, non-lingering response to the cold test (Endo-Frost, Coltene, Altstätten, Switzerland). A heat test (heated gutta-percha cone) and an electric pulp test yielded normal responses. Radiographic examination with respect to UL7 revealed a proximal coronal radiolucency involving enamel and dentine approximating the pulp, with no peri-apical changes observed (Figure 1).
The final diagnosis, following clinical and radiographic evaluation, was reversible pulpitis with normal periapical tissue concerning the UL7, as per diagnostic terminology recommended by the American Academy of Endodontics' consensus conference.8
After securing the patient's written consent and advising her about scheduled follow-up appointments, treatment was initiated. Local anaesthesia with epinephrine was administered, followed by gingival tissue management using a Thermacut bur (Dentsply Sirona, Charlotte, NC, USA) and rubber dam inversion was carried out for proper isolation. Soft caries was removed with a slow-speed round bur from the floor and periphery of the cavity, leading to pulpal exposure (Figure 1a–d). Pulpal bleeding was controlled using 2.5% sodium hypochlorite, followed by further excavation of soft caries (Figure 1e). Pulpal haemostasis was achieved within 3 minutes, and the decision was made to perform DPC.
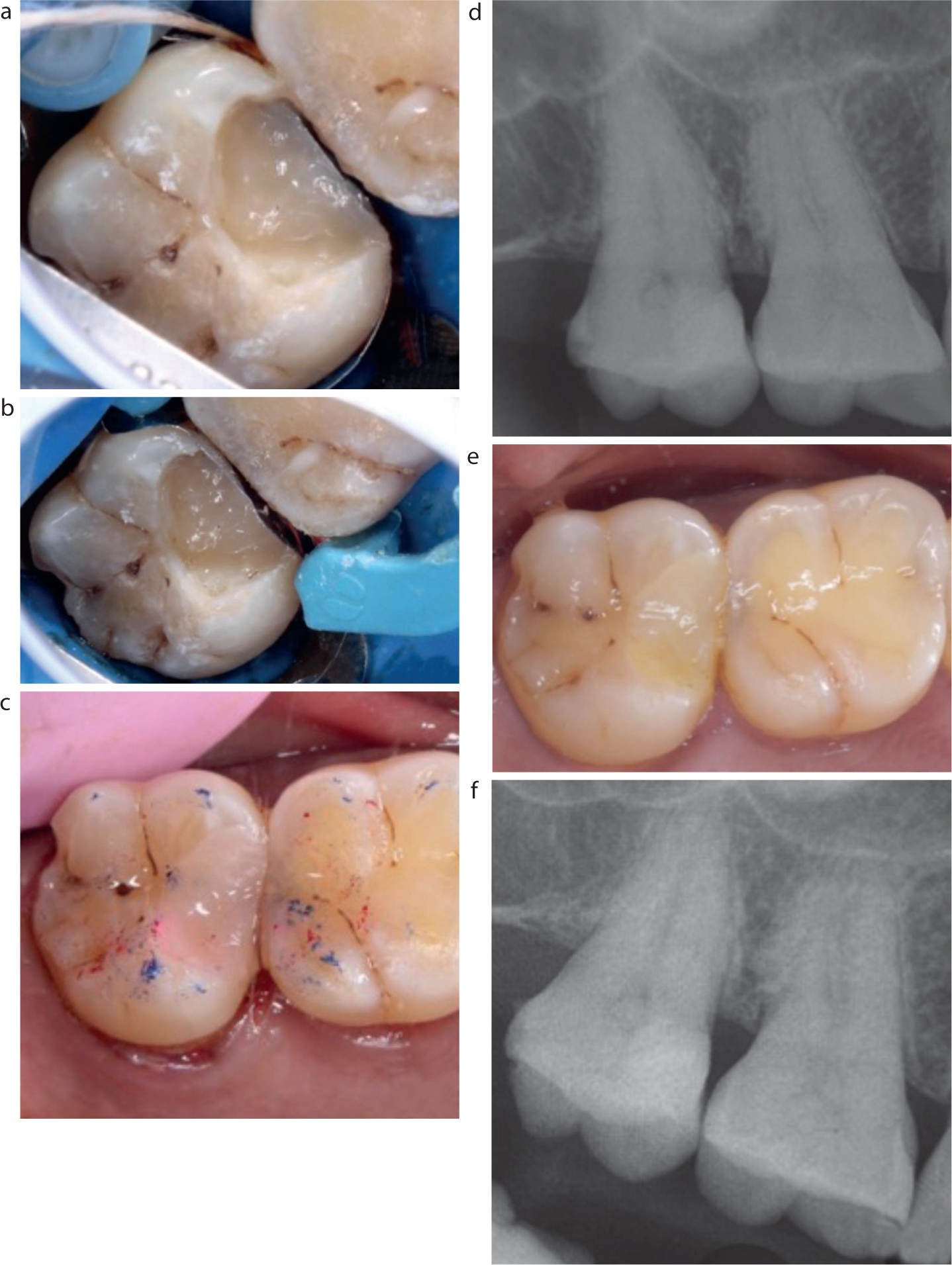
