Leslie EJ, Marazita ML Genetics of cleft lip and cleft palate. Am J Med Genet C Semin Med Genet. 2013; 163C:246-258 https://doi.org/10.1002/ajmg.c.31381
Kawalec A, Nelke K, Pawlas K, Gerber H Risk factors involved in orofacial cleft predisposition – review. Open Med (Wars). 2015; 10:163-175 https://doi.org/10.1515/med-2015-0027
Fitzsimons KJ, Hamilton MJ, van der Meulen J Range and frequency of congenital malformations among children with cleft lip and/or palate. Cleft Palate Craniofac J. 2023; 60:917-927 https://doi.org/10.1177/10556656221089160
Sadler TW Chapter 17, 14th edn. : Lippincott Williams and Wilkins; 2019
Phippen G Articulating the issues: speech assessment and intervention in cleft lip and palate. Br Dent J. 2023; 234:912-917 https://doi.org/10.1038/s41415-023-5954-y
Sandy J, Williams A, Mildinhall S The Clinical Standards Advisory Group (CSAG) Cleft Lip and Palate Study. Br J Orthod. 1998; 25:21-30 https://doi.org/10.1093/ortho/25.1.21
Searle A, Neville P, Ryan S, Waylen A The role of the clinical nurse specialist from the perspective of parents of children born with cleft lip and/or palate in the United Kingdom: a qualitative study. Clin Nurse Spec. 2018; 32:121-128 https://doi.org/10.1097/NUR.0000000000000371
Fitzsimons KJ, Deacon SA, Copley LP School absence and achievement in children with isolated orofacial clefts. Arch Dis Child. 2021; 106:154-159 https://doi.org/10.1136/archdischild-2020-319123
Hotton M, Cropper J, Rundle J, Crawford R The role of the clinical psychologist within a cleft service. Br Dent J. 2023; 234:887-891 https://doi.org/10.1038/s41415-023-5952-0
Martin SV, Van Eeden S, Swan MC The role of primary surgery in the management of orofacial clefting. Br Dent J. 2023; 234:859-866 https://doi.org/10.1038/s41415-023-6002-7
Gillgrass T The orthodontic management of patients with cleft lip and palate: from birth to the late mixed dentition. Br Dent J. 2023; 234:873-880 https://doi.org/10.1038/s41415-023-5955-x
Bruce I, Harman N, Williamson P The management of otitis media with effusion in children with cleft palate (mOMEnt): a feasibility study and economic evaluation. Health Technol Assess. 2015; 19:1-374 https://doi.org/10.3310/hta19680
Gillgrass T The orthodontic management of patients with cleft lip and palate: from the permanent dentition and the adult returning to the service. Br Dent J. 2023; 234:892-898 https://doi.org/10.1038/s41415-023-5956-9
Chen YH, Liao YF, Chang CS Patient satisfaction and quality of life after orthodontic treatment for cleft lip and palate deformity. Clin Oral Investig. 2021; 25:5521-5529 https://doi.org/10.1007/s00784-021-03861-4
May J, Smallridge J, Collard M Challenges for dental care of the paediatric patient born with cleft lip and/or palate. Br Dent J. 2023; 234:867-871 https://doi.org/10.1038/s41415-023-5995-2
Gallagher N A general dental practitioner›s role in treating patients with a cleft lip and/or palate. Br Dent J. 2020; 228:19-21 https://doi.org/10.1038/s41415-019-1116-7
Smart C Craniofacial anomalies and the role of the dental therapist: the link between cleft lip, palate and alveolus, and periodontal disease. A literature review. BDJ Team. 2022; 9:26-29 https://doi.org/10.1038/s41407-022-0926-7
Wishney M Potential risks of orthodontic therapy: a critical review and conceptual framework. Aust Dent J. 2017; 62:86-96 https://doi.org/10.1111/adj.12486
Kuhlefelt M, Laine P, Suominen AL Smoking as a significant risk factor for infections after orthognathic surgery. J Oral Maxillofac Surg. 2012; 70:1643-1647 https://doi.org/10.1016/j.joms.2011.06.224
Consultant Cleft and Maxillofacial Surgeon, Honorary Clinical Associate Professor, University of Glasgow; Royal Hospital for Children, Glasgow, Scotland
General dental practitioners form a vital part of the multidisciplinary team for cleft lip and palate management and their role in treatment and prevention is key to ensuring successful outcomes. This article highlights key dental aspects to be aware of when treating this cohort of patients and summarizes the input of other medical specialties involved in care from birth to adulthood.
CPD/Clinical Relevance: Knowledge of the pathway for patients born with cleft lip and palate is fundamental for GDPs.
Article
Cleft lip and palate (CLP) is the most common congenital cranio-facial abnormality and therefore, it is likely that dentists will be involved in the care of these patients at some point during their career. This cohort of patients requires enhanced care from their general dental practitioners (GDP) owing to increased rates of caries and periodontitis, dental abnormalities and the need for shared multidisciplinary care. This GDP guide to cleft lip and palate provides an overview of the condition, and the framework for management as part of a multidisciplinary team within the UK.
