Doshi M, Shehabi Z, Liu S, Geddis-Regan A General anaesthesia in special care dentistry. Part 1: justifying and planning the use of general anaesthesia. Dent Update. 2024; 51:780-785
King TA, Duffy J Peri-operative care of elective adult surgical patients with a learning disability. Anaesthesia. 2022; 77:674-683 https://doi.org/10.1111/anae.15691
Geddis-Regan AR, Gray D, Buckingham S The use of general anaesthesia in special care dentistry: a clinical guideline from the British Society for Disability and Oral Health. Spec Care Dentist. 2022; 42:(S1)3-32 https://doi.org/10.1111/scd.12652
Cook TM, Lee G, Nolan JP The ProSeal laryngeal mask airway: a review of the literature. Can J Anaesth. 2005; 52:739-760 https://doi.org/10.1007/BF03016565
Goma A, Pons I, Moret ML, Guitart J Satisfaction and complications comparing flexible rein-forced laryngeal mask airways (FRLMA) with ETT in surgery of the face in adults. Eur J Anaesthesiol. 2011; 28
Anderson CR, Premakumar Y, Navaratnam AV The use of throat packs in ear, nose and throat, oral and dental surgery: a systematic review. Rhinology. 2020; 58:306-313 https://doi.org/10.4193/Rhin19.308
Campbell M, Pierce JMT Atmospheric science, anaesthesia, and the environment. BJA Educ. 2015; 15:173-179
Mac Giolla Phadraig C, Fennell-Wells A, Geddis-Regan AR, Wilson K Supporting people and their behaviour in the dental setting as sustainably as reasonably achievable. In: Duane B (ed). Cham: Springer International Publishing; 2022
Bocskai T, Kovács M, Szakács Z Is the bispectral index monitoring protective against postoperative cognitive decline? A systematic review with meta-analysis. PLoS One. 2020; 15 https://doi.org/10.1371/journal.pone.0229018
Ling L, Yang TX, Lee SWK Effect of anaesthesia depth on postoperative delirium and postoperative cognitive dysfunction in high-risk patients: a systematic review and meta-analysis. Cureus. 2022; 14 https://doi.org/10.7759/cureus.30120
Klein AA, Meek T, Allcock E Recommendations for standards of monitoring during anaesthesia and recovery 2021: guideline from the Association of Anaesthetists. Anaesthesia. 2021; 76:1212-1223 https://doi.org/10.1111/anae.15501
Gan TJ, Belani KG, Bergese S Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth Analg. 2020; 131:411-448 https://doi.org/10.1213/ANE.0000000000004833
Cook TM, Woodall N, Frerk C Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth. 2011; 106:617-631 https://doi.org/10.1093/bja/aer058
Immediate post-anaesthesia recovery 2013: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2013; 68:288-297 https://doi.org/10.1111/anae.12146
General anaesthesia in special care dentistry. Part 2: delivering dental care Zahra Shehabi Mili Doshi Sophie Liu Andrew Geddis-Regan Dental Update 2025 52:1, 35-40.
Authors
ZahraShehabi
BDS, MFDS, MSc, MSpecCareDent
BDS, MFDS, MSc (Sed Spec Care), MSCD, MSc (Health Management), Consultant in Special Care Dentistry, Bart's Health NHS Trust
BSc (Hons), BChD, DSCD RCS Eng, MSCD RCS Ed, PhD, Consultant in Special Care Dentistry, University Dental Hospital of Manchester; Honorary Senior Lecturer in Dentistry, University of Manchester
The use of general anaesthesia (GA) in dental care needs to be cautiously justified and considered. Preparation for GA can take a considerable degree of planning, especially as the increased prevalence of coexisting systemic diseases in people with disabilities can increase the risks and challenges of care delivery. When a GA has been deemed appropriate and consent has been gained for relevant treatment, providing treatment this way requires further considerations related to anaesthesia and dental care. There is also a recovery period after GA, and there can be additional post-operative considerations. This paper details the ‘how’ of delivering care under GA, including the dental team's role in supporting an anaesthetic team, the delivery of dental procedures, and the logistics of post-GA care.
CPD/Clinical Relevance: The use of general anaesthesia for patients with disabilities and complex needs requires careful consideration and planning.