Biodentine (Septodont, Saint-Maur-des-Fossés, France), a bioceramic material composed of calcium silicate, was applied to the exposed pulp following manipulation according to the manufacturer's guidelines (Figure 1f). Subsequently, resin-modified glass ionomer cement (RMGIC) (Ionoseal, VOCO, Cuxhaven, Germany) was placed after a 12-minute waiting period. Since the mesial margin of the cavity was subgingival, DME was carried out using a DME-01 kit (Garrison Dental, Michigan, USA) (Figure 1). The cavity base was elevated using flowable composite (Filtek Supreme, 3M Espe, Seefeld, Germany), and the rest of the cavity was restored using a sectional matrix (Palodent V3 Intro Kit Sectional Matrix System, Dentsply, Charlotte, NC, USA) and composite (Filtek Z350 XT, 3M ESPE, Seefeld, Germany) (Figure 2).
After the composite restoration was finished and polished, a post-operative radiograph was taken, and the patient was scheduled for follow-up visits (Figure 2). The patient returned for 6-month and 1-year follow-up visits, during which time the tooth remained asymptomatic, showed a normal response to thermal testing, exhibited no tenderness upon percussion and displayed no peri-apical changes on radiographic examination (Figure 2).
Case report 2
A 26-year-old female patient reported to the clinic with a complaint of food lodgement in the upper left back tooth region for the previous 2 months. Additionally, she mentioned sensitivity to cold water consumption in that region. Upon clinical examination, UL4 showed Class II caries according to GV Black's classification, and there was no tenderness, mobility or discomfort upon palpation and percussion on the tooth of interest (Figure 3).