Background
Prevalence
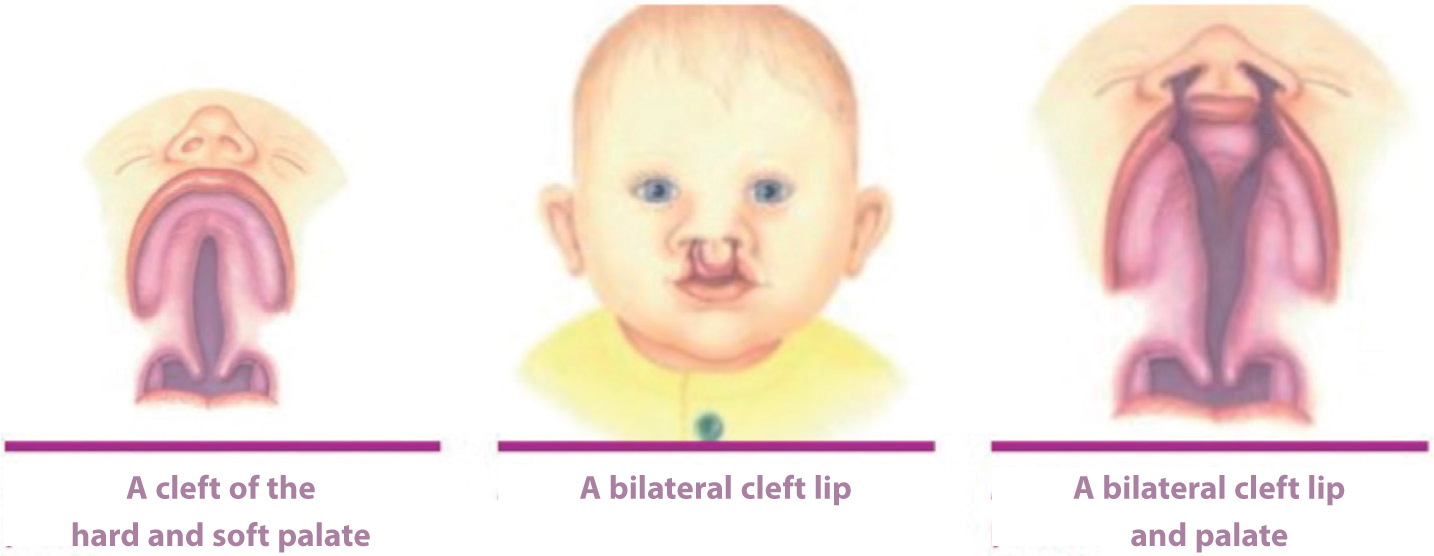
The prevalence of CLP is 1:700 live births.1 They can be unilateral or bilateral, but presence of a unilateral cleft is more common. The cleft is twice as likely to be on the left side than right and males are more affected than females.2 Based on a recent survey, 48% of cleft patients have an isolated soft palate only, 23% have a cleft lip only, 22% have a unilateral cleft lip and palate and 11% have a bilateral cleft lip and palate (BCLP) (Figure 1).2
Figure 1. Courtesy of the Cleft Lip and Palate Association (CLAPA), www.clapa.com.
Genetics/pathophysiology
The majority of orofacial clefts arise spontaneously with no family history or identifiable genetic cause or risk factor. The risk of having a child with a CLP is multifactorial and can be influenced by environmental and genetic factors. A significant factor is maternal alcohol intake, which can cause fetal-alcohol syndrome and can be associated with CLP. Additional proposed contributing factors are smoking, nutrition, obesity, maternal medication use and social deprivation.3 The risk of having a child with a cleft, where there is no family history and the cleft is not caused by a syndrome of condition, is 0.14% and this risk rises to 2–8% if the parents already have a child with a cleft. Where there is a strong family history of clefting, the risk may be as high as 50%.
CLP is known to be associated with a syndromic diagnosis in 15–30%.2 There are over 275 associated syndromes, with the most common being Van der Woude (1:34,000), Apert, Treacher Collins, trisomy 21, 22q11 deletion syndrome (formerly known as DiGeorge) and Pierre-Robin sequence.1 The recent advances in genetic sequencing have identified genomes for some of these syndromes, allowing patients and parents to have genetic counselling as part of the pathway.4
Cleft lip occurs when there is failure of fusion of the frontonasal and maxillary prominences during the 4th to 7th weeks of gestation, while a cleft palate occurs during the 6th to 10th weeks when the palatal shelves fail to fuse.5 Therefore, cleft patterns can occur as isolated palate, isolated lip or a combination of both.
Diagnosis
In the UK, cleft lip is one of the 11 rare conditions for which there is specific screening at the 20-week ultrasound scan, with 85% of children born with a cleft lip receiving an antenatal diagnosis.3 Clefts of the palate can be challenging to visualize via ultrasound, and are therefore most commonly diagnosed after birth. Examination of the palate comprises one component of the new baby check, and must be undertaken with direct visual examination of the palate, with tongue depression, to fully visualize the uvula. Once a baby has been diagnosed with a cleft lip and/or palate, the regional cleft service must be notified immediately so that a specialist nurse can arrange a visit to provide support with feeding and other aspects of care.