Article
As detailed in Part 1 of this series, a substantial amount of planning and preparation goes into delivering dental care under general anaesthesia (GA).1 Many of the aspects described below are considered before the day of treatment under GA. However, they are discussed herein as they often present challenges, despite meticulous planning, when care comes to be delivered. Many aspects of this article relate to those individuals with the most significant behavioural or medical requirements for general anaesthesia, such as those with severe learning disabilities, autism and mental health conditions. The nature of dental treatment planning and treatment delivery is detailed briefly, but is not the primary focus of this article.
Pre-anaesthesia care
Planning the timing of care
A range of reasonable adjustments to support patients with additional needs was discussed in Part 1 of this series.1 It is essential that all staff involved in the GA care pathway, including admitting and recovery staff, are aware that the patients have additional needs. The Health and Care Act 2022 introduced a requirement that staff receive learning disability and autism training appropriate to their role, for example, the Oliver McGowan Mandatory Training on Learning Disability and Autism.2
Appropriate adjustments may also reduce the need for, or extent of, pre-medication, clinical holding or rescheduling treatment.3 This can include using photographs of patient journeys and pre-admission visits for familiarization. Certain patients may benefit from an isolated side room instead of a general ward admission, and they should be permitted to bring distractions (e.g. books, tablets, headphones), wear their own clothes rather than a patient gown, and any other key elements of their routine into the theatre environment where possible. Pre-surgery policies may need to be adjusted, for example, the need for more than one carer to accompany them.
A team brief must occur with the anaesthetic and surgical team at the start of each session.4,5 The dentists would typically take the lead and check that the anaesthetic and dental teams have reviewed the patients. The team brief provides an opportunity for discussions about pre-medication, the type of airway preferred for the planned procedure, clinical holding, multidisciplinary care if planned, recovery and discharge and allows any concerns to be raised.
Ideally, patients with special care needs should be prioritized for surgery early in the day to reduce disruption to their usual routine, prolonged starvation, and interruption to medication schedules. A carer or relative known to the patient should accompany the patient. Provisions should be made for them to be present until anaesthetic induction and soon after emergence in the post-operative recovery room.
Pre-medication and pre-operative anxiolysis
Non-pharmacological methods of anxiolysis are preferable. Thorough explanation, adequate preparation and allowing family members to be present during the pre-operative stages can be very effective. Listening to families/carers about what has worked for the patient and what has not worked is important. For patients who present with challenging behaviours leaving their homes or entering the hospital premises, a prescription of oral lorazepam, diazepam, or promethazine may be helpful. It is generally necessary to discuss with the general medical practitioner or other relevant medical professionals to prescribe this pre-operatively. In some situations, more substantial pre-medication with additional drugs may be needed before hospital attendance or entering the hospital building. Although this introduces more risk than non-pharmacological approaches or in-hospital pre-medication, it can be the only feasible way to support certain individuals entering hospital settings.
Several methods may help to facilitate a smooth induction, especially in those with special care needs or a high level of anxiety. Once in the hospital, local anaesthetic cream (e.g. EMLA/Ametop) can be applied to the skin to help with cannulation. Depending on the preparation, the cream must be applied for 30–60 minutes for the desired effect. Midazolam can be given orally, buccally or nasally on the ward or in the theatre to produce anxiolysis and sedation. Nasal midazolam will, in general take 7–10 minutes to reach peak effect, whereas oral midazolam can take 20–40 minutes for the desired effect. The anaesthetist will determine the dose of the pre-medication. Alternatives are alpha-2-agonists (oral clonidine, intranasal dexmedetomidine) and ketamine (oral/intramuscular (IM)) or a mixture. Ketamine, however, can be painful on injection and may exacerbate already challenging behaviour until it takes effect.
Clinical holding
Clinical holding may be needed for safe cannulation or gas induction in the patient's best interest, even if pre-medication has been given.6 Clinical holding should only be undertaken by trained staff and discussed with the patient/carers as part of the assessment and reconfirmed on the day of treatment and documented.6 Clinical holding may take the form of stabilizing the arm for cannulation to prevent reflex withdrawal and consequent unnecessary pain, distress or injury to the patient, staff or carer. Clinical holding can be unpredictable and emotional for patients/carers and staff, and this should be discussed as part of the theatre debrief to reflect on positive and negative aspects for future learning.
