Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol. 2000; 71:743-751 https://doi.org/10.1902/jop.2000.71.5.743
Ebersole JL, Steffen MJ, Thomas MV, Al-Sabbagh M. Smoking-related cotinine levels and host responses in chronic periodontitis. J Periodontal Res. 2014; 49:642-651 https://doi.org/10.1111/jre.12146
Lung ZH, Kelleher MG, Porter RW Poor patient awareness of the relationship between smoking and periodontal diseases. Br Dent J. 2005; 199:731-737 https://doi.org/10.1038/sj.bdj.4812971
Kelleher MGD, Ower P. ‘Selfies’-an effective communication aid to solve periodontal and implant diseases. Dent Update. 2019; 46:12-22
Ralho A, Coelho A, Ribeiro M Effects of electronic cigarettes on oral cavity: a systematic review. J Evid Based Dent Pract. 2019; 19 https://doi.org/10.1016/j.jebdp.2019.04.002
Ruparelia R, Kelleher MGD, Dhanda LS. Darwinian dentistry? Social media, smartphones and selfie sticks. Prim Dent J. 2022; 11:75-80 https://doi.org/10.1177/20501684221088434
Burke FJT The genesis of minimal cavity design. Dent Update. 2019; 46:705-706
Hassall D. Centric relation and increasing the occlusal vertical dimension: concepts and clinical techniques – part two. Br Dent J. 2021; 230:83-89 https://doi.org/10.1038/s41415-020-2593-4
Edelhoff D, Sorensen JA. Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. 2002; 87:503-509 https://doi.org/10.1067/mpr.2002.124094
Kelleher MGD, Ooi HL, Blum IR. Facts and fallacies about occlusal philosophies for full mouth rehabilitation. Prim Dent J. 2021; 10:101-107 https://doi.org/10.1177/2050168420981529
Kelly RD, Kelleher MGD. Is ‘digital dentistry’ dangerous for teeth? problems associated with zirconia and CAD/CAM restorations. Prim Dent J. 2019; 8:52-60 https://doi.org/10.1308/205016819826439475
Kelleher MGD, Ooi HL, Blum IR. Changes in occlusal philosophies for full mouth rehabilitation. Prim Dent J. 2021; 10:50-55 https://doi.org/10.1177/2050168420981528
Hassall D. The use of the monolithic ceramic and direct monolithic composite in the aesthetic rehabilitation of tooth wear. Br Dent J. 2023; 234:406-412 https://doi.org/10.1038/s41415-023-5621-3
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Kelleher MG, Blum IR. Facts and fallacies about restorative philosophies for the management of the worn dentition. Prim Dent J. 2020; 9:27-31 https://doi.org/10.1177/2050168420911018
MSc, FDSRCS, FDSRCPS, FDSRCS, FCGDent, Specialist in Restorative Dentistry and Prosthodontics, Consultant in Restorative Dentistry, King's College Dental Hospital, London
This three-part series of articles challenges some popular myths about supposedly ‘ideal’ treatment plans and is designed to provoke reflection and stimulate debate. It explains the concept of ‘satisficing’, as opposed to ‘maximizing’, in dentistry, and illustrates how subconscious bias and self-interests might lead supposed experts to promote arbitrary aspirational standards and confuse them with what the law expects (the Bolam Test standard), and what is genuinely in the best interests of an individual patient. It is argued that sound, patient-centred pragmatic planning and treatment is equally valid, with wider applicability than routinely defaulting to a self-serving ‘maximalist’ approach.
CPD/Clinical Relevance: The ‘satisficing’ concept has wide and profound application across many fields of dentistry.
Article
‘Satisficing’ is a word created by combining ‘satisfy’ and ‘suffice’. It may be unfamiliar to some readers, but it is not new, having been first described in 1956 by Herbert Simon, who later won a Nobel Prize. It means approaching something in a way that is sufficient for it to be a satisfactory solution for the required purpose at the time in question. ‘Satisficing’ can be viewed as the polar opposite of ‘maximizing’, which involves seeking the single, supposedly ‘ideal’, outcome or solution to a problem. Maximizing tends to be a culture of idealism and excess, seeking out the most extreme, extensive, intricate or complicated approach, while satisficing aims to do what is necessary and achieve a perfectly reasonable, adequate outcome without the downside risks of that additional complexity and perhaps cost that maximizing tends to involve. Advocates of maximizing often claim that they are pursuing perfection, excellence or the ‘best’ solution, while satisficers may question the basis for, or validity of, such claims. This three-part series of articles examines examples of satisficing and maximizing across a wide spectrum of both clinical dentistry and other aspects of our professional lives in UK dentistry. It is deliberately challenging and potentially controversial in the hope of prompting self-reflection and discussion about who decides which approach is preferable, and who benefits most from the choices we and others make. Readers may find it helpful to read the three sections in their original order; Part 1 included several key references.
Part 1 explained and illustrated the concepts of satisficing and maximizing, and contrasted the application of each approach to the management of dead discoloured teeth. This second part moves on to consider the management of periodontal disease, caries, occlusal problems and tooth wear, and will then explain the consent issues and associated medico-legal risks.
The third and concluding part of the series will appear in the next issue of this publication.
Managing periodontal disease
Some periodontists might have vested interests in their enthusiastic promotion of their sub-specialty. Traditional ‘maximalist’ periodontists usually advocate the undertaking of detailed assessments, including initial and frequent recording of bleeding and pocket depth measurements, usually undertake some dental professional mechanical instrumentation, and sometimes sophisticated surgery, with the ultimate aim that, ideally, no patients should have pockets over 4 mm deep. That is despite a lack of long-term scientifically proven evidence that all of this emphasis on professional ‘measuring and dental professional instrumentation’ philosophy is a prerequisite for most patients maintaining a functional dentition.
Many ‘maximalist’ periodontists' preferred model involves ‘an external locus of control,’ meaning someone external to the patient is responsible for the preferred outcomes by undertaking multiple dental professional interventions with very regular ‘measurements’, recordings and reviews for ‘monitoring ‘of their periodontal diseases. Recently, some specialist periodontal societies’ guidelines have promoted the dubiously named ‘PMPR’ – an acronym for professional mechanical plaque removal – without enough emphasis being placed on the necessity for patients themselves undertaking daily very diligent manual plaque removal, especially using interdental brushing and avoiding smoking.
Some specialist periodontists contend that those subjective pocket depth measurements and professional interventions have to be undertaken at very regular intervals, regardless of their reproducibility, or the practicalities, or the various costs involved, or the pain/sensitivity sometimes caused by repetitive, sometimes aggressive dental professional interventions.