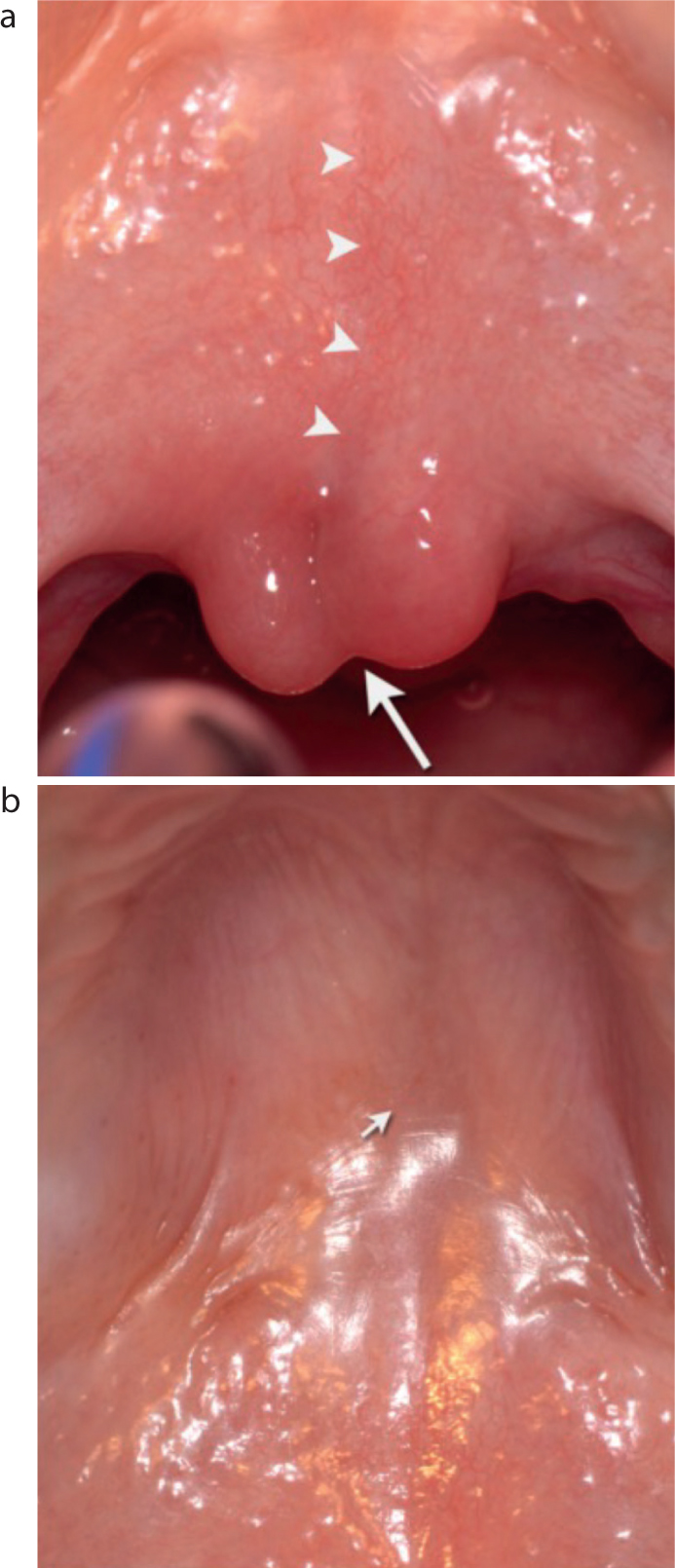
Some babies may have a mild form of clefting known as a submucous cleft palate. This is where the oral and nasal mucosa are intact, but there has been a failure of fusion of the muscle and bone, which can be of varying amounts. They are often diagnosed later because their gross anatomy can appear normal. Signs of a submucous cleft are nasal regurgitation when feeding, a bifid uvula, a palpable notch in the posterior border of the hard palate and a translucency in the midline (zona pellucida) (Figure 2).6 Where a submucous cleft palate is suspected, these children should be immediately referred to the local cleft service.
Figure 2. Submucous cleft palate. (a) Smaller arrows indicate the zona pellucida and the larger arrow show a bifid uvula. (b) Arrow indicates the position of a notch in the hard palate.
Classification
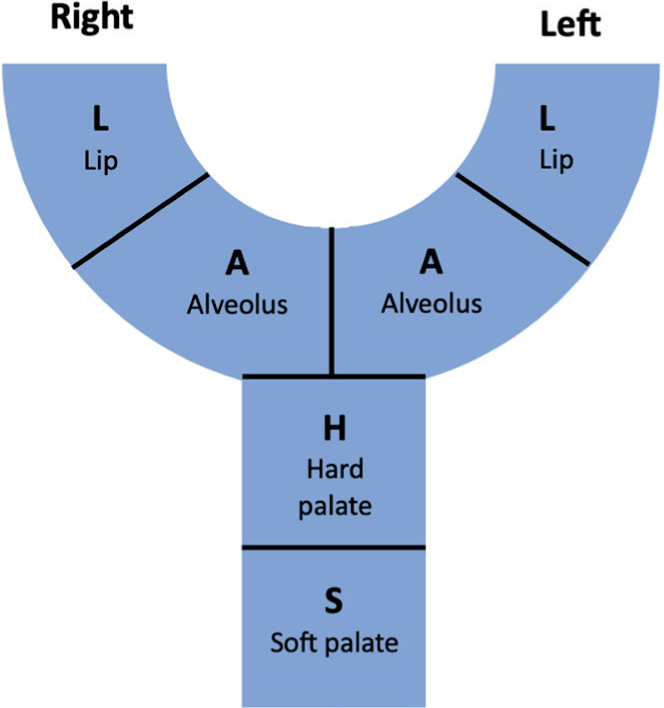
There are a number of different classification systems used to describe CLP. The two most commonly used are the Veau classification system (Table 1) and the LAHSAL method. The method to describe the pattern of clefting is from right to left, commenting on the structure of lip, alveolus, hard palate, soft palate, alveolus and lip: L-A-H-S-A-L with capital letters used to denote a complete cleft and lower case an incomplete cleft (Figure 3). For example, a patient with a complete cleft of the hard and soft palate would be allocated --HS--, a patient with an incomplete cleft of the left lip and alveolus would be allocated ----al, a patient with a right complete cleft lip and alveolus LAHS--, and a patient with an incomplete bilateral cleft lip, but complete cleft of the alveolus and palate would be allocated lAHSAl. An example of how both classifications are used is shown in Figure 4.