Administration of general anaesthesia
Induction of anaesthesia
The chosen anaesthetic technique depends on patient factors, surgical factors and the anaesthetist's preference. Aspects and variations of the anaesthetic process are detailed below. Anaesthesia can be induced using intravenous (IV) agents or with an inhalational gas method.7 Propofol is the most common intravenous induction agent when IV access and induction are feasible. This induces a rapid onset of anaesthesia and apnoea. Where behavioural challenges limit the suitability of conscious sedation or oral pre-medication, an IV induction may also not be feasible. A gas induction has a much slower onset of anaesthesia, where spontaneous respiration is usually maintained. It can be useful in patients who may not tolerate an intravenous cannula while awake, such as those with severe learning disabilities or needle phobia. Once the patient has been anaesthetized, loss of muscle tone causes the airway to collapse, resulting in airway obstruction. At this point, chin lift, jaw thrust and head-tilt airway manoeuvres are employed to open the airway and assisted ventilation commences using a facemask.
Choice of airway
The decision regarding the airway should be made after a discussion between the dentist and anaesthetist.8 This should be based on the need for surgical access, risk of airway dislodgement and patient factors. Some of the most common airway devices are listed below.
Supraglottic airways
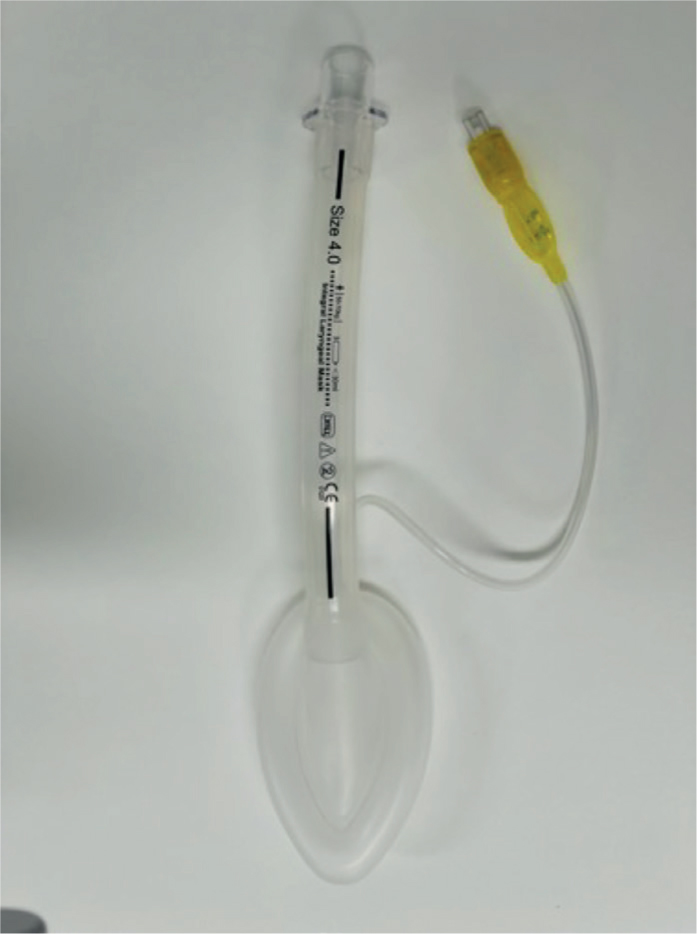
The laryngeal mask (LMA) can be used when a definitive airway is not required (Figure 1). An LMA allows for spontaneous or positive pressure ventilation. Paralysis is not necessary, and tolerance of an LMA requires a lighter plane of anaesthesia than an endotracheal tube, resulting in less haemodynamic disturbance.9 As many recovery nurses are trained to remove LMAs, list turnover time can be decreased as the anaesthetist does not need to extubate the patient before transferring them out of the operating theatre to the recovery room. Other benefits of LMAs include less airway trauma on insertion, decreased incidence of sore throat, less risk of airway irritation, less coughing and reduced risk of post-operative respiratory infection.10 The LMA sits in the hypopharynx with a large cuff above the vocal cords, reducing the risk of blood and debris falling into the larynx. Depending on the risk of oral debris and surgical preference, a throat pack may or may not be used. As LMAs are not a definitive airway and the cuff may leak or dislodge, there is a risk of aspiration, so they should be used with caution in patients with gastro-oesophageal reflux disease, high body mass index or at risk of vomiting. For comprehensive dental care under GA, intra-oral radiography is difficult because access can be challenging. Thorough suctioning is required to immediately remove foreign bodies, fluids from secretions (e.g. blood, saliva) and water used for cooling instruments (e.g. fast handpieces and ultrasonic scalers) prior to throat pack removal to avoid aspiration via breaches in the LMA cuff. Alternative intubation methods (endotracheal or nasal tubes) therefore offer more secure airways.