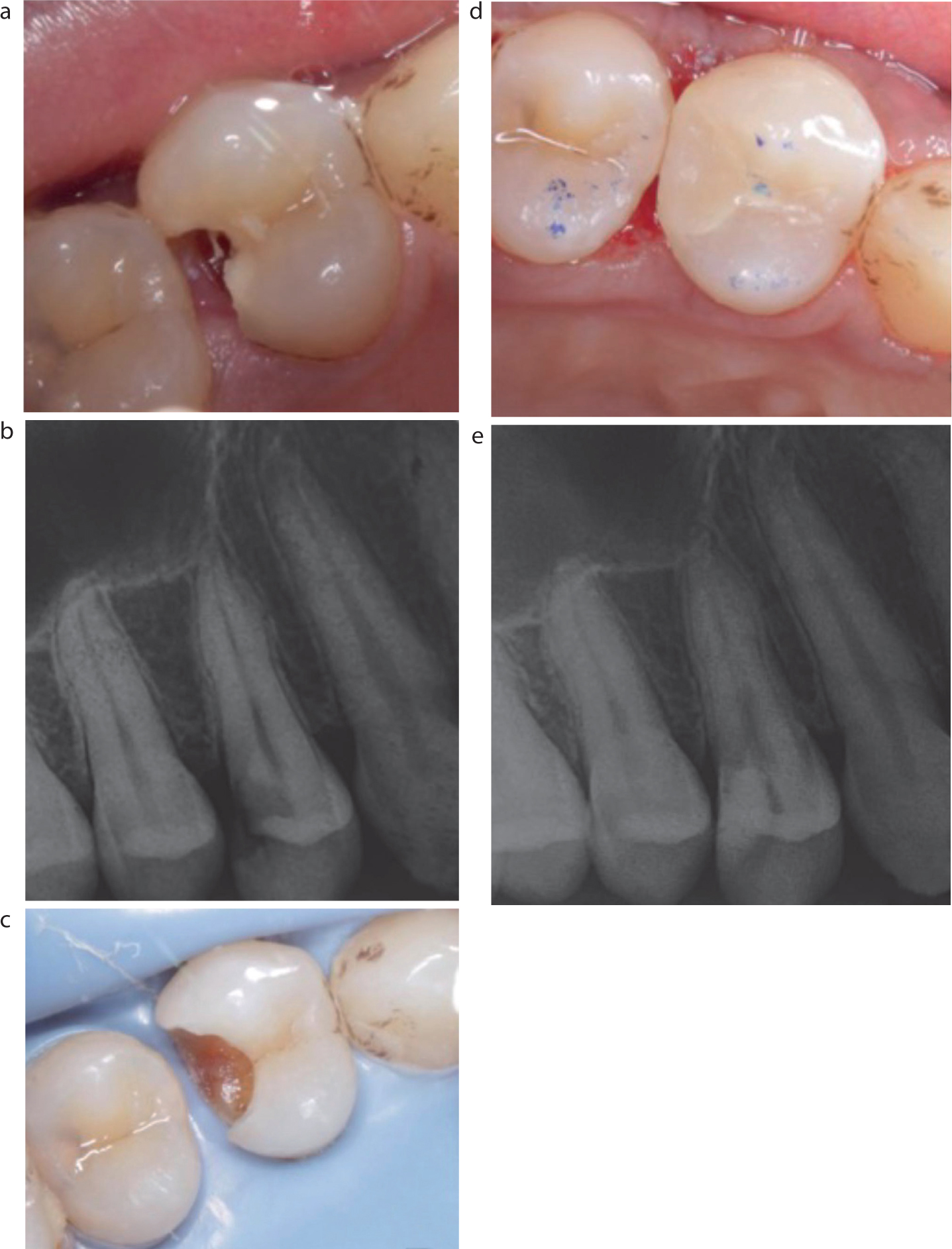
Figure 3. (a) Pre-operative image showing Class II cavity. (b) Pre-operative intra-oral peri-apical radiograph. (c) Removal of soft caries under rubber dam placement. (d) Biodentine applied and composite restoration placed. (e) Post operative intra-oral peri-apical radiograph.
Periodontal examination revealed normal sulcus depth. Pulp sensibility tests showed early responses to the cold test, and electric pulp and heat tests elicited normal responses. Radiographic examination confirmed the presence of radiolucency involving enamel and dentine and approximating the pulp of UL4, with normal peri-apical tissues (Figure 3). The final diagnosis, following clinical and radiographic evaluation, was reversible pulpitis with normal peri-apical tissue concerning the UL4.8
The tooth was anaesthetized using 2% lidocaine hydrochloride with epinephrine 1:80,000 then a rubber dam was placed for isolation (Figure 3). Careful manipulation of the dentine was performed using sterile round burs and a spoon excavator, ensuring removal until firm dentine remained on the pulpal floor and complete caries excavation was achieved from the cavity walls to facilitate optimal bonding. Following cavity disinfection with 2.5% sodium hypochlorite, freshly prepared Biodentine (Septodont) was applied on the cavity floor. After initial setting of Biodentine, RMGIC (Ionoseal) was placed. A saddle matrix was used to create contact on the distal margin of the cavity, and composite (Filtek Z350 XT) restoration was carried out. Finishing and polishing and occlusal adjustments were made on the restoration and a radiograph was taken (Figure 3).