Type
Description
1
Isolated cleft of the soft palate
2
Cleft of the hard and soft palate
3
Unilateral cleft of the lip and palate
4
Bilateral cleft of the lip and palate
Figure 3. LASHAL classification.Figure 4. An isolated, complete cleft of the soft palate. LASHAL: ---S-- or Veau 1.
Multidisciplinary team approach (MDT)
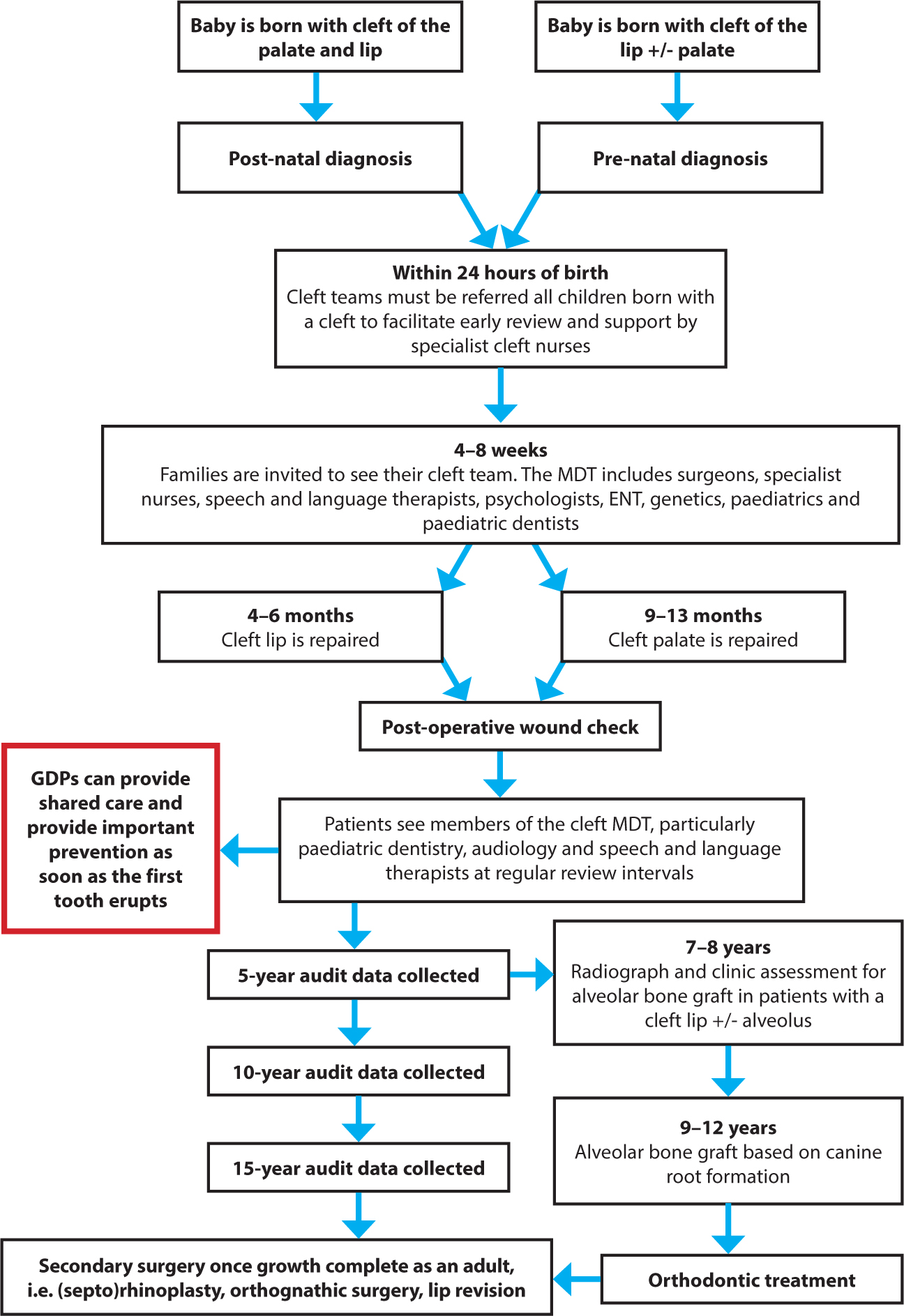
The Clinical Standard Advisory Group (CSAG) (1998)7 for cleft was a national study that reviewed the pathways and outcomes in the UK. It made a series of recommendations and led to centralization of cleft services. At the time of writing, there are 12 designated cleft centres in the UK, designed to bring together a wide range of healthcare disciplines to coordinate holistic care for patients with CLP. They are set up in a hub and spoke arrangement. Larger hospitals that can provide this tertiary level of care act as the hub, with the GDP being a key aspect of the spoke services. Families are invited to a new baby clinic in the hub in the first few weeks so that they can be assessed, meet their cleft team and have a management plan made. Regular reviews are undertaken with audit records taken by different members of the MDT at the key ages of 5, 10 and 15 years (Figure 5).