Figure 1. A laryngeal mask.
Endotracheal tubes
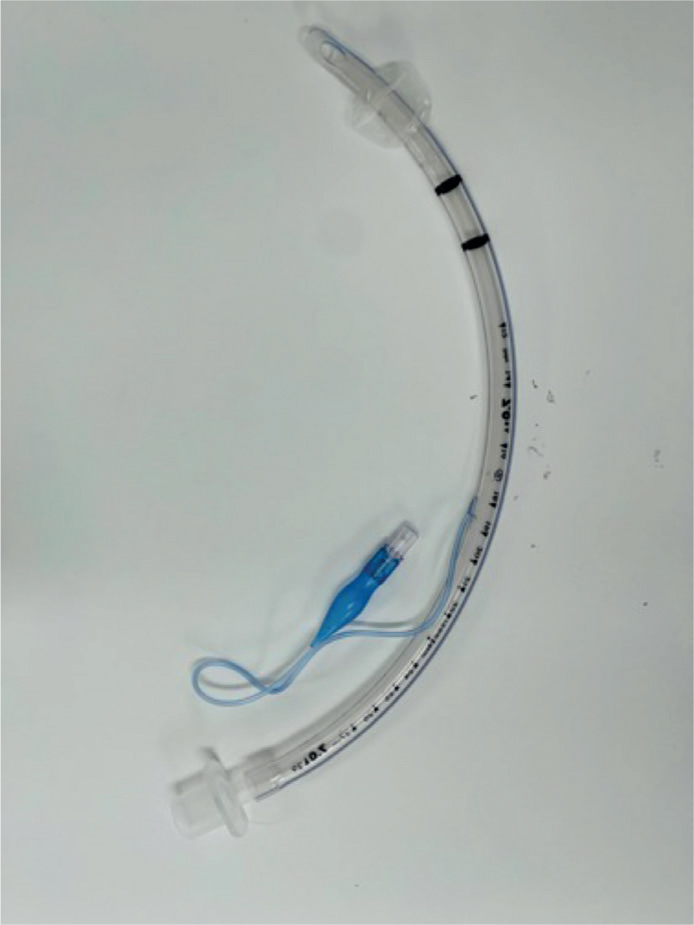
Oral or nasal endotracheal tubes provide a definitive airway with an inflatable cuff that lies below the vocal cords providing a reliable seal. The cuff offers protection from aspiration of debris from the oropharynx into the trachea. A throat pack is usually placed to reduce the amount of blood and debris above the cuff that could fall into the airway once the cuff is deflated. Nasal tubes (Figure 2) provide full access to the oral cavity and enable occlusion to be checked after the placement of dental restorations. They can be more complex to insert and are contraindicated in those with coagulopathies. Complications of nasal tubes include epistaxis, damage to nasal structures (avulsion of nasal polyps, fracture of turbinates) and bacteraemia from nasal cavity bacteria.11
Figure 2. A nasal tube.
Use of throat pack
Historically the use of a throat pack for all dental anaesthetics was standard practice to prevent the aspiration of fluid and debris into the respiratory airways intra-operatively and during extubating. The UK National Patient Safety Agency (NPSA) released a 2009 alert to reduce the risk of throat pack retention after surgery and recommended that local policies be implemented.12 While a throat pack is not always required,13 it can be beneficial when undertaking comprehensive care, including ultrasonic scaling removal of restorations and extractions. Such procedures can cause debris to be produced, and a throat pack can support the collection and removal of this debris from the airway (Figure 3). The report recommended that if a throat pack is indicated, the responsible person for its insertion and removal should be agreed upon, and it should be taken from the swab count.8
Figure 3. Throat pack with oral debris.