However, many in the ‘satisficer’ camp prefer to get the periodontitis-affected patient to get professional help to stop smoking, mainly on the grounds that smoking, present and past combined, has been reported as being largely responsible for over 50% of periodontitis.1 The Tomar and Asma study1 showed that current heavy smokers are about four times more likely than persons who had never smoked to have periodontitis. Among current smokers, 42% of their periodontitis was attributable to smoking, while 9% was due to former smoking. However, in the UK less than 10% of smokers are aware of that causative relationship, and one is left wondering who stands to benefit most from that striking gap in information and apparent understanding.2,3
It is unclear how encouraging regular attendance with a hygienist for the main purpose of re-cleaning the patient's teeth (often caused by chlorhexidine mouthwash staining) and recording detailed pocket charting and bleeding sites, before then doing some ‘PMPR’, gets across to patients the message that stopping smoking and the patient undertaking very effective daily interdental and intracrevicular cleaning at home are the really important changes that are required for that patient to sort out their periodontal problems.4 Incidentally, satisficers have not bought the smoking industry's nonsense about switching to ‘vaping’ as a way of giving up nicotine, because the mouth is the first port of call for vaping, and innocent-sounding vaping has known and, as yet, likely unknown bad effects on oral health.5
In order to demonstrate where the main problems actually are, and what to do about them, many satisficers disclose the patient with a cotton wool pledget held in tweezers drenched in a spectacularly coloured disclosing solution and dab it mainly over the most obviously inflamed areas (i.e. they don't use tablets).
They also apply that multi-coloured highly visible disclosing solution to the fit surfaces of any dentures.4 They show the patient the various right brushes to get rid of their plaque problems on their teeth but, very importantly, also on the inside of any dentures. Once the patient has a good idea how to use those cleaning brushes, a well-illuminated customized video can be made on the patient's own smartphone to show them where their most problematic bleeding areas are, and what they now need to do to get rid of the main causes of their periodontal problems. That customized video stays on the patient's smartphone as an easily accessible reminder for the patient of exactly what to do when they are doing their daily biofilm removal.6 Another advantage is that, once that information has been recorded as having been done on their mobile, they certainly cannot then claim thereafter that they were ‘never told about their smoking or problems’–as some opportunistic lawyers are inclined to allege.4,6
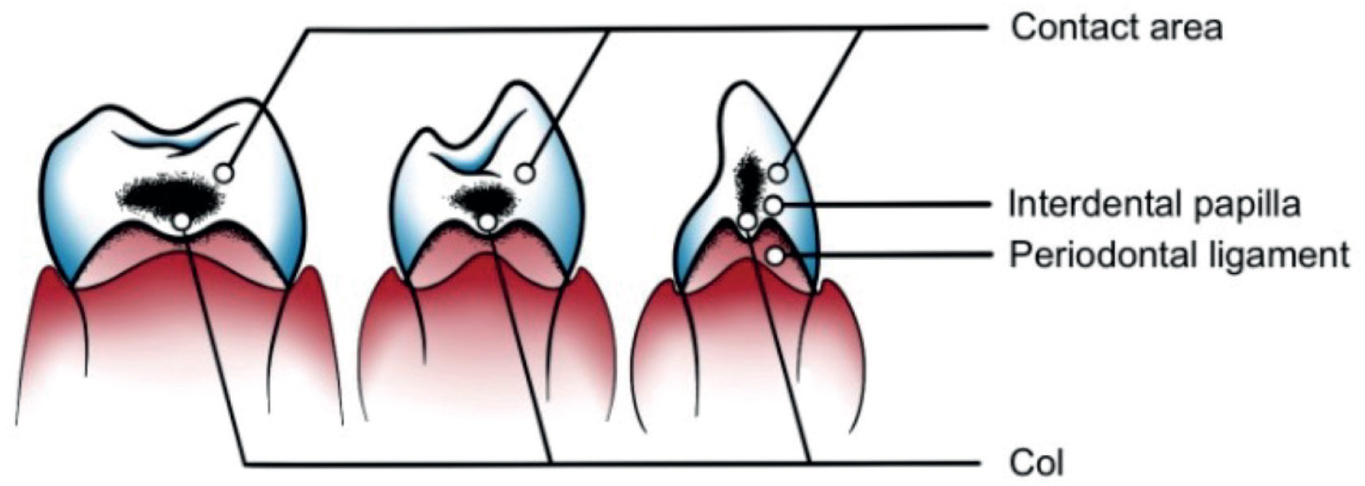
Many pragmatic clinicians suggest changing the proper meaning of that ‘PMPR’ acronym to emphasize the need for ‘personal, manual plaque removal’ in periodontitis-susceptible patients with them using the appropriate long-handled, tapering, different diameter, interproximal brushes from the insides as well as the outsides of all their problematic teeth to remove their plaque from their interdental cols. A col is a geographical term meaning a shallow depression between two hills. It is where the pathogenic bacteria accumulate between the peaks of the interdental papillae and below the contact zones (particularly in between wider back teeth) and cannot be removed effectively by using flossing or by most routine brushing (Figure 1).
Figure 1. The shallow depression between the interdental papillae is the col. It is where is where many periodontitis problems start, and are perpetuated because it is difficult to clean unless long-handled tapering interdental brushes are used.4,6
However, it is easy to explain the concept of a col to any patient by using the back of one's clenched knuckles to show them the shallow depression between any two knuckles and to say something like ‘those areas between the peaks of the gum on the inside and outside of your teeth are where your enemy bugs are camped and they are plotting to get rid of your teeth. You need to get rid of them with a long-handled tapering brush, pushing the gum down from both sides, in order to get at their camp and destroy them’ (Or whatever words you prefer, as long as the patient gets the main messages.) The periodontitis-susceptible patients also need to understand that they usually need to use a single-tufted brush vertically to clean their gingival crevices very effectively, every day, as well as using conventional manual or electric toothbrushes to accomplish those tasks effectively, if they want to keep their teeth in the longer term (Figure 2).
Figure 2. Satisficers aim to get the most important messages across effectively and quickly, with some simple messages, i.e. ‘stop smoking and do sufficient daily effective cleaning of your teeth for it to be satisfactory for controlling your gum disease problems’.
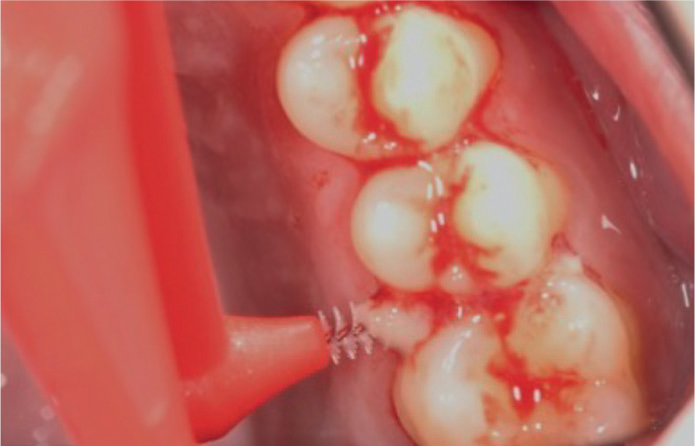
Many patients remain blissfully unaware of problems with their gums. Showing them where their bleeding areas are is accomplished better by inserting a long-handled interdental brush from the insides of their back teeth, rather than by using a sterile periodontal probe (Figures 3 and 4). The real danger with using a standard periodontal probe for initial diagnosis, rather than an interdental brush from the inside of all the teeth to produce the immediate or delayed bleeding, is that many patients think that because the sterile probe is a surgical instrument (that only dentists or hygienists possess) that this really means they must have a mainly surgical problem. Consequently, many assume that ‘an external locus of control with surgical instrumentation’ is now required rather than their problems being caused by their inadequate personal interdental grooming problem.