Figure 5. Cleft pathway in the UK from birth to adulthood.
The cleft nurse specialist
The cleft nurse specialists are usually the first member of the cleft team who parents will meet, and are a highly valued point of contact. A survey undertaken in 2018 showed them to be a trusted mediator between families and the wider cleft team.8 These nurses have a wealth of experience and monitor the growth and development of babies pre- and post-surgery. Babies with CLP can have challenges with breast and bottle feeding because they cannot create a negative pressure inside the oral cavity, and can struggle with coordination. Cleft nurses offer support to parents with recommendations of techniques and modified bottles that improve feeding to ensures babies thrive, allowing them to have surgery at optimum times.
Psychology
Patients and their families are seen regularly by clinical psychologists who aim to support them to adjust to their diagnosis, and can assist by advocating in decision-making processes. Psychologist support is offered from when a diagnosis is made, right through to when the patient has reached adulthood and is accessing treatment. Psychologists can help manage parental emotions and expectations in regard to the long-term implications of cleft and surgery. When older, they provide invaluable input to children with CLP, who can have difficulties with social involvement and bullying. Children with CLP can also lack confidence in speaking if their peers struggle to understand them, leading to frustration and withdrawal as well as low self-esteem. This can lead to disruption in their school life with increased absence,9 and can potentially influence behavioural issues in their adolescent and adult lives.10 The Strength and Difficulties questionnaire is used as a screening tool to assess patients' and parents' mental health. Based on these assessments, psychologists can offer cognitive behavioural therapy for appearance-related anxiety.
When planning any treatment for children and adults with a cleft, psychologists are an invaluable part of the team who can help to address any procedure-related concerns and prepare patients for surgeries.
Cleft surgery
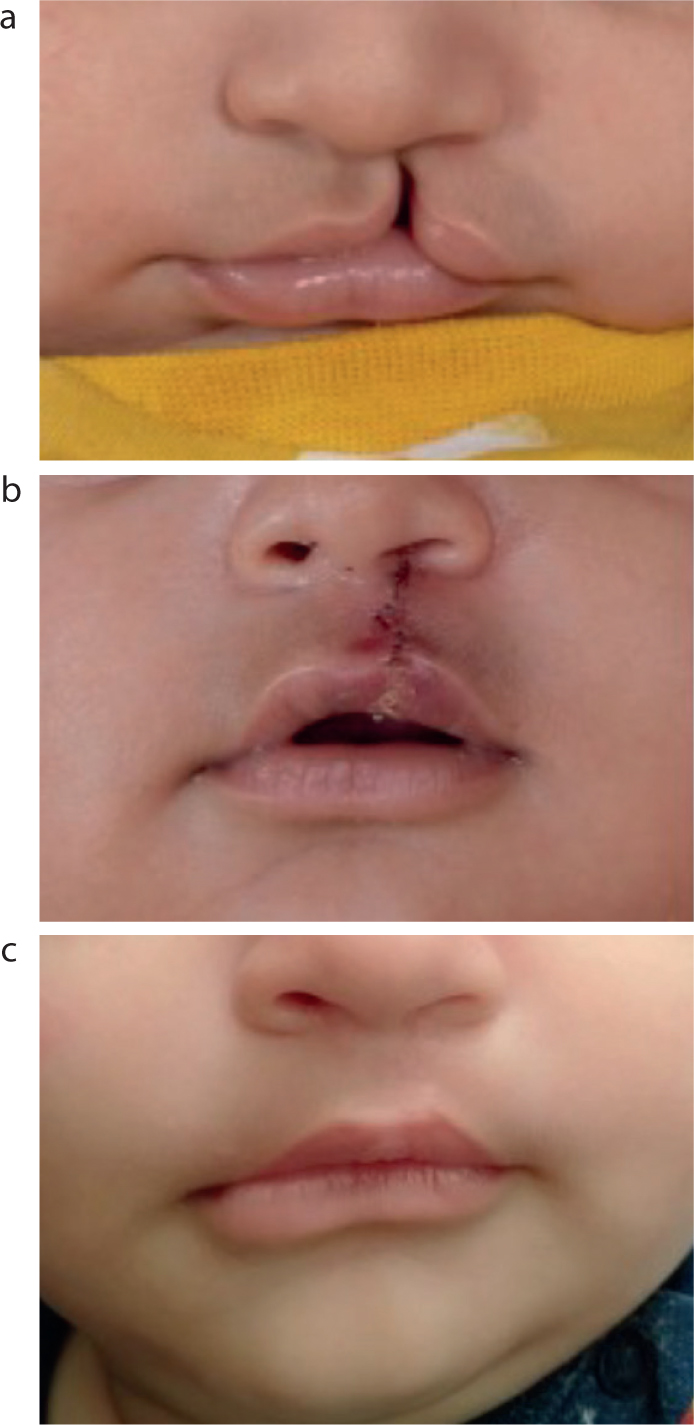
In the UK, timings of surgical repair are nationally set with lip repair aiming to be completed by the age of 6 months, and palate repair by the age of 13 months. Numerous different surgical techniques are described and used to repair the cleft lip (technical descriptions are outwith the scope of this article), but all aim to restore normal appearance and function of the upper lip with reconstruction of the underlying orbicularis oris muscle (Figure 6). Often, hard palate closure with a vomer flap is undertaken at the same time. As part of the lip repair, the nasal deformity is often improved too, although revisional surgery for nasal shape may be required at a later stage. Repair of the cleft palate involves a two-layer repair of the nasal and oral mucosas with reconstruction of the levator veli palatini muscular sling to allow closure of the soft palate against the nasopharynx. This allows for normal speech production and feeding,11 and is most commonly performed with an intravelar veloplasty (Sommerlad repair) or a double opposing Z-plasty (Furlow repair).
