Ricketts DNJ, Tait CE, Higgins AJ Tooth preparation for post-retained restorations. Br Dent J. 2005; 198:463-471
Hunter AJ, Feiglin B, Williams JF Effects of post placement on endodontically treated teeth. J Prosthet Dent. 1989; 62:166-172
Standlee JP, Caputo AA, Holcombe JP The Dentatus screw: comparative stress analysis with other endodontic dowel designs. J Oral Rehab. 1982; 9:23-33
Torbjorner A A literature review on the prosthetic treatment of structurally compromised teeth. Int J Prosthodont. 2004; 17:369-376
Heydecke G, Peters MC The restoration of endodontically treated, single-rooted teeth with cast or direct posts and cores: a systematic review. J Prosthet Dent. 2002; 87:380-386
Ferrari M, Vichi A, Mannocci F, Mason PN Retrospective study of the clinical performance of fiber posts. Am J Dent. 2000; 13:9B-13B
Fredriksson M, Astback J, Pamenius M, Arvidson K A retrospective study of 236 patients with teeth restored by carbon fiber-reinforced epoxy resin posts. J Prosthet Dent. 1998; 80:151-157
Bolla M, Muller-Bolla M, Borg C, Lupi-Pegurier L, Laplanche O, Leforestier E Root canal posts for the restoration of root filled teeth. Cochrane Database of Systematic Reviews. 2007; (Issue 1)
Rasimick BJ, Wan J, Musikant BL, Deutsch AS A review of failure modes in teeth restored with adhesively luted endodontic dowels. J Prosthodont. 2010; 19:639-646
Rosen H Operative procedures on mutilated endodontically treated teeth. J Prosthet Dent. 1961; 11:973-986
Morgano SM, Rodrigues AHC, Sabrosa CE Restoration of endodontically treated teeth. Dent Clin N Am. 2004; 48:397-416
Sorensen JA, Engleman MJ Effect of post adaptation on fracture resistance of endodontically treated teeth. J Prosthet Dent. 1990; 64:419-424
Ng CC, Dumbrigue HB, Al-Bayat MI, Griggs JA, Wakefield CW Influence of remaining coronal tooth structure location on the fracture resistance of restored endodontically treated anterior teeth. J Prosthet Dent. 2006; 95:290-296
Milot P, Stein RS Root fracture in endodontically treated teeth related to post selection and crown design. J Prosthet Dent. 1992; 68:428-435
Jotkowitz A, Samet N Rethinking ferrule – a new approach to an old dilemma. Br Dent J. 2010; 209:25-33
Al-Wahadni A, Gutteridge DL An in vitro investigation into the effects of retained coronal dentine on the strength of a tooth restored with a cemented post and partial core restoration. Int Endod J. 2002; 35:913-918
Tan PL, Aquilino SA, Gratton DG In vitro fracture resistance of endodontically treated central incisors with varying ferrule heights and configurations. J Prosthet Dent. 2005; 93:331-336
Gargiulo A, Wentz F, Orban F Dimensions and relations of the dentogingival junction in humans. J Periodont. 1961; 32:261-267
Abbott PV Incidence of root fractures and methods used for post removal. Int Endod J. 2002; 35:63-67
Siqueira JF Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001; 34:1-10
Zuolo ML, Ferreira MOF, Gutmann JL Prognosis of periradicular surgery: a clinical prospective study. Int Endod J. 2000; 33:91-98
Ng YL, Mann V, Gulabivala K A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 1: periapical health. Int Endod J. 2011; 44:583-609
Friedman S Considerations and concepts of case selection in the management of post-treatment endodontic disease (treatment failure). Endod Topics. 2002; 1:54-78
Saunders WP, Saunders EM Coronal leakage as a cause of failure in root-canal therapy: a review. Endod Dent Traumatol. 1994; 10:105-108
Fox K, Gutteridge DL An in vitro study of coronal microleakage in root canal-treated teeth restored by the post and core technique. Int Endod J. 1997; 30:361-368
Fernandes A, Dessai G Factors affecting the fracture resistance of post-core reconstructed teeth: a review. Int J Prosthodont. 2001; 14:355-363
Smith BJ Removal of fractured posts using ultrasonic vibration: an in vivo study. J Endod. 2001; 27:632-634
Gomes APM, Kubo CH, Santos DR, Padhila RQ The influence of ultrasound on the retention of cast posts cemented with different agents. Int Endod J. 2001; 34:93-99
Fuss Z, Trope M Root perforations: classification and treatment choices based on prognostic factors. Endod Dental Traumatol. 1996; 12:255-264
Regan JD, Witherspoon DE, Foyle DM Surgical repair of root and tooth perforations. Endod Topics. 2005; 11:152-178
Torabinejad M, Chivian N Clinical applications of mineral trioxide aggregate. J Endod. 1999; 25:197-205
Parirokh M, Torabinejad M Mineral trioxide aggregate: a comprehensive literature review – Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010; 36:400-413
Main C, Mirazayan N, Shabahang S, Torabinejad M Repair of root perforations using mineral trioxide aggregate: a long-term study. J Endod. 2004; 30:80-83
Failure of a post-retained restoration can provide a challenge to the general dental practitioner (GDP) in terms of diagnosis, treatment planning and communication with the patient. The cause of failure must be identified, and a thorough assessment of the restoration, remaining tooth and its functional and aesthetic demands carried out in order to plan treatment to provide the most reliable result.