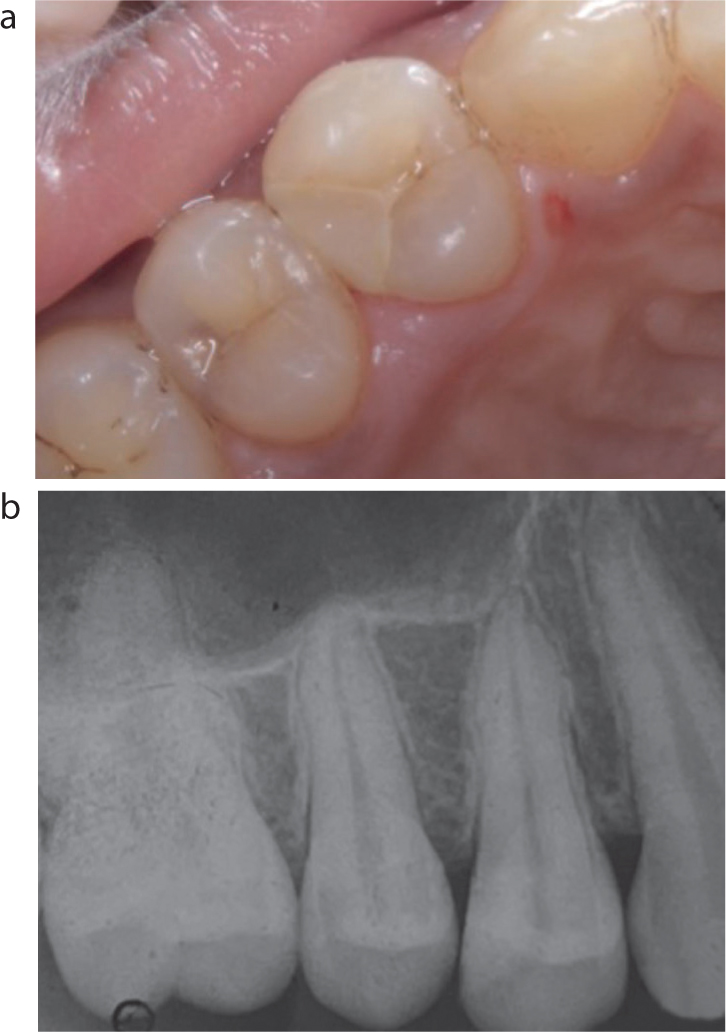
The patient was scheduled for follow-up visits at 6 months and 1 year. Although she did not attend the 6-month follow-up in the clinic, she reported no symptoms over the phone. At the 1-year follow-up, clinical and radiographic assessments were conducted, revealing normal responses to pulp testing and asymptomatic status of the tooth (Figure 4).
The aim of VPT includes the maintenance of vitality of the pulp as well as preservation of the remaining dental pulp for adequate structural/functional healing of the pulp-dentine complex.