Figure 6. A patient with left-sided cleft lip. (a) Pre-operative; (b) immediately post-operative; and (c) on review of healing, with a good surgical outcome and minimal scarring of the lip.
Alveolar bone graft (ABG) surgery is a procedure carried out for clefts affecting the alveolus when there is an insufficient volume of bone to allow the eruption of the permanent canine. This infills the defect and allows the tooth to erupt, remodelling the bone as it does so. Radiographs (OPT, upper standard occlusal) are taken to assess the timing of ABG, as well as confirming the presence of a cleft. Surgery timing is based on the root development of the canine and incisor and should be performed prior to eruption of the cleft-side canine. This is closely monitored by the cleft orthodontist, but generally occurs between the ages of 9 and 11 years.12
Patients with cleft lip and palate are at risk of maxillary hypoplasia, which is due to a combination of underlying growth abnormalities and scarring. Therefore, some patients may seek to have orthognathic surgery to correct a Class III occlusion, which most commonly requires a Le Fort I osteotomy. However, owing to the instability of the pre-maxilla and scar tissue, osteotomies in these patients can be challenging. Adult patients also require a psychological assessment to ensure such surgery outcomes will meet realistic patient expectations.
Once the patient has reached adulthood, other surgeries can be undertaken to correct aesthetic and functional concerns. Procedures typically undertaken are open rhinoplasty to address aesthetic and function concerns as well as lip scar revisions.
Speech and language therapy (SALT)
The speech and language therapist is a key member of the MDT because children with a cleft palate can have challenges related to speech sound articulation or air escape down the nose owing to velopharyngeal insuffiency (VPI). It is reported that 50% of children with a cleft palate will require therapy.13 Typically, speech is first assessed at the age of 18 months, and assessment is repeated at regular intervals throughout childhood. The Great Ormond Street Speech Assessment (GOS.SP.ASS) is the standard used in the UK to assess speech sound production and quality. Videofluoroscopy and nasendoscopy can be used where children have evidence of nasal air escape owing to an underlying anatomical problem with the closure of the soft palate against the posterior pharyngeal wall. This can present as hypernasality, nasal emission, nasal turbulence, grimace and compensatory articulatory errors.
Otolaryngology (ENT)
Another consequence of abnormal palate muscle insertion is that the eustachian tube that links the middle ear and the nasopharynx is affected. A new-born audiology test is completed shortly after birth and is done so every year until school age. Conductive hearing loss is a condition that is increased in patients with CLP, with otitis media with effusion (glue ear) being the most common type. ENT surgeons can treat the build-up of fluid in the middle ear by inserting small tympanostomy tubes known as ‘grommets’. These allow drainage, and are expelled spontaneously after 6–12 months. These are no longer inserted prophylactically at the time of palate repair as was done in the past. In some cases, patients may benefit from the use of hearing aids in addition to, or instead of, insertion of grommets.13
Dental specialties
Orthodontics
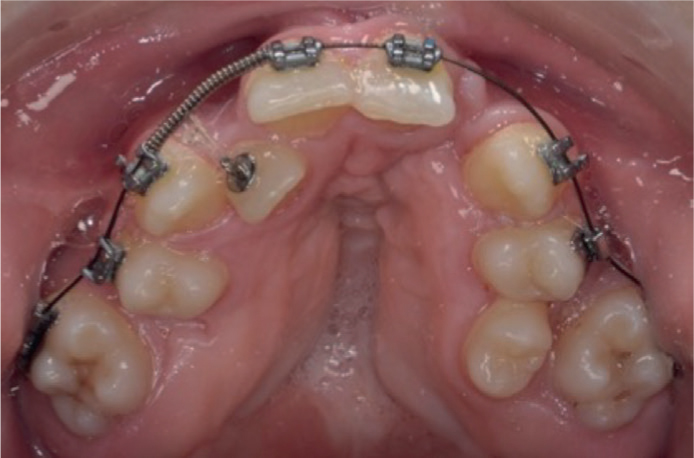
Cleft is recognized as a dental component (5p) in the Index of Orthodontic Treatment Need (IOTN) and therefore, patients are entitled to orthodontic treatment in the absence of contraindications. Treatment aims to correct the maxillary alveolus because there are issues with arch form, and alignment and crowding (Figure 7). Owing to the hypoplastic nature of the maxilla, cleft patients commonly have a Class III skeletal pattern. Treatment may involve transverse maxillary expansion pre-ABG with quad/tri-helix appliances, and for patients with BCLP, the pre-maxilla can be mobile and so pre-surgical orthodontics can help with stability and correction of the centre-line shift. Post-ABG orthodontics aims to correct crossbites, incisor rotation and inclination and other anomalies. However, the incidence of apical root resorption around the cleft site is high, and so careful records and monitoring are required before commencement of treatment.12 Unfortunately, on completion of orthodontic treatment, the rate of relapse is high and so bonded retainers are preferred to ensure long-term retention.14
Figure 7. Intra-oral photograph of a patient in fixed appliance phase with severe maxillary arch crowding.