Clinical Relevance: This article discusses the assessment of failing post-retained crowns, with discussion of reasons for failure, thereby assisting the GDP in decision-making and treatment planning for such teeth.
Article
Posts provide a means of anchoring the core in endodontically treated teeth where there is inadequate coronal tooth structure to provide retention and support for the restoration.1 It was originally thought that the placement of a post strengthened the endodontically treated tooth; this is now known not to be the case: indeed, preparation for a post weakens the tooth.1,2 The use of active, threaded posts, such as the Dentatus screw, is associated with increased stresses and root fracture,3 particularly with a tapered design where there is an additional ‘wedging’ effect into the post space.
The failing post-retained crown can present a real challenge to the dental practitioner, and the decision as to whether to attempt re-restoration is not always straightforward. This article aims to discuss common reasons for failure of the post-retained crown and the factors which must be considered prior to treatment planning.
A number of post systems are available. High-level, long-term clinical data on their survival times are lacking,4 and comparison of existing studies is difficult owing to variations in patient sample, materials used and definitions of failure. A systematic review of single-rooted teeth provided with direct or cast posts found 72-month survival rates of 86.4–88.1%, with no difference between the types of post.5 Failure rates of between 0% and 10% have been reported for fibre-reinforced posts over 4 years.6,7 A 2007 Cochrane review found that there was insufficient evidence to conclude whether metal or non-metal posts are preferable.8
Failure of the post-retained crown
Modes of failure
Failure of the restoration may be discovered during clinical examination or become apparent due to de-cementation or development of signs and symptoms, and may result from one or more factors, listed in Table 1. The reasons for failure must be carefully considered in order to appreciate the likely prognosis of the tooth and treatment options.
Tooth-related
Restoration-related
Iatrogenic
Insufficient tooth tissue
Inadequate post design
Perforation of the root during initial preparation for the post
Caries
Crown or post fracture
Root fracture
Occlusal factors
Endodontic failure
Cement failure
Periodontal failure
The de-bonded restoration
When a patient presents with a de-cemented restoration, it is tempting simply to re-cement the restoration. It is vital when any restoration is deemed to have failed to determine the cause of the failure; otherwise repeated failure for the same reasons may well result. Following de-bond, the restoration and remaining tooth should be carefully inspected, and the fit and marginal adaptation assessed. The root surfaces must be examined for caries, fracture and perforations, and periodontal probing performed.
Where the lost restoration and remaining tooth are intact, there are essentially three possibilities which should be considered as the cause of failure:
Design of the post and crown;
Cement failure; and
Occlusal factors.
A post-retained crown may be suitable for recementation (in the absence of other pathologies) where:
The cement seal has only been lost for a short time period;
No root fracture or perforations are present;
The restoration is intact and of good marginal adaptation;
The post is of adequate design.
In all cases, radiographic examination is essential to identify any periapical pathology. A loose or lost post-crown provides an ideal opportunity for accessing the root filling for revision, if indicated.
Consideration must be given as to whether re-infection of the canal system has occurred. In vitro studies have shown that, if gutta-percha is exposed to the oral environment, bacteria can migrate to the apex in a matter of days and their toxins in an even shorter time.6 It could therefore be argued that even a very short-term loss of the restoration would have allowed the ingress of bacteria and necessitate re-endodontic treatment.