Maintenance of anaesthesia
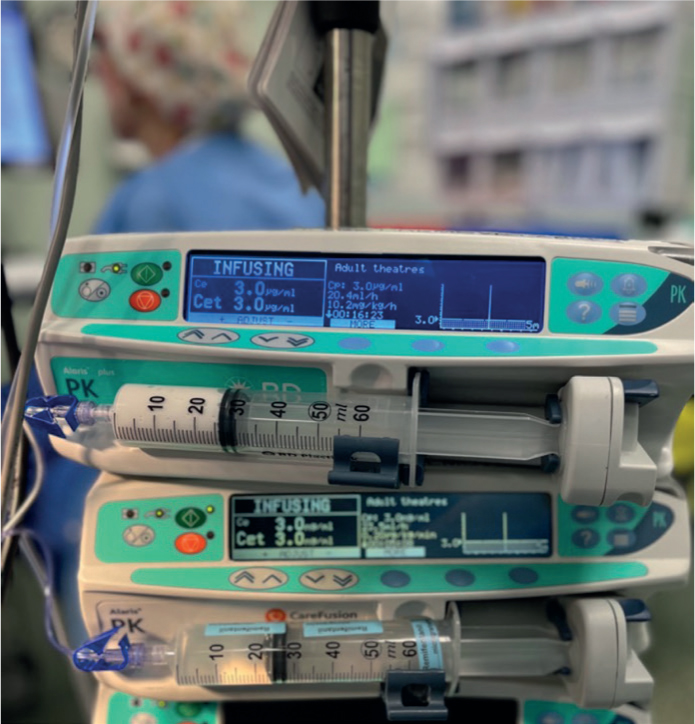
There are two established techniques of maintaining anaesthesia: volatile-based inhalational anaesthesia or propofol-based total intravenous anaesthesia (TIVA) (Figure 4). Sevoflurane is the most used volatile agent. Desflurane was once popular owing to its low blood solubility, which resulted in a faster wake-up time; however, it has been found to have an enormous global warming potential of 2540 times that of carbon dioxide.14 It has now been banned by NHS Scotland and NHS England is committed to phasing it out by 2024.15,16
Figure 4. A TIVA infusion set-up showing target-controlled infusions of remifentanil and propofol.
TIVA uses intravenous agents for a constant blood plasma level to maintain unconsciousness (Figure 4).17 The most used agent is propofol, with a short-acting opioid such as remifentanil. There is no direct measure of blood concentration like the end-tidal concentration of volatile agents, instead computerized syringe drivers are used to calculate the plasma concentration using complex pharmacokinetic models. Depth of anaesthesia monitors such as BIS (bispectral index) can be used to analyse brain electroencephalogram (EEG) activity and allow drug titration (Figure 5). This is important in the older population as persistent low BIS values (lower than 40 for GA) are associated with an increase in post-operative delirium.18,19
Figure 5. A bispectral index (BIS) monitor.
Intra-operative monitoring
Standard monitoring, as recommended by the Association of Anaesthetists, should be employed as a minimum. For general anaesthesia, this consists of electrocardiogram (ECG), pulse oximetry, non-invasive blood pressure, capnography and age-adjusted minimum alveolar concentration (MAC) if volatile gases are used.20 It should be commenced before induction and continued through to the recovery room.
A combination of metabolic rate dropping by 15–40% during anaesthesia and increased heat loss owing to loss of behavioural responses and vasoconstriction results in a risk of intra-operative hypothermia; therefore, warming during anaesthesia is important.21 Hypothermia can alter coagulation cascades, increase recovery time by altering drug metabolism and increase oxygen demand. Active warming, such as a forced hot air blanket and measurement of core temperature, should be employed.
Anti-emetics
Post-operative nausea and vomiting (PONV) is one of the most frequent adverse events after anaesthesia and can be very distressing for the patient. It has an incidence of around 30% in the surgical population.22 Special care dentistry (SCD) patients may be more susceptible to PONV owing to anxiety, sensory sensitivities or underlying medical conditions. Assessment of nausea can be difficult in patients with communication difficulties and therefore, prevention of PONV is key in ensuring post-operative comfort. This can be achieved by the avoidance of opioids and the use of prophylactic anti-emetics.