Figure 3. Bleeding on introduction of a long-handled interproximal brush from the inside of their affected back teeth shows a patient where their problems are, and how to disturb their ‘bugs’/biofilm/plaque from their problematic col areas.4Figure 4. A customized selfie video, made on a patient's smartphone, of their bleeding sites immediately after using an appropriately sized interproximal brush provides a graphic reminder that their gum problems result from a ‘failure of personal dental grooming’ rather than it being a surgical problem, or one that has to be dealt with by someone else.
Using a long-handled interdental brush with a tapering diameter to go through the obviously most inflamed areas from the inside of their back teeth, while they watch in a mirror, gets the message across that it is a personal grooming issue that they can solve themselves, and get the benefits of better breath and gum health.
Figure 5 shows images of a patient using different sizes of long-handled tapering interdental brushes from the inside and outside of their teeth and a single-tufted brush with the correct techniques. Their resultant bleeding was recorded on their smartphone (Figure 4) by using a ‘selfie holder’ and a ring light for effective illumination of the back of the mouth. The selfie set-up shown is in widespread use for make-up sessions, so beloved of Instagram and other posters on social media. It is cheap (about £30) and readily available from various suppliers.
Figure 5. (a) An illumination system and a ‘selfie stick’ to hold the patient's own smart phone to record them doing the effective cleaning that they need to do daily in the privacy of their home. (b) The patient's smartphone is held in the selfie stick and used to record the different-coloured long-handled brushes to clean from the inside and outside to remove the plaque from their cols, and to remind them of which brushes go where.
The smartphone recording of the patient doing what is required for their oral health (as well as helping their social and/or love life because of the elimination of bad breath) reminds them of which interproximal brushes to use, and where and how to remove their biofilm/plaque from their interdental cols.
Using the right brushes for the right spaces
It is sensible to provide the periodontitis-affected patient with a selection (‘a rainbow of colours’) of the appropriate tapering interproximal brushes at their first appointment so that they can clean from the insides, as well as the outsides, of their problematic teeth straight away (Figure 6).
Figure 6. A rainbow of different coloured handles indicate the different diameter (and consequent increasing durability) of the interproximal brushes.
Long handles are preferred because they can be used from the inside of all the side and back teeth to get at the vulnerable wider cols, which are most difficult to clean properly.
A ‘mouth map’ can be made for them and also recorded on their smartphone to remind them which ones to use and how and where to use the different ones.
If the practice does not wish to supply the wide variety of different tapering long-handled brushes in the future, then the website name of an appropriate supplier should also be given to the (hopefully now enthusiastic) patient so that they don't have to waste time and money hunting to get their correct replacements.
As an aside, to reduce plastic pollution related to the conveniently coloured plastic handles (which indicate their diameter and shapes), an ecologically sounder ‘satisficer’ approach would be for the patient to acquire three or four metal handles with a ferrule type of attaching mechanism for securing the different diameter tapering brushes. Having those durable metal handles would mean that the patient would then only need to dispose of the replaceable tapering heads rather than the head and the attached plastic handles. If there was sufficient demand in this more environmentally conscious era, that sort of system could be manufactured cheaply enough to make them a feasible proposition for many periodontitis-affected patients. This is not a new idea. A Canadian company, Butler, were selling these in the 1970s, but the costs deterred many patients then from using them. Many satisficers suggest to the patient that they can get an awful lot of brushes for the cost of multiple dentist or hygienist appointments. However, some commercially minded maximizer dentists, hygienists or their practice managers might stock and sell them if they had space, but some others might choose not to draw attention to this aspect, perhaps for understandable commercial or other reasons. However, many satisficers' experience has been that many patients are so grateful to be given such care, hope and useful practical advice that they become loyal and vocal supporters of that practice.
Satisficers routinely disclose any dentures to show the patient where their mature Gram-negative pathogenic biofilm is growing undisturbed on the fit surfaces of their dentures (Figure 7). Once the patient can see that graphic evidence, it is usually not difficult to get the patient to understand that if their previously unseen, but tenaciously adhering plaque is not removed properly from their denture every day, then that particularly nasty plaque is being re-inserted undisturbed and thereby is re-infecting the pockets on their critically important supporting and stabilizing/retaining abutment teeth.
Figure 7. Satisficers disclose any denture and video the patient cleaning the fit surfaces of their partial dentures correctly.
Unfortunately, some traditional partial denture design teachers still persist in extolling the supposed ‘primary requirement for support’ to distribute the occlusal loads widely in order to avoid progression of periodontal disease around abutment teeth. That fallacy keeps on being repeated in many undergraduate programmes. The real truth is that it is more often the undisclosed and undisturbed mature plaque adhering grimly on to the partial denture guide planes, occlusal rests or other minor connectors, as well as the fit surfaces of the dentures, that is the much more likely cause of progression of periodontitis around many abutment teeth in periodontitis-susceptible patients. Those adhering pathogenic bacteria simply wander across to re-colonize the pockets when the ineffectively cleaned denture is re-inserted, and they are responsible for the hypertrophic chronic inflammatory granulation tissue often present due to the body trying desperately to combine protective inflammation and attempts at healing.
Partial dentures are often called ‘gum strippers’, but this not due to excessive occlusal forces, but rather because partial dentures are brilliant at accumulating mature pathogenic bacteria and re-supplying them to the adjacent pockets around critical abutment teeth.
Many patients are social prisoners to their partial dentures, but many have never had their dentures disclosed and had a record made for them on their smartphone of how to physically clean the inside of their dentures daily with the appropriate brushes (Figure 5).
Ubiquitous and unchallenged advertising by commercial mouthwash and denture-soaking companies has convinced many denture wearers and, sadly, many unquestioning dental professionals, to believe in expensive, but near-useless mouth rinses and denture soaking fluids and to tacitly accept that they are equally good and equivalent to efficient physical plaque removal from their dentures, especially on the inside of the teeth where these appliances contact their critical abutment teeth. That is why graphic disclosing solutions and videoing of the patient doing what is actually required is so valuable for them in order to deal physically with the pathogenic biofilm on their dentures and in their nearby gingival crevices (Figure 7).
Use of limited time and resources in periodontics?
In spite of many satisficers advocating these patient-empowered approaches as being capable of producing better patient outcomes, as well as being a better use of scarce time and resources, many traditional ‘periodontal maximalists’ and some hygienists still prefer to spend the available time doing dubiously reproducible measurements of bleeding and pocket depths at arbitrary intervals. It might not do much to benefit their patients, but at least they maintain laudably copious records that may provide some protection against any passing ‘no win, no fee’ law firms and some tame ‘experts’ employed by them, and not least, the critical gaze of the GDC. So, a ‘maximalist’ approach might ultimately benefit many dental professionals, or specialist periodontists, even if not practically helping many trusting patients, many of whom have limited incomes.