Although revision endodontics would be indicated in a root canal that had been exposed to the oral microflora for several days, or where gross contamination is evident, a pragmatic approach of irrigation of the post space with hypochlorite under rubber dam may be sufficient in a patient who has presented promptly without symptoms.
Residual cement must be thoroughly removed prior to re-cementation: metal posts should ideally be sandblasted. Care should also be taken to remove residual cement from the post hole. Adhesive luting cements may reduce the incidence of de-bonding,9 although may increase the difficulty of removal of post fragments in case of fracture.
Tooth-related failure
Insufficient tooth tissue
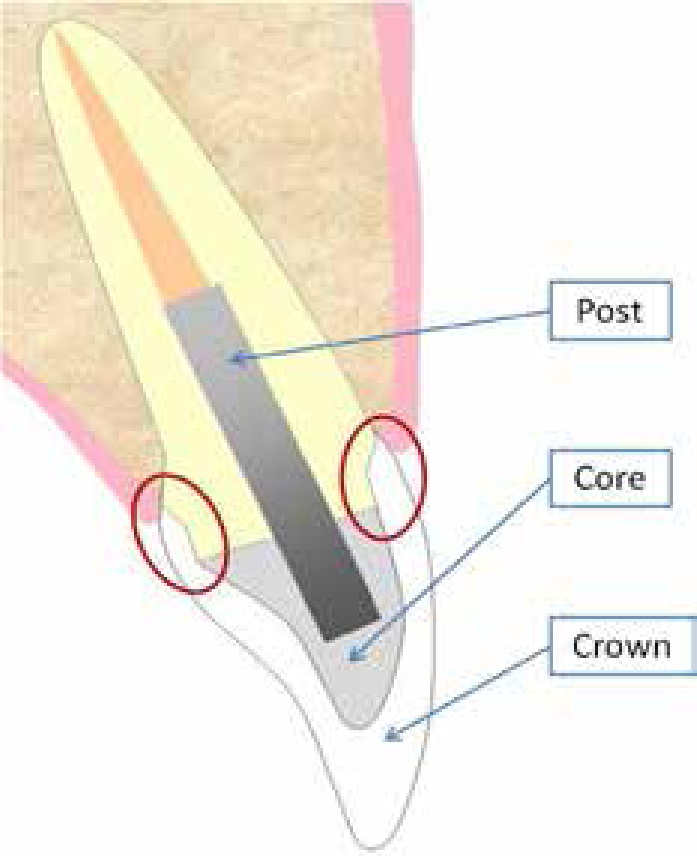
Highly influential in the success of a post-retained restoration is the amount of tooth tissue remaining supraginigvally and the availability of a ferrule.10,11,12,13,14,15,16,17 The ferrule effect was first described by Rosen in 196110 as ‘an encircling band of the cast restoration around the coronal surface of the tooth,’ which provides bracing and retention (Figure 1).
Figure 1. Ferrule (circled) created by the extension of the crown margins over the underlying tooth tissue.
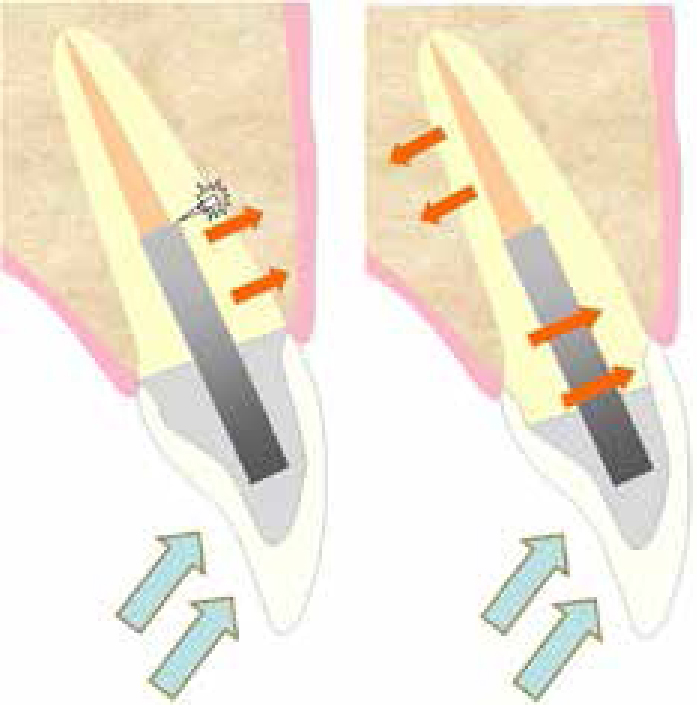
The ferrule avoids the concentration of stresses at the end of the post, thus reducing the risk of root fracture12,13 (Figure 2). A ferrule reduces the risk of de-bonding of the restoration,11 and increases the likelihood of any failure being retrievable.14
Figure 2. Occlusal forces leading to root fracture where no ferrule present, or being transmitted through the root where a ferrule exists.