Dental treatment provision under GA
Examination under anaesthesia
When a patient is anaesthetized, a thorough intra-oral assessment should be completed, including a hard and soft tissue examination. This may be the only opportunity to identify soft tissue lesions (e.g. leukoplakias) that require a biopsy. Similarly, traumatic lesions (e.g. ulcers) may result from a tooth damaging the tissues and extractions of sound culprit teeth may be necessary if the ulceration is extensive and aggravating behaviour or preventing eating.
A periodontal health assessment, including a BPE, noting the gingival appearance, pocket depths, recession and mobility of teeth, is essential in assessing the overall prognosis and the likelihood of further deterioration. Full periodontal indices, however, are generally not indicated as they prolong the anaesthetic time and may not change the nature of treatment that can be delivered under GA.
Intra-oral radiography aids diagnosis and treatment planning and is useful for patient records, especially if the patient is likely to need future treatment under GA. Direct phosphor plate sensors connected to a mobile digital device (e.g. laptop) offer a quick method of obtaining radiographs without needing an additional processing tool. Self-developing films can also be useful where local processing is not possible.
Clinical photographs can also be useful to support documentation of a person's initial dental status, justify decision-making, and explain care to carers or family members. For teeth that are retained, photographs can be a useful baseline to determine any changes in oral status over time.
Dental treatment considerations
Treatment planning must be considered on a person-by-person basis,8 and should consider factors such as, but not limited to:
A person's preferences;
A person's oral hygiene;
The realistic prognosis of teeth that are heavily damaged;
The person's occlusion;
The impact of treatment on their wellbeing (both dentally, medically, and psycho-socially);
Their risk factors for future dental care;
The risks of future anaesthetic.
These ideal aims may lead to conflict, for example, if a person wishes to retain teeth, but the required treatment is not possible or feasible with GA, or where multiple episodes of GA may be needed to deliver it. Such potential issues should be discussed, and an agreement sought before a patient is listed to receive a GA.
Broad principles of treatment planning are summarized in BSSCD guidance,8 but potential treatments are summarized in Table 1. It is worth noting that intra-operative treatment decisions for patients who lack capacity should ideally be supported by two dentists, one of which should be a specialist or consultant in SCD.
Procedure
Rationale
Prevention
Preventive treatment provided should be based on the patient's oral health risk assessment and in line with current guidelines
Extractions
Unrestorable teeth
Caries extending to pulp in posterior teeth
Third molars likely to cause caries in the second molars
Periodontally involved teeth with poor long-term prognosis and no role in function
Root fractures
Overerupted teeth causing food trapping or trauma to opposing ridge
Restorations
Restorable teeth that contribute to oral function
Caries in enamel and dentine
Abrasion cavities
Fractures of anterior teeth that are deemed restorable
PMPR
Removal of supra and subgingival calculus to assess tooth structure and maintain periodontal health
Root canal treatment
Anterior teeth with good coronal tooth structure, where oral hygiene is sufficient
Discoloured anterior teeth
Prosthesis
Impressions/scanning for replacement of anteriors with resin-bonded bridges/Essix retainers provided that a patient could tolerate cementation under sedation post-operatively, or could tolerate a removable prosthesis
Extractions, professional mechanical plaque removal (PMPR), and basic restorations are the mainstay of treatment provided under GA in SCD. Local anaesthesia is not required for restorations alone, but provides pain relief for the post-operative period and intra-operative haemostasis (if adrenaline-containing local anaesthetic is used).23 For longer procedures, a long-acting anaesthetic such as 0.5% bupivacaine can be beneficial to support a reduction in orofacial pain in the immediate post-operative period. Local anaesthetic may need to be avoided in some patients, such as those with a history of lip biting post-treatment.
The delivery of fixed prosthodontics under general anaesthesia, and similar advanced reconstructive work is generally not appropriate under GA. Full mouth reconstruction of worn dentitions is typically not feasible, especially where risk factors have not been addressed, and further general anaesthesia would be required to maintain or replace any lost restorations affecting occlusion and oral function.