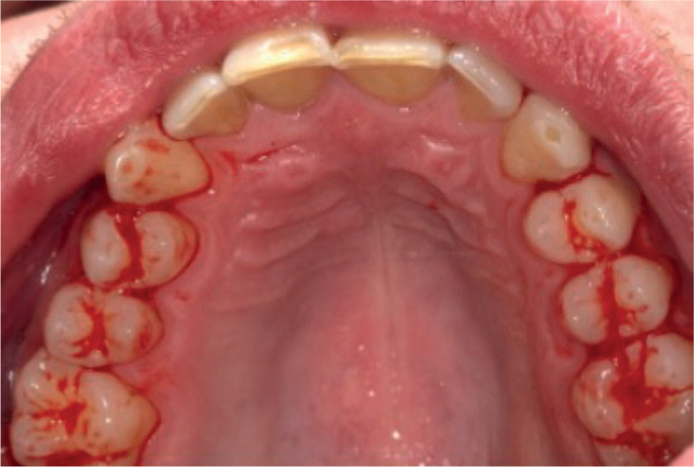
Sadly, various iterations of periodontal classifications and guidelines now appear to have ‘lost the plot’ by emphasizing the supposed need for the dubiously named ‘professional mechanical plaque removal’ at both the initial and follow up treatments. Unfortunately, and perhaps unintentionally, that reinforces the message in many patients' minds that that they are somehow largely dependent on those other people for controlling their gum problems. Cultivating that dependency may not particularly help to address the patient's disease, but it is certainly in the interests of the dental health professionals upon whom the patient then often comes to rely very heavily. Sadly, this pattern of care is the sort of experience that so many patients report when they present themselves at a dental hospital for the first time with significant periodontal problems. Many patients report visiting the hygienist every 3 months in the mistaken (and expensive) belief that it is what the hygienist ‘cleaning’ does will somehow cure their problems, even if they don't stop smoking or clean their teeth effectively every day in between these visits. In whose interests is the perpetuation of such ‘maximalist’ myths? The business model of many practices is often predicated on the secondary income from hygienists routinely removing what is often tooth surface staining without local anaesthetic. This is often the highly visible and unsightly chlorhexidine discolouration caused by the largely useless mouth rinses that are frequently suggested by commercially driven multinational pharmaceutical companies, by many hygienists and sadly, even some dentists as being ‘adjunctive periodontal cleaning aids.’ However, the rarely quoted Richards (2017) article in the BDJ's Evidence Based Dentistry publication showed that 50 out of 52 studies on mouth rinses had minimal and clinically irrelevant effects on treating periodontitis, but many caused significant staining (Figure 8).7
Figure 8. The patient had attended every 3 months for ‘monitoring and PMPR’ for 5 years. The hygienist was emphatic that using a chlorhexidine mouth rinse daily was an essential part of maintaining his gum health. The chlorhexidine staining is worse on the composite restorations due to their higher free surface energy reacting with the chlorhexidine.
In summary, plaque removal needs to be done daily by the correctly informed, enthusiastically motivated and empowered patient, taking personal responsibility for their own gum diseases. The ‘cure’ is certainly not routine visits to a hygienist four times a year for measurement and ‘monitoring’ with a gentle wafting of an ultrasonic tip, often without local anaesthetic, with some encouraging them to use expensive, useless, but staining mouth rinses, perpetuating the dependency cycle.
Yet this very approach is tacitly encouraged by certain specialist periodontal societies, academics and indemnifiers, and is expected by draconian regulators and their tame experts. Cynical Irish farmers have an expression about the ‘regular measurement’ approach, which is that ‘weighing the pig won't fatten it.’ Sadly, this sage advice is absent from most periodontal society or dental journals.
Many experienced and compassionate satisficers know that what the patient does both by stopping any smoking (and avoiding/stopping vaping) and doing very effective daily cleaning is sufficient to solve the vast majority of periodontal problems. What is not helping is the self-serving mystique that has been built up around the accumulation of multiple, often useless pocket depth numbers (which are, as mentioned, often of dubious scientific value or reproducibility).
Let us be clear: the ultimate beneficiary of these ‘measuring and monitoring’ processes is not the patient; but there is money to be made by those in the ‘counting houses’, by the hired gun expert witnesses often commissioned by the GDC, by the eager battalions of ‘no win, no fee’ law firms for whom ‘untreated’ (or more accurately, ‘unmeasured’) periodontal disease is viewed as a gift from above, and by the thriving new opportunistic ‘clinical record audit’ industries providing illusory quality assurance for bodies such as the NHS.
In Part 1 of this series, we mentioned the quality giant, Phil Crosby, whose intellect and insight regularly cut through fashionable nonsense and debunked popular myths and misconceptions. He warned that many activities were mistakenly described as quality assurance when they were nothing of the sort. Quality assurance, argued Crosby, is the prevention of quality-related problems, through planned and systematic activity that can be shown to be effective most of the time.8 It is an organizational culture with a clear focus on the end-goal, not fruitless activity for its own sake, or for the sake of outward appearances.8 He added that inspection/audit after the event is not quality control because it relies on retrospective detection rather than prevention. It can be a valuable tool for reflection, learning and development, and quality improvement, but that's not the same thing.8
‘Maximizers’ versus ‘satisficers’ in managing caries
The traditional GV Black cavities and philosophical approach were an obvious example of ‘maximalism’ when dealing with caries, including ‘extension for prevention’ into those areas that were not yet affected by caries, but were deemed to be at risk of developing it in those pre-fluoride toothpaste days.
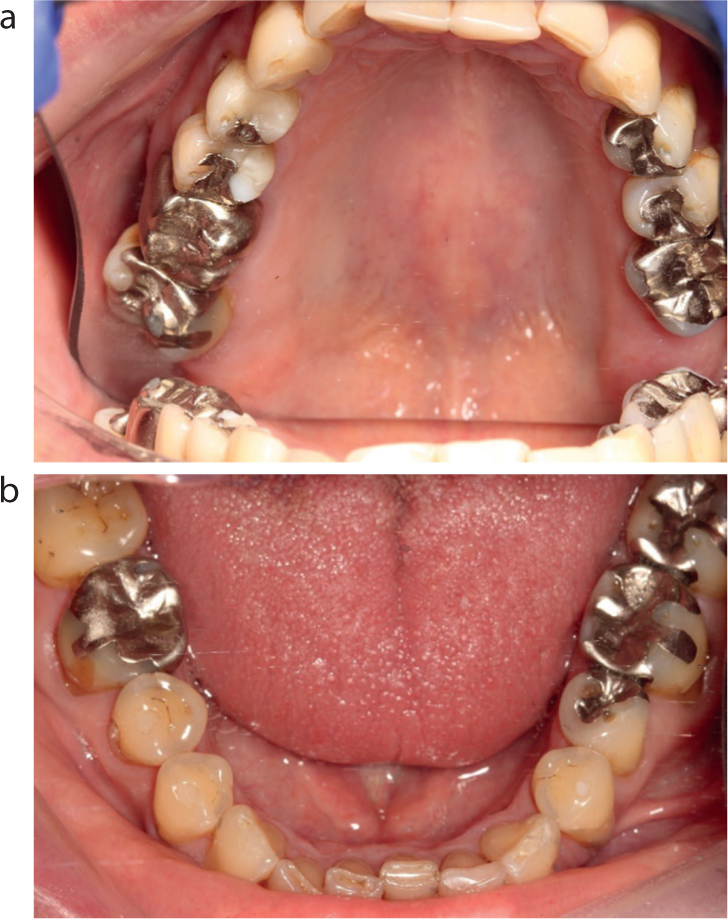
In 1949, the invention and patenting of the airotor by John Patrick Walsh in Otago, New Zealand was the disruptive technology of its day, because it allowed quicker and much more efficient cutting of hard tooth tissue. The subsequent development of the Borden airotor in the USA, coupled with the design of different burs, meant that access was now much easier to remove all of the caries. Cavities were designed because of the limitations in the materials available at that time (amalgam and silicate) and adhesion had not yet been developed. Consequently, the durability of the restoration was what was measured rather than the long-term survival of the tooth being the main focus (Figure 9).