At least 1 mm in height of tooth tissue above the preparation margins will improve the fracture resistance,12 although at least 2 mm is considered optimal;15 and the axial walls must be at least 1 mm thick to contribute to the ferrule.15 A partial ferrule provides better resistance to fracture than none at all.16,17
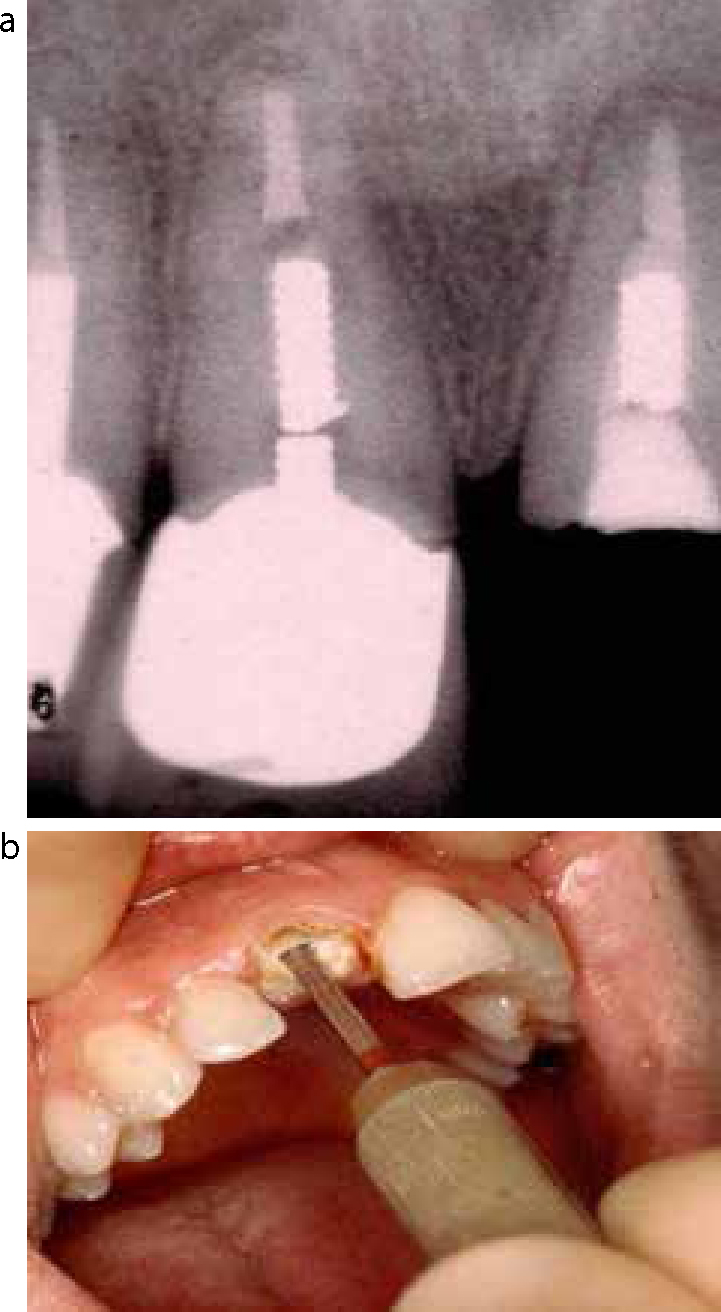
Where there is insufficient tooth tissue for a ferrule (Figure 3), extraction and prosthetic replacement has been recommended.11,15 Restoration of such teeth may involve placement of the crown margins subgingivally. These margins are difficult to record accurately in an impression and are poorly cleansable. Where the restoration margin is within 2 mm of the alveolar crest, it is said to impinge on the biologic width,18 which may lead to recession, periodontal pocket formation and alveolar crest resorption.