Post-operative anaesthetic processes
Once the dental surgery is complete, anaesthesia is reversed by discontinuing the volatile or intravenous agents. In the fourth national audit project that analysed airway complications in anaesthesia, a significant number of airway complications occurred at emergence of anaesthesia (16%) or in or during transfer to recovery (14%).24 Laryngospasm can occur at this time if the endotracheal tube is removed too early or if blood or debris falls onto the vocal cords before the patient has regained their airway reflexes.
It is recommended that patients receive supplemental oxygen on transfer to the recovery room unless they had no oxygen requirement during treatment.25 Reasonable adjustments should be made, and discharge straight from the recovery room (without the need to return to the ward/discharge lounge) should be considered in patients who are likely to get agitated or experience behaviour that challenges recovery. Early presence of a familiar relative or carer may be beneficial in the recovery room. Avoiding delays in discharge is essential for many SCD patients, and communication with the recovery team informing them that the usual requirements of post-operative eating/drinking/urinating may not be necessary for specific groups.
Analgesia
Post-operative analgesia should not be overlooked, especially in those who have communication difficulties, for example those with severe dementia or those with learning difficulties. A combination of local anaesthetic and simple analgesics achieves multimodal analgesia. Often, paracetamol and non-steroidal anti-inflammatories (NSAIDS) will suffice if not contraindicated for the patient. As discussed above, local anaesthesia may reduce the requirements for stronger post-operative analgesics, such as opioids.
Post-operative cognition disorders
Some patients may experience a brief period of delirium when emerging from anaesthesia, which clears fully after a few minutes. Persistent post-operative delirium or post-operative cognitive decline (POCD) is seen more commonly in those with advanced age or with a pre-existing cognitive impairment.
Post-operative delirium is a fluctuating disturbance in attention and awareness that develops over hours to days. It is a direct consequence of surgery, a medical condition, medication, or a combination of causes. It causes an increase in hospitalizations, mortality and morbidity and can be distressing to family members, staff and other patients.
Non-pharmacological methods of treating delirium should be employed in the first instance. These include:
Presence of a familiar person;
Orientating the patient to time, place and person;
Regular communication and explanations;
Ensure communication aids are present, e.g. hearing aid, glasses;
Normalizing post-operative care, e.g. normal mealtimes and rest times;
Low background noise, well-lit rooms.
Inpatient GA
Some patients may need to be admitted overnight, planned or unplanned, after surgery.
It is important for patients with additional needs that a carer or family member can stay with them. As in most cases, special care dentistry usually does not have privileges to admit patients, a local arrangement must exist for overnight care, generally with maxillofacial surgery teams. A member of the dental team should discharge the patient unless a comprehensive handover has been provided to the team responsible for the patient's overnight admission.
Follow-up post-anaesthetic
Patients and their carers should be provided with verbal and written information about their dental care and anaesthetic. This should include information on who to contact if there are concerns or complications within working hours and out of hours. It is good practice for a dental team member to contact the patient/carer, ideally within 48 hours, to check on the person's recovery and answer any questions or queries that may have arisen post-treatment.
Follow up of investigations carried out (e.g. blood tests) should be undertaken by the requesting clinician, with results forwarded on to the relevant physician (e.g. to general practitioner) to avoid reliance on information sharing via carers.
Copies of clinical charts, details of treatment delivery, radiographs, clinical photographs and other relevant clinical information should be forwarded to the patient's regular dental care team to aid review and ongoing care. Establishing and maintaining a good oral care preventive regimen post-treatment is very important to help maintain oral health and reduce the need for further dental intervention under anaesthetic within a close time frame. Plans to see the patient regularly by their general dental practitioner or special care dental team is important, in addition to prevention to try and reduce the need for further dental treatment for as long as possible.
Summary
A great deal of planning may be required when general anaesthesia is being considered to support the delivery of dental care. The care of some patients inevitably requires more planning than for others, especially when numerous reasonable adjustments are considered to support a person to receive care. While pre-operative dental examinations may not always be possible, planning the processes of hospital attendance, in-depth consent and best interest processes and pragmatic treatment planning aim to secure suitable long-term oral health outcomes for patients with complex needs.