Figure 9. (a,b) Traditional cavity preparations for different materials reflected the limitations and benefits of the available materials and were destructive. These restorations are over 35 years old and have given no trouble. Traditional restorations required significant skill and, for many dentists, were beautiful in their own way. They were judged on their durability, rather than on the survival of the teeth being the main focus.
Variations on Black's principles of cavity preparations evolved subsequently, which reflected the changing philosophies of some pioneers, the tooth cutting technology then possible and/or the dental materials being available. However, although the word had yet to be invented, some of the subsequent satisficers of later times gradually suggested the use of smaller cavities with different cavo-surface angles and the removal of just the caries off the amelo-dentinal junction and most of the soft caries, but taking great care not to endanger the pulp.9 Those less destructive approaches got modified further to just removing the obvious caries locally and then using sealing and bonding techniques along with ‘aggressive prevention’ as the dental materials and biological understanding of pulps and caries improved, as well as fluoride being added to nearly all toothpastes, and those being gradually accepted as the normal toothpaste.
In the 1970s, various visionary clinicians including New Zealand's John Rodda and England's Dick Elderton advocated doing less tooth destruction to ‘satisfice’, even if they did not term it that, and many others since then have advocated progressively less, and latterly ‘minimal’, dental destruction when managing caries.9–11 Elderton and Sheiham were among the first to describe and warn against ‘the restorative cycle’ whereby restorations got bigger and the remaining tooth structure got less each time a restoration was replaced.10–12 Many other aware and concerned clinicians realized that developments in adhesion were game changers and contributed in various ways to the evolution of minimally destructive dentistry.12
However, this was an uncomfortable and unpopular direction of travel among some ‘maximalist’ dentists. Some, having acquired the necessary manual skills, were rewarded well by the remuneration systems in operation at that time because the more you did, the more you earned. For instance, an MOD filling was worth more than an MO and much more than a single-surface filling. A crown was worth a lot more than any filling, partly offset by the laboratory fee.
Multiple crowns were quicker, easier and more lucrative to provide than a single crown. More extensive crown preparations could be and were done under the cover of a supposed necessity for idealized occlusion or for appearance reasons, and those justifications were promoted very strongly by various ‘occlusal gurus’.13 Advocates of ‘reliable maximum intervention’ were also being comforted by the support of reactionary group thinking and were (and some still are) reluctant to see the light and stop destroying their patient's finite and precious ‘dental capital’, which, one might cynically observe, they perhaps view as being more disposable than their own tooth structure, or that of their immediate family.13
Many actively resist doing the minimum that would meet the criteria to ‘satisfice,’ and some resort to ridiculing the minimally destructive approach and to using spurious terms such as ‘360-degree veneers’, instead of calling those full coverage ceramic crowns. Biologically sound concepts have been opposed by some voluble members of the ‘destructodontista’ tribe, many of whom have now found justifications for destroying sound tooth tissue under the pretext of providing the disputable benefits of the appearance of monolithic ceramics, or their durability, or to provide an ‘ideal occlusion’ or a more attractive smile.13
As increasingly more clinical evidence has been amassed for the medium-term success of adhesive approaches to managing wear, which have a predictable, very decent fall-back position of the residual sound tooth structure still being present, allowing a further round of refurbishment, unnecessarily destructive mutilation of largely sound teeth for full coverage ceramic restorations undertaken for ‘cosmetic reasons’ or for ‘occlusion reasons’ has attracted criticism.14,15
‘Maximalists’ and ‘full-mouth rehabilitationistas’
The usually stated aim in undertaking an alleged ‘full-mouth rehabilitation’ is to restore all the biting surfaces of all of the teeth in order to provide optimal chewing efficiency with asymptomatic masticatory muscles and temporomandibular joints. Many of those occlusal teachings were well meant at the time they were introduced. However, closer examination reveals that many of them involved serious destruction of mainly sound tooth tissue,16 without necessarily delivering all of their purported benefits.13 The biological and structural disadvantages of ‘subtractive’ dental procedures, were, and still are, undertaken to provide traditional ‘full-mouth rehabilitations’ (spelt ‘full-mouth mutilations’).