Figure 3.
(a) Intra-oral view of fractured UL1 with insufficient tooth tissue to provide a ferrule. (b) View showing root face UL1 with fractured post segment visible.
To avoid subgingival margin placement, it may be possible to increase the amount of supragingival tooth tissue via orthodontic extrusion and/or crown lengthening.
Caries
Owing to the radio-opacity of most crowns, caries can remain undetected radiographically until there has been considerable destruction of tooth tissue. Crown margins should be routinely checked with a probe. When caries is noted, the clinician must assess whether the full extent can be accessed and removed with the crown in situ; if there is any doubt then the crown should be removed.
Root fracture
Fracture of a root in association with a post tends to start at the coronal aspect of the root and propagate downwards and forwards towards the labial surface. Signs and symptoms of root fracture are listed in Table 2. A post-retained crown with a vertical root fracture requires extraction, whereas a superficial horizontal root fracture may be restorable.
Clinical
Radiographic
Mobility of a root fragment
Visible root fracture
Mobility of the restoration
Lateral pathology adjacent to the fracture site
Repeated loss of the restoration
Generalized widening of the periodontal ligament space
Narrow periodontal pocketing adjacent to the fracture lines
Tenderness on biting or to percussion
Endodontic failure
Endodontic failure may present via pain, swelling or sinus formation. This failure may be caused by the persistence of bacteria within the root canal system20 due to incomplete disinfection or inadequate initial endodontic treatment (Figure 4), or recontamination of the obturated root canal by bacteria from the oral cavity,21 for example due to coronal leakage. Root fracture or perforation may result in lateral, rather than apical, pathology (Figure 5): insertion of a gutta-percha point into a sinus prior to radiography may help to identify this. It should be remembered that plain radiography will provide a 2-dimensional view of a 3-dimensional situation: pathology buccal or palatal to the root may not always be visible on a radiograph.
Figure 4. Existing post-retained restoration, with absence of endodontic treatment and periapical lesion. Note that the root canal appears sclerosed: this may account for the absence of endodontic treatment.Figure 5. Post-retained crown UR4 with poorly angled post, mesial perforation and associated lateral radiolucency.
The prognosis of re-endodontic treatment depends on a number of factors including the presence and size of the periapical lesion, presence of a discharging sinus and root perforation.22 Treatment options include extraction, orthograde re-treatment and apical surgery or surgical perforation repair. Orthograde retreatment has been suggested as the treatment of choice for endodontic failures,21 and has been shown to improve the prognosis of subsequent apical surgery.23
Restoration-related failure
Inadequate post design
Length of post
This should be at least equal to the height of the clinical crown.11 An excessively short post risks loss of the cement seal and increases the risk of root fracture through creation of lateral forces within the root.1 Conversely, at least 5 mm of gutta-percha must remain apical to the post in order to maintain an adequate apical seal: less than this will be susceptible to microleakage.1,24
Width
The post should fill the root canal adequately, particularly in the apical and coronal portions. An excessively narrow post will have insufficient strength for long-term survival, whilst excessive width increases the risk of perforation and root fracture.1 A rule of thumb is that the post should not exceed one third of the root diameter at a given depth,1 although this is very difficult to assess accurately on a plain radiograph taken from the buccal aspect: the root may well be narrower mesio-distally.
Angulation
A poorly angled post may give rise to suspicion of root perforation. It is worth mentioning that the seal provided by a temporary cement and post, is poorer than that of definitive posts and therefore risks re-infection of the canal system.25 A temporary post may not be well adapted to the canal, leading to a large volume of temporary cement, which is prone to fracture or dissolution if exposed to oral fluids. The authors are aware of the use of unusual materials for temporary ‘posts’, such as sections of paperclips or wooden wedges, which cannot provide an appropriate seal (Figure 6). In the interim stage of fabricating a cast post, it may be preferable to restore the root face temporarily with a well-sealed dressing and provide an overdenture rather than attempt to use a temporary post and crown.
Figure 6. Narrow, poorly fitting temporary post UL3 resembling a section of wire such as that used in paperclips. Note under-extended, under-condensed endodontic treatment and periapical lesion.
Figure 7.
(a) Pre-operative radiograph showing fractured posts UR1and UL1, with the coronal restoration UR1 temporarily recemented. (b) Use of Masserann system to remove fractured segment of post in a different case.