Orthodontic treatment plans can be extremely lengthy (3.3–8.5 years) and patients require numerous appointments for monitoring and adjustments.12 This requires high motivation from both patients, who are absent from school, and dedication from parents/carers to bring their children to appointments. Orthodontic treatment therefore poses a high burden of care for these patients, but the aesthetic outcomes gained from this have been shown to improve their oral health-related quality of life.15
Paediatric dentistry
Paediatric dentists are vital in the treatment of young, complex patients who may also require treatment adjuvants, such as inhalation sedation or general anaesthetic. This is especially important when a proportion of this group have other complex medical considerations, such as cardiac or respiratory, and require tertiary level care. As with any child, it is important to maintain primary dentitions to prevent early loss, which can create crowding, complicating future treatment. Paediatric dentists use their expertise by using a combination of techniques in their armamentarium, including pre-formed metal crowns (Hall technique), silver-diamine fluoride (SDF) and resin-based restorations, such as ICON and composite.16
Restorative dentistry
Restorative dentists are involved with rehabilitation of the dentition as the patient progresses through their teenage years into adulthood.17 Minimally invasive procedures are advocated at this point to delay the restorative cycle in the future by using reversible methods. Tooth replacement options such as removable appliances with pontics and resin-bonded bridges are commonly used to maintain space and improve aesthetics in the growing patient.17 Dental implants can also be considered when the patient reaches adulthood if there is sufficient bone available and no contra-indications. Cone beam CT scans can be useful in planning for this procedure as it provides a three-dimensional view of the area and allow for 3D printed cutting guides.
The role of a GDP
Patients with CLP may be seeing several other health professionals at a time, but the role of the GDP is paramount in ensuring patients remain in optimal dental health. In recent years, after the COVID pandemic, a large proportion of CLP patients (46%) had difficulty accessing primary dental care.16,18 Cleft patients should be identified at the point of registration and GDPs should ensure they familiarize themselves with the stage of the pathway that the patient has reached. Communication with the patient's ‘hub’ can then help to determine whether there is any outstanding treatment required that can be completed in primary care.
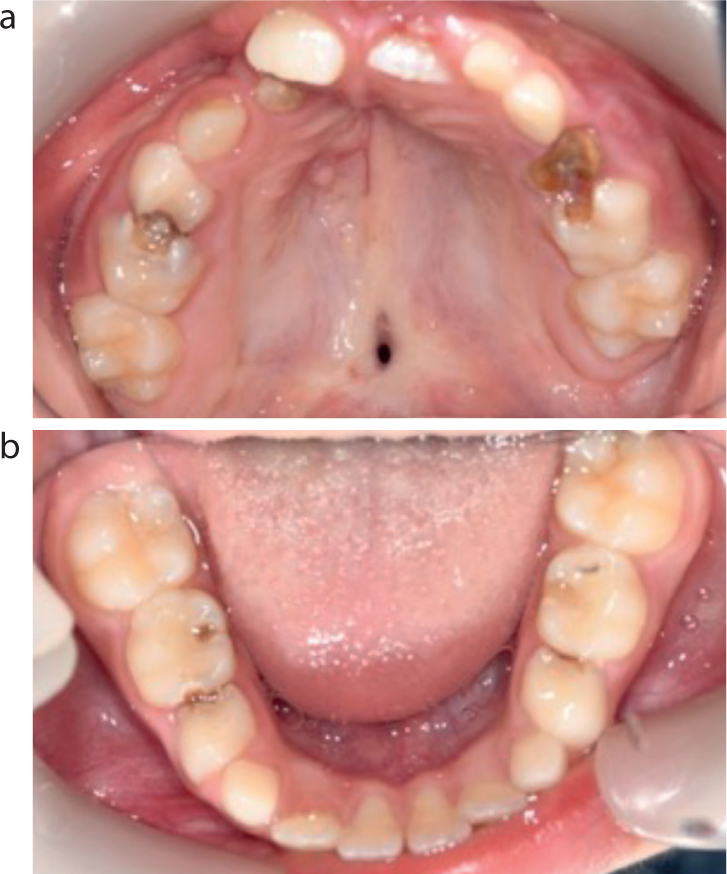
Children with CLP have an increased risk of caries compared to the general population, with 2022 figures showing 65% of these children having caries compared to 52% in the general population (Figure 8).16 This risk increase is due to several factors involving poor oral hygiene, cariogenic diet, alveolar and tooth deformity, orthodontic appliance wear, saliva buffering capacity and mouth breathing.16 Socio-economic factors are also a risk, with social deprivation a risk for both cleft and caries. It is also worth noting that these patients have been subject to numerous medical interventions and surgeries and as such, can develop dental phobia or treatment fatigue. This results in poor attendance with GDPs and other professionals, which can negatively impact their care.