Satisficers contrast such approaches with the proven advantages of pragmatic, minimally destructive, additive techniques, which can solve frequently encountered clinical problems, previously deemed to require traditional ‘full-mouth rehabilitations.’ A more accurate term would be full mouth destructodontics because of the structural, pulpal and longer-term periodontal problems that were often inflicted on many innocent teeth in the pursuit of those biologically dubious goals. In truth, the pursuit of the alleged nirvana of ‘occlusal perfection’ often became the enemy of the long-term good of many patients' teeth and dentition, especially in their later years. Edelhoff and Sorensen demonstrated that approximately 63–72% of a tooth's coronal tooth structure is destroyed (in double-quick time) by the preparations for classic full-coverage metal–ceramic or all-ceramic crowns.16 It is a fallacy that doing this amount of destruction is likely to improve the prognosis for any posterior or anterior tooth treated in that way, and most dentists would avoid having that amount of destruction done to their own teeth, or to the teeth of their children. However, various ‘occlusionistas’ or ‘rehabilitationistas’ have claimed that it is getting the occlusion right that is the key to solving many dental problems and that dentally destructive approaches are justified to achieve that objective, just as long as the right ‘preparations’, articulators, materials and technicians are involved.13
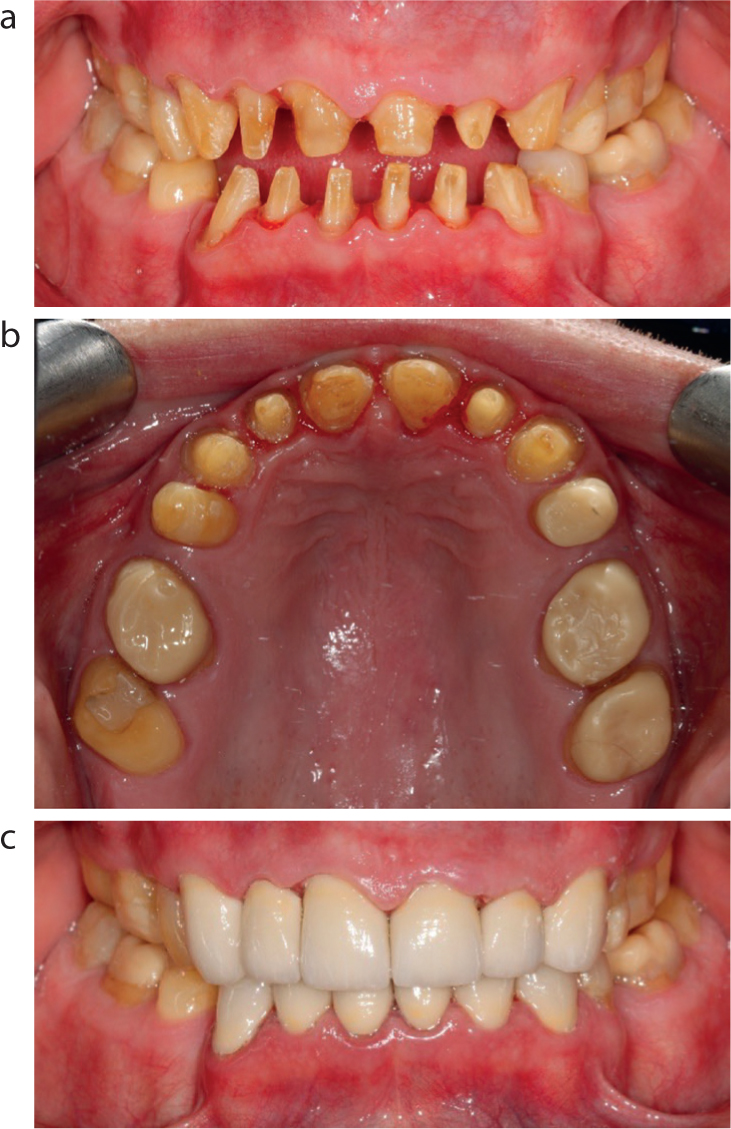
Many problems, such as amelogenesis imperfecta, are still treated with very destructive approaches (Figure 10) as though the adult teeth are some sort of intermediate secondary dentition that the patient gets after their primary dentition and can be mutilated in pursuit of some full-mouth rehabilitationist's cult-like beliefs. Their fall-back position appears to be that because the teeth were suffering from genetically determined enamel/dentinal defects, or from serious dental problems caused by decay or trauma, that one can do whatever destruction one likes in pursuit of an occlusal or cosmetic dentistry goal because there is, in theory at least, a supposedly ‘permanent’ implant-retained dentition to fall back on, which some cult like maximalist believers prefer, possibly for a variety of motivations (Figure 10).
Figure 10. (a–c) Amelogenesis imperfecta treated with multiple full bonded crowns with obvious long-term structural and periodontal problems and dubious appearance.
Is maximalist dentistry justified by occlusal philosophies?
Myths and fallacies surrounding occlusion are still perpetuated about the alleged causal relationship between occlusion and the development or treatment of temporomandibular joint disorders, or the development of infra-bony defects in periodontitis.17 Both of these treatment approaches have been discredited, but the long-term effects of true believers in ‘occlusal treatment’ for either, or both, lingers on in the ‘heavy metal brigade’. Worryingly, a potentially large new group is being added and many are likely to have long-term pulpal, structural and other problems because of the current fad for extensive elective ‘digital dentistry’, which often involves very heavy ‘preparations’ in order to use scanners easily and use ceramic-veneered zirconia.18 Some destructodontists have re-emerged in a new guise as ‘digital dentistry full-mouth rehabilitationists.’ Many enthuse on their websites, and in some case reports on various platforms about the supposed benefits of ‘digital dentistry,’ often by using monolithic or veneered zirconia. Worryingly, this gushing enthusiasm by various charismatic digital dentistry gurus has unleashed a tidal wave of needlessly destructive dentistry, with nonsensical or questionable occlusal philosophies,19 now being re-hashed as a justification for those treatments because it is ‘new and better’ (which is itself an oxymoron).
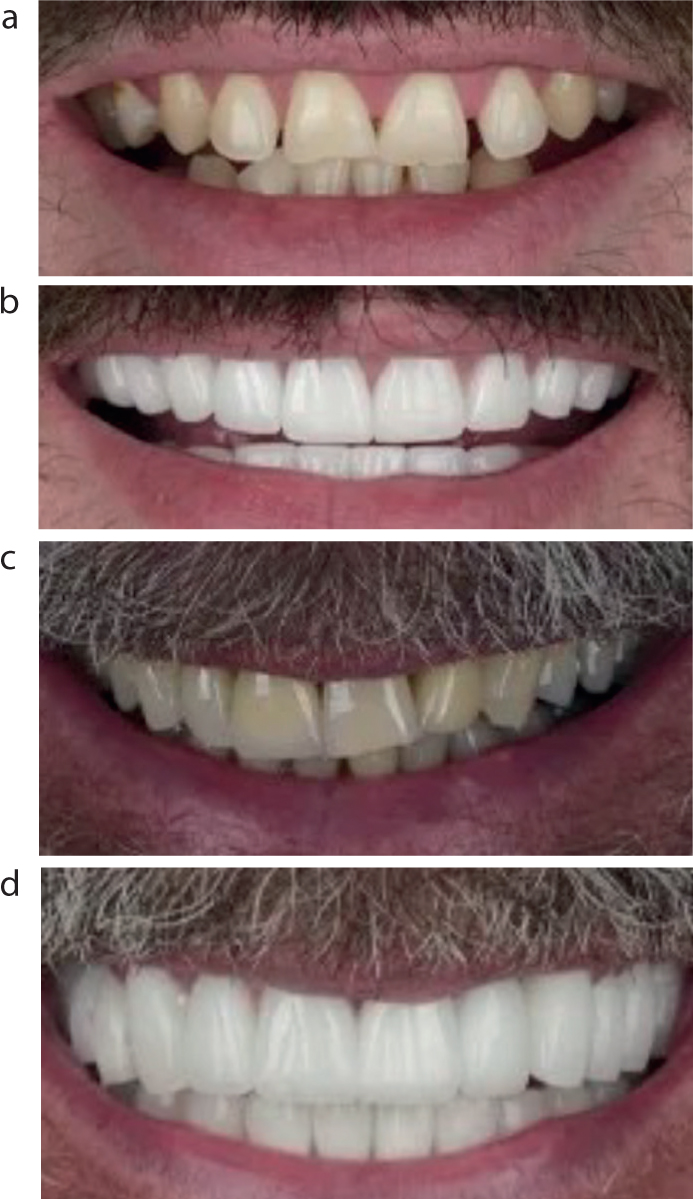
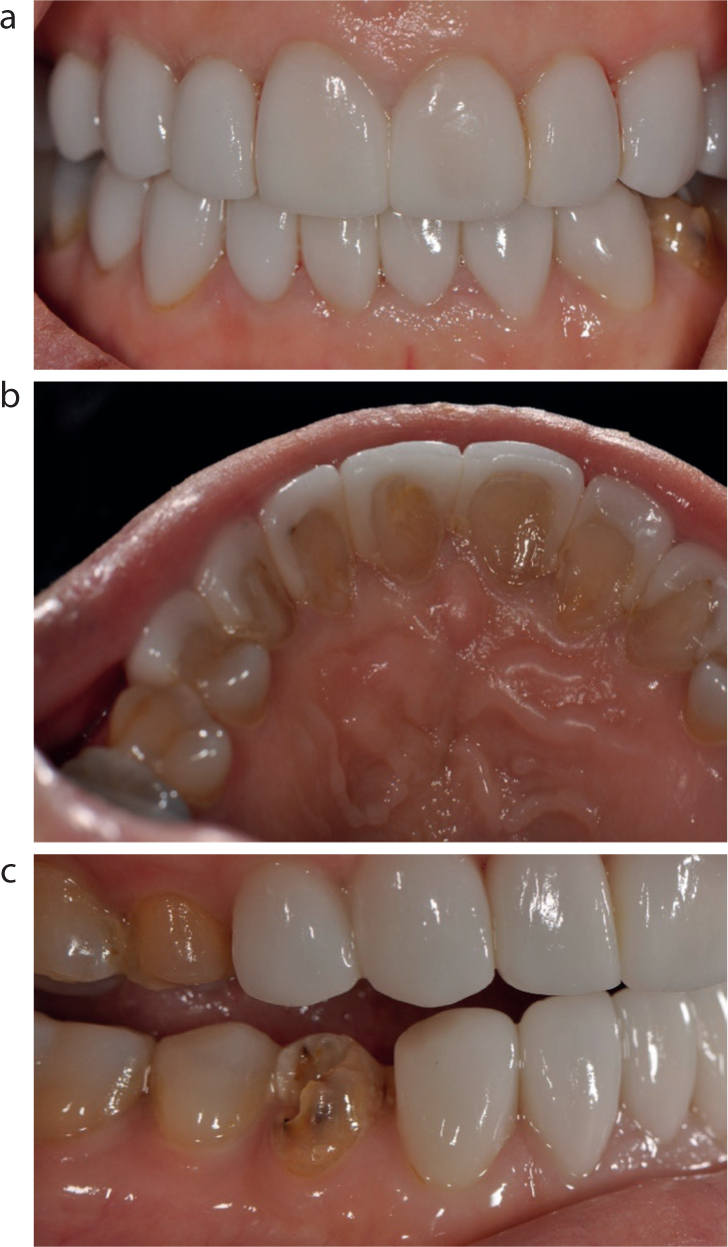
Aggressive advertising and unproven claims on various platforms of being the ‘latest and greatest’ have caused some gullible dentists to fall for crassly superficial straplines, which are often used to promote needlessly aggressive techniques involving various new and clinically unproven variations of ceramic materials (Figures 11 and 12).