Crown fracture may result from trauma, material failure or be due to occlusal factors. Where there are no other pathologies, the crown can be replaced, leaving the existing core and post in situ.
Fibre posts have a lower modulus of elasticity than metal posts: while it is suggested that this allows them to flex under load, improving force distribution and reducing the risk of root fracture, it may lead to movement of the crown with subsequent marginal leakage or post fracture.26
Removal of a fractured post depends on its accessibility and is aided greatly by the use of magnification and illumination from loupes or surgical operating microscopes. Screw posts can often be simply unscrewed with forceps.
Several post removal devices are available, eg Masserann kit (Figure 7b) (Micro-Mega, Besancon, France), which works by trephining around the post, and the Ruddle post remover (Analytic Endodontics, Orange, CA, USA), which exerts pulling force onto the post.
The use of an ultrasonic scaler is an effective way to remove metal posts27,28 by breaking the cement lute. A gutter should be cut around the post head using a fine diamond bur or diamond-coated piezoelectric scaler tip. A less aggressive scaler tip should be placed on the side of the post at full power, ensuring cooling from water irrigation. In the authors' experience it can take some 20 minutes or more to loosen the post so patience is required! After dislodgement, the post can be removed with fine forceps. Fibre posts are removed by drilling down directly through the centre of the post: special drills are available for this purpose.
Occlusal factors
Occlusal interferences, premature contacts or parafunctional habits may cause loss or fracture of the restoration. Adjustment may be possible where there are errors in the occlusal scheme; and the provision of a soft or hard splint for night-time wear may offer protection from parafunctional forces.
Cement failure
Failure of the cement itself may manifest as de-bond, caries or endodontic failure, and may be subsequent to:
Failure to introduce the cement sufficiently far down the post canal;
Inadequate moisture control with regards to saliva, gingival exudate or bleeding;
Failure to select a cement compatible with the choice of post or to follow correct cementation procedures as per manufacturer's instructions.
Iatrogenic failure: root perforation
Root perforation may be noticed at the time of preparation or later via the development of pain, swelling or sinus formation. Avoidance of perforation is obviously preferable to treatment, and can be achieved by attention to the anatomy of the root, assessment of radiographs prior to treatment and careful alignment of instruments during preparation.
The location and accessibility of the perforation are probably the most important factors in determining restorability: although perforations in the region of the alveolar crest and gingival attachment are associated with a poorer prognosis.29
Traditionally, perforations were managed surgically but recently non-surgical repair has been facilitated by the use of loupes and surgical operating microscopes30 and is advocated where possible.31
Non-surgical perforation repair has been advocated using newer calcium silicate-based restorative materials, such as mineral trioxide aggregate (MTA),32,33 eg ProRoot MTA (Dentsply Ltd, Addlestone, Surrey) and Biodentine (Septodont, Maidstone, Kent).
Good success rates following perforation repair with MTA have been described,33,34 although further clinical investigation is needed to confirm the long-term efficacy of these materials.
Treatment planning
The predictability and long term prognosis of all treatment options must be properly considered: for example, it may be that the patient would be better served by extraction and provision of a simple cantilever resin-retained bridge. The patient must be provided with sufficient information to understand fully the options and their implications. In some cases, removal of the existing crown and post may be required prior to making the final decision as to whether the tooth is restorable, for example to assess the amount of remaining tooth tissue or to identify the presence of a root fracture or perforation.
In addition to the factors discussed earlier, the clinician may consider the strategic importance of the tooth:
Is the tooth a functional, opposed unit?
Is it in the ‘aesthetic zone’?
Will prosthetic replacement be difficult? eg incisors with spacing;
Will its loss have a detrimental effect on the success of a prosthesis?