Figure 8. Intra-oral (a) maxillary and (b) mandibular occlusal views of a paediatric cleft patient with caries in all deciduous molars, and a residual palatal fistula.
From birth to age 5 (primary dentition)
A dental check is encouraged when the first deciduous teeth erupt, or when the child turns 1 year of age, as recommended the national programme ‘Dental Check by 1’.19 Babies with CLP will often have their first surgeries in the first year of life, and so dental reviews are beneficial to instil positive attitudes towards dental visits and acclimatize patients to the dental surgery. GDPs can ensure parents and carers are well supported in providing dental care to the child, and offer dietary advice from the outset. It is recommended that free sugars contribute to less than 5% of the total energy from diet20 and so advice should aim to restrict cariogenic food and drink (Table 2).
Sugary soft drinks and juices (including dilute cordial)
Confectionary, cakes and biscuits
Breakfast cereals
Dried fruit (e.g. raisins)
Canned fruit in syrup
Fruit juice/smoothies exceeding 150 ml
Jams, preserves, honey
Ice cream and ice lollies
Enhanced preventive measures for these high-risk patients should be implemented as per the evidence-based guidance, ‘Delivering Better Oral Health’.20 This includes fluoride varnish applications at least twice a year, fissure sealants on the primary molars, in-depth oral hygiene instruction and 3-monthly recalls.20 Oral hygiene levels and caries-free dentitions are particularly important for ensuring good outcomes for surgery.12,16 If caries is encountered, it should be treated by the same techniques used in non-cleft patients. If adjuncts, such as inhalation sedation or general anaesthetic, are required, an urgent referral to paediatric dentistry should be undertaken promptly to ensure an optimized surgical environment is maintained.
Ages 6–12 years (mixed dentition)
Patients with CLP have been shown to have higher plaque levels, particularly in the anterior maxilla region (Figure 9).21 This may be attributed to fear of brushing the cleft site, with periodontal bleeding, difficulty with access and mobility of teeth in the pre-maxilla in patients with a bilateral cleft lip and palate. As the patient progresses into the mixed dentition phase, it is important that the first permanent molars are sealed when fully erupted. In addition, it is paramount that a simplified Basic Periodontal Examination (BPE) is performed on children aged 7–12 years, and a standard BPE on those over 12 years of age. This should be carried out with a WHO 621 probe at each routine examination to screen for periodontal issues, along with the appropriate radiographs. Inflammation is usually resolvable with detailed oral hygiene instruction, with stress given to obstructing the biofilm that builds at the gingival margins. However, any unresponsive areas, despite the patient's best efforts, should be acted upon with a referral to local specialist services for investigation.22
Figure 9. Poor oral hygiene with calculus, soft plaque deposits with gingival inflammation around the cleft site and a Class III incisor relationship.
Dental abnormalities are common in patients with CLP for which GDPs should be mindful when monitoring dental development. Hypodontia is the most common, as clefts occur where the lateral incisor would usually develop, and so are absent or diminutive in 40% of patients.16 Other abnormalities include tooth quantity, with supernumerary and supplemental teeth in the pre-maxilla, which are usually the last tooth in the series (2s, 5s, 8s). These teeth should be carefully assessed with regard to their placement in the arch and the need for removal. Defects in tooth structure are also a common finding, with the enamel of patients with CLP being hypoplastic (quantitative defect) or hypomineralized (qualitative defect). This can be in either deciduous or permanent teeth, and can result in post-eruptive breakdown. Often, these teeth require restorations to maintain the tooth for as long as possible, providing they are asymptomatic.
Age 12 and beyond (permanent dentition)
Young adults with CLP are often engaged with fixed orthodontic treatment that carries additional risks in itself. These include oral hygiene-specific risks, such as demineralization and periodontal inflammation, but also root resorption, temporomandibular dysfunction, de-vitalization of pulp, and relapse.23 During this time, GDPs can support treatment by educating patients further, and recommending adjuncts to toothbrushing such as daily 0.05% fluoride mouth rinses at a different time to brushing, and the use of interdental aids.20 Adult patients require preventive advice that includes smoking cessation in order to maintain periodontal and soft tissue health. This is especially important for those patients undertaking orthognathic surgery because smoking can increase the risk of post-operative infection.24
During regular dental assessments, GDPs should assess whether adult patients with CLP have further concerns that require referral back to their cleft hub. As described previously, adult patients can access care throughout their lives, and can benefit from input from the wider team, especially restorative specialists for rehabilitation.
Conclusion
GDPs require a good understanding of CLP and the pathway that patients follow in order to appreciate the challenges specific to this group of patients. Despite the patient being seen by numerous medical professionals, it is paramount that GDPs maintain their shared-care role with the CLP team, and have the confidence to provide simple, yet important, prevention and basic treatment where required.