Figure 11. (a–d) These sorts of aggressive full-mouth ‘mutilectomies’ for ceramic restorations are quite quick and easy to do, but are highly destructive of sound structure. The problems could have been dealt with in a satisficing way with some bleaching and bonding which would have improved the appearance, but left all the sound tooth tissue intact for the patient's future.Figure 12. (a) An upper occlusal view of the upper arch of the third ‘occlusal rehabilitation’. A more appropriate description could be ‘a ceramic cemetery’ concealing the dead and root-filled teeth underneath. (b) This ‘ceramic cemetery’ conceals a multitude of problems caused by the previous, and this latest ‘full-mouth rehabilitation’. (c) The OPT showing where many teeth were murdered and root filled, and some were extracted to provide implants as part of a ‘maximalist’ approach to full-mouth rehabilitation for ideal occlusion and aesthetic reasons. These teeth were intact prior to having three full mouth rehabilitations in a vain attempt to get the ‘perfect occlusion and the perfect smile’. Please note what is left of the teeth and how many have died, been root filled or removed and replaced by implants in pursuit of that goal. Was all that elective dental destruction justified for occlusal philosophical and cosmetic ‘maximalist’ reasons?
‘Satisficing’ solutions for managing tooth wear
In 1962, Declan Anderson, an oral physiologist and polymath working in London, showed that patients readily adapted to planned changes in their occlusion.20 Although rarely cited, Anderson's paper pre-dated the later publication of Dahl et al by 13 years.21 Since then, various advancements in adhesive bonding systems and developments in resin composite materials have allowed many dental problems, such as tooth surface loss, to be treated successfully by using local occlusal changes without causing significant dental destruction, unlike the often lazily quoted supposed ‘Dahl principle’, which actually involved a removable appliance prior to undertaking modified crown preparations.
Multiple clinical studies have shown that most patients adapt well to planned occlusal changes for managing their wear and other problems.22 It appears that most tooth wear patients are ‘satisficed’ – provided that they have given their consent (after being warned fairly in advance of their requirement for adaptation and the costs of future maintenance) and are happy with the change in their dental appearance, meaning that the approach has solved their perceived problems of their significantly worn teeth. In other words, the price they pay for preserving the mainly sound tooth structure of their remaining natural teeth is some effort by way of adaptation, but, once explained in advance, most are happy to ‘satisfice’ in that regard (Figures 13 and 14).22
Figure 13. (a,b) Mainly erosive tooth surface loss in a 35-year-old male who was treated with ‘satisficing’ bleaching and additive direct bonding to protect the residual tooth structure.Figure 14. (a–c) Ankylosed deciduous maxillary canines in a former smoker: mixed aetiology tooth surface loss treated with ‘satisficing’ NGVB bleaching for 5 weeks, followed by additive freehand direct bonding.
Sadly, in spite of the widespread trend towards minimally destructive dentistry by adding to worn, but largely sound teeth, recent articles and advertisements advocating extensive subtraction of tissue from mildly worn teeth to produce dubious outcomes using monolithic ceramic have still been appearing in various dental publications and also on various platforms and websites.13,23
Satisficing approaches in aesthetic dentistry versus ‘maximalist veneereology’
There are only a limited number of cases that can be treated with ceramic veneers when the preparations are to be kept in enamel. However, various opportunistic pathogens, called ‘veneereologists’ have increasingly found more cases that could be treated rapidly and lucratively with multiple ‘extended ceramic veneers’. Now the twin forces of consumer demand and opportunistic dentists have come into alignment to ‘maximize’ the number of veneers that are deemed to be required. This expansion has morphed from doing just one ceramic veneer, which was difficult to shade match in different lights because of metamerism, to two ceramic veneers, which are quicker and easier to match. Four ceramic veneers then became fashionable and, rather conveniently, seemed easier to do as well as more profitable. For a few people, six veneers would do, but that did not address the perils of not ‘widening the buccal corridor.’ Undertaking four more extended veneers for widening the buccal corridor became more popular and even more lucrative for the ‘cosmetic dentistry’ maximizers and self-styled ‘smile scientists’ who seemed blissfully unaware of the dental damage being done in their pursuit of the highly subjective ‘perfect smile’ (and the even-more-perfect bank balance). In fact, many cases shown involve reverse three-quarter ceramic crowns that destroyed much of the valuable load-bearing marginal ridges and damaged many previously healthy pulps with direct trauma, as well as inadequate temporization to add further insult to injury (Figure 15).17,18
Figure 15. (a–c) This patient had given her consent for 20 veneers, but what was done to those teeth was more like preparations for three-quarter style ceramic crowns. When two came off they exposed how much sound tooth had been removed. Was her consent really valid? Open to question?
