Ng YL, Mann V, Rahbaran S Outcome of primary root canal treatment: systematic review of the literature – part 1. Effects of study characteristics on probability of success. Int Endod J. 2007; 40:921-939 https://doi.org/10.1111/j.1365-2591.2007.01322.x
Ricucci D, Pascon EA, Siqueira JF The complexity of the apical anatomy. In: Versiani M, Basrani B, Sousa-Neto M Cham, Switzerland: Springer; 2019
Gotler M, Bar-Gil B, Ashkenazi M Postoperative pain after root canal treatment: a prospective cohort study. Int J Dent. 2012; https://doi.org/10.1155/2012/310467
Alzahrani MS, Alzahrani AAH, Alhuwairini SM Post-endodontic treatment flare-up of patients treated by general dentists and endodontic specialists. J Dent Sciences. 2021; https://doi.org/10.23880/oajds-16000315
Katebzadeh N, Sigurdsson A, Trope M Radiographic evaluation of periapical healing after obturation of infected root canals: an in vivo study. Int Endod J. 2000; 33:60-66 https://doi.org/10.1046/j.1365-2591.2000.00301.x
Del Fabbro M, Taschieri S, Testori T Surgical versus non-surgical endodontic re-treatment for periradicular lesions. Cochrane Database Syst Rev. 2007; https://doi.org/10.1002/14651858.cd005511.pub2
Torabinejad M, Corr R, Handysides R, Shabahang S Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009; 35:930-937 https://doi.org/10.1016/j.joen.2009.04.023
Ng YL, Gulabivala K Factors that influence the outcomes of surgical endodontic treatment. Int Endod J. 2023; 56:(Suppl 2)116-139 https://doi.org/10.1111/iej.13896
Ramachandran Nair PN, Pajarola G, Schroeder HE Types and incidence of human periapical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 81:93-102 https://doi.org/10.1016/s1079-2104(96)80156-9
Karabucak B, Setzer F Criteria for the ideal treatment option for failed endodontics: surgical or nonsurgical?. Compend Contin Educ Dent. 2007; 28:391-407
Kvist T, Henelius D, Smakiqi A Endodontic retreatment decision-making: the influence of the framing effect. Clin Exp Dent Res. 2023; 9:290-298 https://doi.org/10.1002/cre2.715
Dawood A, Patel S The dental practicality index – assessing the restorability of teeth. Br Dent J. 2017; 222:755-758 https://doi.org/10.1038/sj.bdj.2017.447
Tifooni A, Al-Nuaimi N, Dawood A, Mannocci F, Patel S Validation of the effectiveness of the Dental Practicality Index in predicting the outcome of root canal retreatments. Int Endod J. 2019; 52:1403-1409 https://doi.org/10.1111/iej.13142
Abbott PV Assessing restored teeth with pulp and periapical diseases for the presence of cracks, caries and marginal breakdown. Aust Dent J. 2004; 49:33-45 https://doi.org/10.1111/j.1834-7819.2004.tb00047.x
Magne P, Spreafico RC Deep margin elevation: a paradigm shift. Am J Esthet Dent. 2012; 2:86-96
Mullally BH, Ahmed M Periodontal signs and symptoms associated with vertical root fracture. Dent Update. 2000; 27:356-360
Patel S, Bhuva B, Bose R Present status and future directions: vertical root fractures in root filled teeth. Int Endod J. 2022; 55:(Suppl 3)804-826 https://doi.org/10.1111/iej.13737
Patel N, Gemmell A, Edwards D When to consider the use of CBCT in endodontic treatment planning in adults. Dent Update. 2021; 48:932-941 https://doi.org/10.12968/denu.2021.48.11.932
Gómez-de Diego R, Mang-de la Rosa Mdel R, Romero-Pérez MJ Indications and contraindications of dental implants in medically compromised patients: update. Med Oral Patol Oral Cir Bucal. 2014; 19:e483-e489 https://doi.org/10.4317/medoral.1956
This narrative review considers the common clinical dilemma of choosing from non-surgical root canal re-treatment (NSRCreT), surgical root canal re-treatment or dental extraction. While orthograde root canal treatment is generally successful, cases with unresolved symptoms or persistent infection prompt the need for orthograde root canal re-treatment or surgical intervention. The latter involves microsurgery, reserved for suitable cases. Deciding on the appropriate treatment requires a holistic understanding of the patient, the existing dentition and specific tooth factors. This article discusses insights into decision-making, fostering optimal endodontic care and successful treatment outcomes.