Certain factors affect the success of VPT, which include the diagnosed state of the dental pulp, the removal technique for carious tissue, disinfection and bleeding control, the choice of material for pulp capping, economic factors and how pulp ‘friendly’ or not the patient is.9
To ascertain the state of the dental pulp, specialized tests such as pulp sensibility and pulp vitality tests have been used. Pulp sensibility tests such as heat, cold and electric tests assess the neural response of the pulp but they rely on a patient's reporting of the sensation. In contrast, pulp vitality tests, such as laser Doppler flowmetry and pulse oximetry, are physiometric tests that directly assess the blood flow within the dental pulp to determine its vitality, thereby bypassing the need for narrative feedback from the patient. However, laser Doppler and pulse oximetry are not widely available in dental care settings, owing to their high cost and the extra training required for interpretation of the results. Nonetheless, numerous studies have demonstrated sensibility testing to be reliable and accurate in determining pulp vitality and, as such, these tests have become accepted as standard practice.10,11,12
In both case reports described, the patients exhibited non-lingering reactions during pulp sensibility testing. In Case 1, the patient experienced discomfort when consuming cold food while, in Case 2, sensitivity occurred during exposure to cold water. These symptoms suggest a diagnosis of reversible pulpitis. Conversely, symptoms such as radiating pain persisting beyond the stimulus and causing sleep disturbances are indicative of irreversible pulpitis.12
After ascertaining the diagnosis, it was decided to perform complete caries excavation during a single appointment rather than step-wise excavation. This approach was chosen because complete caries excavation has resulted in better healing, as any remaining bacteria from selective caries removal can lead to continuous mild pulpal irritation, inflammation and, eventually, pulpal necrosis.14,15 Also, re-entry as in the cases of step-wise excavation has been considered unnecessary.16 During soft caries removal in Case 1, the pulp was exposed. Because the exposure occurred within an area of bacterial contamination, it was categorized as Class II pulpal exposure.1 A decision was made to proceed with DPC following a stringent protocol. Pulpal bleeding was managed with a 2.5% sodium hypochlorite solution, resulting in haemostasis in <3 minutes.
Subsequently, Biodentine was applied in both cases as a pulp capping agent. Biodentine, a calcium silicate-based bioceramic material, has demonstrated the ability to create a uniform dentine layer at the site of injury when applied directly to the pulp tissue.17 Adequate adherence between all layers of the materials used is an important issue with a high clinical impact. To ensure adequate sealing, RMGIC was applied in both case studies after the Biodentine had set. RMGIC exhibits high shear bond strength to composite materials, possibly because it includes 2-hydroxyethyl methacrylate, which enhances chemical adhesion between the RMGIC and the resin composite.18 Subsequently, composite restoration was carried out using the Palodent matrix in Case 1 and the saddle matrix in Case 2.
The entire procedure was performed with rubber dam isolation. Rubber dam isolation conducted before caries excavation is believed to enhance the success of VPT by creating a moisture-free environment, minimizing cross-contamination and enhancing the bond strength of resin composites to enamel.19
In the first case report, DME was performed owing to caries extension subgingivally in the mesial gingival margin of the tooth. This procedure was facilitated using Garrison's DME-01 kit. The advantage of using this kit is its ability to snugly adapt around the margins, ensuring proper contouring of the restoration. Additionally, with the DME matrix band in position, another sectional matrix can be employed over it to establish appropriate contact and contour.
An important factor in determining the success of VPT in permanent teeth is the ability to recall patients regularly. As histological success cannot be determined, clinical success is judged by the absence of any clinical or radiographic signs of pathosis and the presence of continued root development in teeth with incompletely formed roots as well as, in some cases, continued responsiveness to sensibility testing. Both the patients on recall at 1 year were asymptomatic and radiographs displayed no peri-apical changes or secondary caries.
Conclusion
The success of both direct and indirect pulp capping procedures was apparent in these patients' follow-up evaluations. Prioritizing the preservation of tooth vitality is of paramount importance. The success of VPT hinges on numerous factors, ranging from careful case selection to bacterial elimination followed by a well-defined course of action. The prognosis relies on the choice of pulp capping material and the implementation of techniques such as magnification, proper isolation, correct bonding procedures and precise use of matrix systems for optimal restoration.
This article endeavours to provide a comprehensive, step-by-step guide to managing both direct and indirect pulp capping procedures. Although success cannot be guaranteed, adhering to a well-defined and evidence-based plan enhances the predictability of achieving favourable outcome.