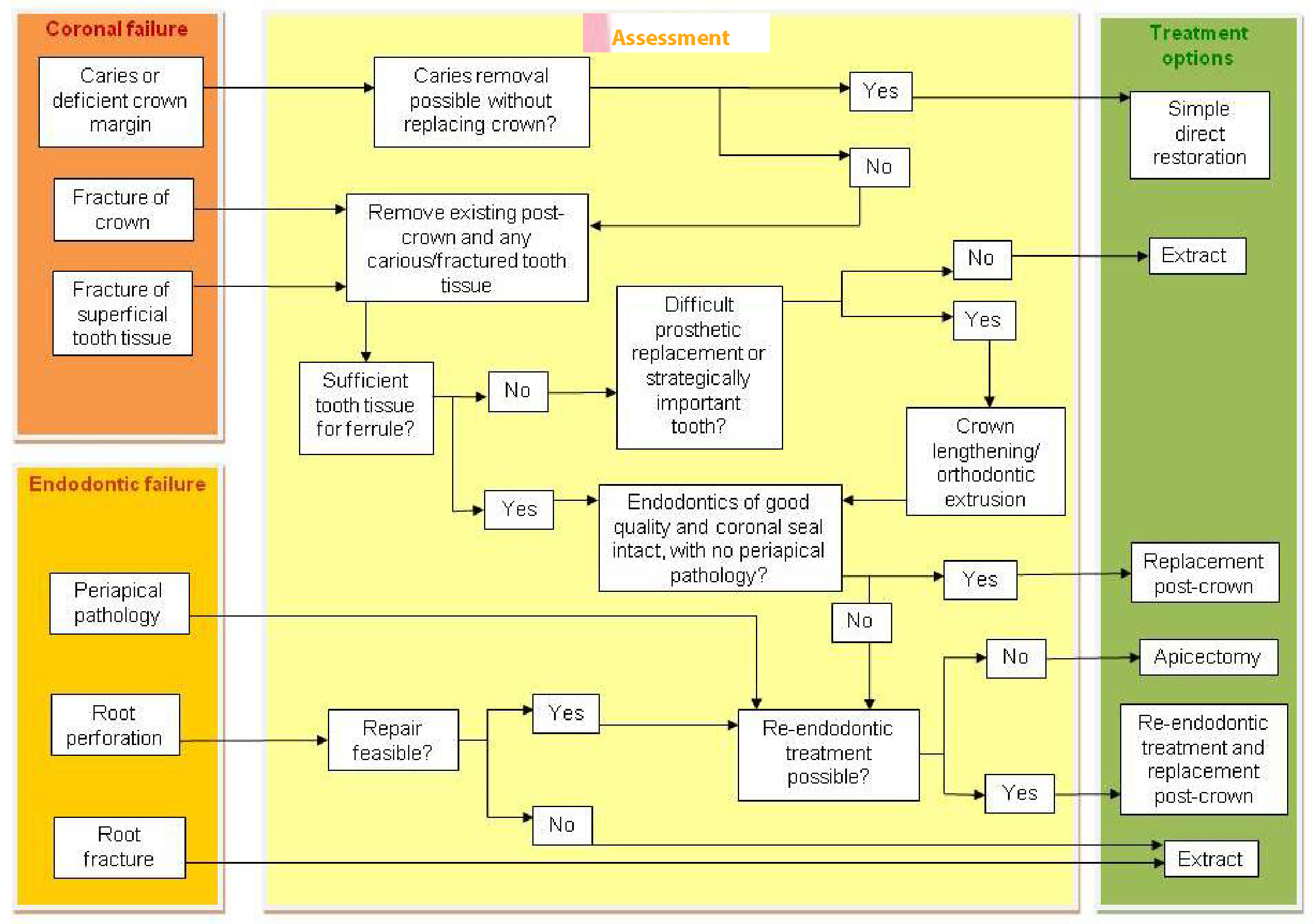
Causes of failure and potential treatment options are summarized in Figure 8. However, it is essential not to consider the tooth in isolation, but in the context of the rest of the mouth. Where the oral hygiene is inadequate or the health of the remaining dentition poor, for example, advanced treatment options are obviously not appropriate.
Figure 8. Simplified summary of assessment and potential treatment options for a failing post-retained crown.
Conclusions
When faced with a failing post-retained restoration, decision-making can be challenging. The prognosis of the tooth depends largely on the cause of failure, which must be ascertained prior to embarking upon treatment. The functional and aesthetic demands on the tooth should be considered. It is important to think logically and objectively about what will provide the most stable and reliable result, and then to explain this to the patient.
It is understandable that the patient may be upset at the prospect of losing his/her tooth. However, attempting to save an unrestorable tooth is unlikely to provide long-term satisfaction for either the dentist or the patient. Modern materials and techniques can aid in restoration of a heavily compromised tooth, but can also provide a prosthetic replacement of a very good prognosis and aesthetic result.