CPD/Clinical Relevance: Knowledge of current recommendations regarding non-surgical root canal re-treatment, extraction or referral for apical surgery is useful knowledge.
Article
Endodontics has seen recent advances in equipment, materials and techniques for non-surgical and surgical approaches, resulting in improved outcomes and altering considerations for different treatment options. Selecting the appropriate treatment requires a comprehensive evaluation of the patient's clinical signs and symptoms, as well as considering the ‘bigger picture’, with factors including tooth anatomy, restorative status, periodontal condition, and systemic health all influencing decision-making. This article addresses a common clinical dilemma: determining when to consider non-surgical root canal re-treatment (NSRCreT); refer patients for endodontic surgery; or extract a tooth.
Background
Root canal treatment is highly successful for managing peri-radicular pathologies related to an infected root canal system, with up to 96% of cases resolved with primary, non-surgical root canal treatment alone.1 However, there are cases where initial treatment fails to resolve symptoms or eliminate infection. This leaves practitioners with the decision to either perform non-surgical root canal re-treatment, extract the tooth or refer for surgical intervention. NSRCreT involves revisiting the root canal system to address persistent symptoms and eliminate residual infection. Where the cause of failure is clear, this may be achievable in a general practice setting, but may sometimes require more advanced clinical techniques.2,3
Alternatively, endodontic microsurgery may be more appropriate. This involves surgically resecting the apical portion of the root, followed by sealing the root-end to prevent further infection, with the aim of removing the part of the root housing complex anatomy and eliminating residual bacteria.4 This procedure is reserved for cases where NSRCreT is less likely to succeed, among other factors discussed throughout this article. In contrast, cases with a hopeless prognosis must be identified, where extraction and replacement should be considered as first-line treatment.
Endodontic failure
Following initial root canal treatment (RCT), success can be determined in several ways, with abatement of pre-operative symptoms being the most obvious. Post-endodontic treatment pain is typically transient, and eases within the first few days following obturation.5 Should pain persist, or increase in the days and weeks following the RCT, failure of the root canal treatment is the most likely cause. However, mechanical irritation of peri-apical tissues can cause similar symptoms, with overinstrumentation of the root canal and extrusion of material through the apical foramen being the likely causative factors.6
Other signs and symptoms of recurrent infection include the presence or persistence of an apical abscess. The use of a GP point inserted into a draining abscess often allows localization of the tooth from which pathology originates.
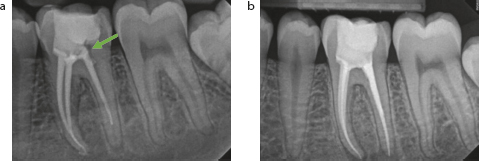
Radiological examination of the RCT provides important information regarding the quality of endodontic treatment provided, indicating potential reasons for failure, and aiding in the decision on further treatment options. Simple factors, including obturation in relation to the radiographic apex, homogeneity of obturation and a wellsealed coronal restoration typically result in favourable outcomes (Figures 1 and 2).8 The gutta percha should be closely adapted to the canal walls, with no visible canal space beyond the endpoint of the root canal filling and without extensive extruded obturation material.14 Additionally, it is desirable to obtain information on the previous RCT concerning the quality of isolation and irrigation. This may be done through the review of records or during history taking (Table 1).
Figure 1.
(a,b) Non-surgical root canal re-treatment of LL6 because of continued symptoms following initial obturation. The distal canal is short of the radiographic apex, with obvious voids in the floor of the access cavity and coronal restoration (as shown by the green arrow in (a)). Following the re-treatment of this tooth with obturation to the radiographic apex, the patient's symptoms resolved.Figure 2. Root canal re-treatment of UL1 owing to continued symptoms following initial obturation. (a) The root canal contains obvious voids throughout the full length of the first obturation (green arrows). (b) The previous root filling, once removed from the canal, along with a thermafill carrier also removed from the root canal system. (c) Endodontic re-treatment using a bioceramic apical plug followed by thermoplastic obturation.
Causes of endodontic failure
How to identify the cause?
Inadequate chemical disinfection
Discussion with patient and review of clinical notes from the initial RCT appointment (if available):Was rubber dam isolation used?Can the patient remember the smell of bleach (indicating using of sodium hypochlorite)?Was Corsodyl used for canal disinfection?