To provide the supposed ‘training’ and justification for all that destructive activity, and to provide a very thin veneer (no pun intended) of pseudo-science, various ‘study groups,’ ‘institutes’ and ‘academies’ sprang up to provide certification of training, or just proof of ‘cult’ membership. Various charismatic gurus from the US found untapped audiences on this side of the pond and offered (for a not-entirely-modest fee) to sprinkle their fairy dust on the acolytes attending. This in turn seemed like an attractive and proven model for home-grown aspiring gurus to follow, and so it has proved. It was Peter Drucker, the founder of management consultancy who quipped that Americans prefer the word ‘guru’ because they can't spell the word ‘charlatan.’
Satisficing, maximizing and issues of consent
Consent has come to be one of the hottest topics in the dento-legal field. It is often very easy for a patient to argue, after a suboptimal or adverse outcome of some kind, that ‘I would never have agreed to go ahead with this treatment if I had been warned that x might happen.’ When the Woolf (‘Access to Justice’) Reforms to the civil justice system were introduced in 1999, it permitted conditional fee arrangements (popularly known as ‘no win, no fee’) for personal injury and clinical negligence claims, for the first time in the UK. It is debatable whether the main beneficiary of these reforms ended up being the patients (as intended) or the legal profession because the claimant's legal representatives can earn huge amounts of money if they carefully select the cases they take on. But in order to open the cashpoint, their client's claim must first succeed. To make this more likely, the list of allegations (of negligence) tends to be very long, and invariably includes one or more ‘consent’ allegations. Only one single ‘breach of duty of care’ allegation needs to be proved in order for the claim to succeed, so the allegations are often framed so that if one fails, one of the alternative allegations will succeed. The more entrepreneurial law firms learned very quickly how to make the system work to their benefit.
One of the legal tests applicable to a negligence claim is known as ‘causation,’ which essentially means that the claimant must show that, on the balance of probabilities, they would not have suffered the harm that resulted if the defendant had acted differently in some way. This could relate to something the dentist did, or failed to do, but very often it relates to what the patient was told (or not told) at the time they were asked to give their consent, about the nature and purpose of the procedure(s), the risks, limitations and benefits, the likely outcome/prognosis and how all this compares to any alternative treatments that might be available.
There are risks associated with both satisficing and maximizing, and a lot depends upon the nature and quality of the communication between dentist and patient. However, the consequences of getting it wrong when you have been ‘maximizing’, are likely to be considerably greater than had you been ‘satisficing’ – both in financial (damages) terms, and in terms of recovering the situation.
Many satisficing approaches leave the patient no worse off, such as with bleaching and direct bonding,24,25 whereas the same cannot be said for a lot of maximizing approaches, many of which are destructive and often irreversible, with possible long-term consequences. Of course, a few minutes of conversation with an eager no win, no fee lawyer is often sufficient to convince a patient that they were given incorrect or misleading information, or insufficient information or warnings about risks. This is where it does make good sense to keep full and accurate records of those key conversations. The least defensible scenario, in terms of both civil (negligence) claims and GDC complaints, is an allegation that the patient was talked into, steered towards or (worse still) pressurized into a maximalist approach, without having been made aware that simpler, less risky, and perhaps less expensive ‘satisficing’ options would have been available to them.
In a civil claim, the claimant still needs to be able to demonstrate that they would have chosen the ‘satisficing’ option had they been aware of it, but in most cases that is a more credible argument than the reverse. The law attaches little significance to the commercial aspects of the transaction, i.e. the cost implications of treatment and treatment choices, but the same cannot be said of the GDC and its Professional Conduct Committee, which regularly allows itself to assume a commercial/financial motive into a dentist's actions. Its default presumption, revealed even in its published guidance, Standards for the Dental Team, is that the least expensive treatment option is inherently desirable, and you would need to have a pretty compelling reason to charge the patient much more.
Not uncommonly, dentists report and/or state in the clinical records that a patient presented ‘wanting’ treatment A, ‘demanding’ treatment B, or was not interested in option C, or that they refused or declined option D. Any of that may well be so, but a lot depends on what happened, and what they were told, before they came to their decision. They may have been influenced by what the dentist has told them face to face, or what others have told them, what they have read somewhere, or what they have gleaned from the TV, or a practice website, or from social media. When seeking a patient's consent, it is not enough that they seek out the practice specifically wanting to improve the appearance of their teeth; that does not give us carte blanche to decide unilaterally how best to achieve that. Instead, we need to make them aware of all the options and how they compare in terms of what they involve, what they can and can't achieve, the potential risks and benefits, and what the likely outcome is. Plus, the cost and time implications of course.
A clinician may well have a personal preference to treat a patient, or a clinical situation, in a particular way.13,23 That clinician might even believe that it is the ‘best’ way or ‘treatment of choice,’ and there is nothing wrong with explaining that viewpoint to the patient in a fair and balanced way – explaining any downside or material risks as well as the upside benefits. Similarly, any clinician has a right to decline to provide treatment with which they disagree and explain their reasons for doing so.14,15,17–19
But either way, the patient must understand that other approaches are, or might be, possible, and might be offered by a different dentist, and we should certainly not deliberately withhold such information from them or imply that no such alternatives exist.22,24,25
The GDC states in its guidance to registrants that they must always put their patients' interests before any other consideration, or any financial, personal or other gain. It also reminds registrants that they must find out about and follow current evidence and best practice, and if they decide to deviate from established practice and guidance, they should record the reasons why, and be able to justify their decision.
This clear guidance should concentrate the mind and hopefully ensure that patients and their short- and long-term interests are always paramount when alternative treatment approaches are being considered.
Summary
It is time to redress the balance in providing practically available dental healthcare by recognizing that pragmatic ‘satisficing’ is an equally valid philosophical approach to solving dental problems as ‘maximizing.’ Many specialist areas of dentistry have become dominated by ‘maximalists’ enthusiastically promoting their sub-discipline as being more important than any other part of dentistry and therefore in need of much more resource, status and importance in healthcare generally.
Protestations that their subjective, frequently unsubstantiated, views are always in the ‘best interests of the patient’ often provide cover for undertaking lucrative and more extensive treatments involving unnecessary complexity, or biological damage, or provide cost-ineffective, long-term consequences for many patients.
Their pursuit of supposed ‘perfection’ is often the enemy of ‘the good’ in dentistry. Promoting their often self-interested versions of the ‘highest standards’ to regulators, who appear to accept them unquestioningly, has had the perverse effect of dissuading many general dental practitioners from trying to provide decent average standard practical dentistry to solve very many patients' problems satisfactorily.
Satisficers have often been sneered at by maximalists and snootily accused of ‘bodging’ or providing suboptimal or compromised treatment even though that pragmatic philosophical approach might well provide compassionate and practically available solutions for the vast majority of dental problems.
We don't live in Utopia, and it is high time for the GDC and their hired gun ‘maximalists’ to recognize that inconvenient truth, to stop being instruments of fear and to start being a force for the good, for patients and indirectly, the profession. We will bring this challenge full circle in Part 3.