Inadequate mechanical preparation
All canals should be instrumented and obturated to within 2 mm of the radiographic apex. Radiographically, the GP/sealant should be well adapted to the canal walls throughout the full length of the canal
Missed anatomy
Suspicion of a second root or second root canal which has not been located, instrumented and obturated
Iatrogenic causes
Suspicion of perforation/strip perforation indicated by radiographic bone loss or presence of a sinus. Identified intra-operatively through insertion of a file with attached apex locator into the suspected perforation. A perforation is confirmed through ‘apex location’ when a file is only just inserted into the defect
Poor coronal seal
Identified through clinical and radiological examination of the coronal restoration (direct restoration/crown). Evidence of caries is a likely cause of bacterial reinfection of the root canal system
Poor apical seal
The tooth should be instrumented and obturated to within 2 mm of the radiographic apex
Resistant micro-organisms
Unable to resolve symptoms and remove infection even with optimal root canal disinfection
Care must be taken when interpreting the size of apical pathology as a marker for disease regression with two-dimensional radiographic imaging (e.g. peri-apical or dental panoramic tomography). Differing angulation of the X-ray beam, altered exposure, angulation of the film, processing errors and image processing can give the illusion of a change in size of pathology.7
Clear deficiencies in a previous root filling (including voids, lack of patency, etc.) and lack of adherence to guidelines for root treatment (e.g. use of rubber dam isolation), would require non-surgical root canal re-treatment should the patient be keen to retain the tooth.8 The predictability of NSRCreT may reduce if previous high-quality treatment has failed. This requires clinicians to investigate the potential reasons for failure to inform subsequent treatment planning (common reasons for endodontic failure are outlined in Table 1). Attempting peri-radicular surgery as first-line treatment in these cases may be inappropriate, introducing risks associated with surgery, and increasing post-operative morbidity.
When to consider surgical endodontics
Systematic reviews indicate that non-surgical re-treatment, when attempted first, may yield a more favourable long-term outcome compared with surgical endodontic treatment.9,10 However, advances in modern tricalcium silicate cements and microsurgical techniques have improved the predictability of surgical approaches. Varying success rates for peri-apical microsurgery are reported, with a systematic review reporting 77% success,12 and a recent narrative review reporting 48–93%, with a trend of increased success in more recent studies.11,12 Moreover, in cases of symptomatic and progressive peri-radicular disease, apical surgery can be considered a preferred first-line treatment option under specific circumstances (Tables 2 and 3).
Indications for apical surgery
Image/radiographic depiction
Previous treatment has been carried out to guideline standards, but clinical/radiographic outcomes suggest failure6
No reduction in apical pathology following obturation. In these cases, the RCTs can be deemed to be unsuccessful and apical surgery may be indicated
Instances where non-surgical root canal re-treatment may be detrimental to the structural integrity of the tooth or be destructive to a restoration or fixed prosthesis
Symptomatic UL2 requiring further treatment. Removal of the post-crown would likely damage the underlying tooth structure, rendering the tooth unrestorable. As such, a surgical approach was the preferred treatment option and successfully resolved symptoms
Symptomatic teeth in which iatrogenic/developmental anomalies (dens in dente) prevent conventional root canal treatment being undertaken
When completing root treatment for this tooth, the apical third could not be negotiated. As such the tooth was obturated to the level of the perforation and subsequent apical surgery performed
When visualization of the peri-radicular tissues and tooth root is required if perforation or root fracture is suspected
Surgical access allows for exploration to discover causes of symptoms and apical pathology. The UL2 was found to have a perforation caused by a cast-post (left image). The region was smoothed and repaired with MTA, alongside conventional apicectomy. Images courtesy of Dr Mark Ritchie
Contra-indications for apical surgery
Image/radiographic depiction
Primary disease (caries/poor coronal seal or periodontal disease) has not been stabilized
Poor coronal seal with overhanging crown margins and distal caries (shown by the green arrow)
The tooth is unrestorable
Limited ferrule and supragingival tooth tissue remaining (as shown by the green arrow). Even with longstanding apical pathology the most predictable treatment option is likely to be extraction
The apical lesion is a confluent perio–endo lesion
Root treatment of the LL7 to resolve a perio-endo lesion. Apical surgery is this case would not be successful in resolving the pathology and therefore conventional root canal re-treatment is the treatment of choice. Images courtesy of Dr Tauseef Mahmood
The prognosis of the tooth is limited by compromised bone support or its root length should root-end resection be carried out.
Root canal treated UR1 already exhibiting approximately 50% bone loss. Given that apical surgery would remove 3 mm of apical root, this would render the crown–root ratio of this tooth to <1:1. Image courtesy of Professor John Whitworth
Presence of a root fracture
Upon accessing this molar, a crack could be visualized in the pulp chamber across the mesial and buccal walls and extending down the MB root canal. The subsequent extraction depicts the extent of the root fracture
The root apex is in close association with anatomical structures (maxillary antrum, mental foramen)
Continued symptoms from the UL2 following RCT. The palatally ectopic UL3 contra-indicated apical surgery, and so orthograde re-RCT is the preferred treatment modality so as not to damage the canine
The nature of the peri-apical lesion, classified as peri-apical abscesses, granulomatous, or cystic, may also be a cause of primary RCT failure, and compromise outcomes of orthograde re-RCT.15 True cysts separated from the root are an example of lesions that require surgical intervention as the first-line treatment (enucleation, marsupialization or decompression).
In cases of failed non-surgical root canal re-treatment, further non-surgical re-treatment becomes less predictable, making a surgical approach advisable.8,16 Extra-radicular infections with biofilms on the root surface and colonies of resilient species, such as Actinomyces and Propionibacterium, within the soft tissue lesion may also hinder the success of NSRCreT, although this may not be known until the treatment has failed.17
Further challenges to non-surgical root canal re-treatment include accessing the root canal system through complex restorations such as Nayyar cores, fibre posts or cast metal posts. Although posts can often be safely removed with appropriate techniques to avoid root fractures,18,19 where post removal may compromise the structural integrity of the tooth, or the benefits of further chemo-mechanical disinfection through NSRCreT cannot be justified. These cases will often benefit from surgical approaches as a first-line option.
Successful RCT relies heavily on thorough disinfection throughout the canals.14 This may be challenging with complex canal anatomy, such as significant curvatures (>30°), multiple roots and root canal systems, or long roots (>25 mm), posing considerable challenges.20 Additional factors, including calcifications, resorptions, and iatrogenic errors (including file fractures and perforations), can further hinder effective chemo-mechanical debridement, making non-surgical treatment increasingly challenging. These issues are further enhanced the closer they occur to the apex.21
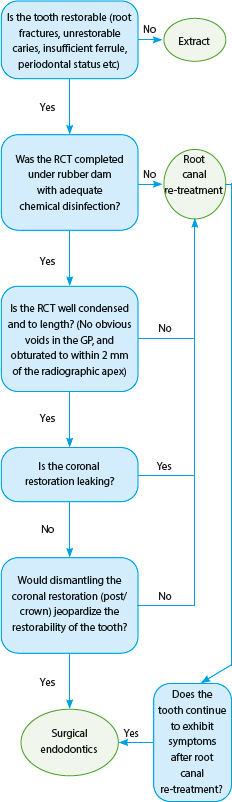
Should any of the above factors be present when clinically or radiologically examining a patient's previously root-treated tooth, referral to a secondary or tertiary care setting is advised for consideration of surgical intervention. These factors are summarized in Figure 3.
Figure 3. Suggested decision tree for the management of symptomatic root-treated teeth.
Restorability of the tooth: the bigger picture
Considering technical limitations, anatomical complexities, and iatrogenic errors, the feasibility of restoring a tooth should be the primary concern before considering either non-surgical root canal re-treatment or apical surgery. To aid in the decision-making process about restorability and effectively communicating them to patients, the dental practicality index (DPI) proves to be a valuable tool.22,23 The DPI evaluates the structural integrity of the tooth, its periodontal stability, endodontic requirements, and other contextual factors, such as overall restorative needs, social aspects, dental history, and medical considerations.
At the level of the tooth
An initial step in assessing restorability may involve the removal of existing restorations, because this can help identify the cause of failure and most importantly, the restorability of the tooth. By removing restorations, issues, including caries, cracks, and marginal breakdowns become more apparent. This can be a critical step, with one study identifying caries in 19.2% of teeth, which increased to 86.1% following complete removal of the coronal restoration.24 Furthermore, this procedure allows for direct visualization of supra- and subgingival margins, facilitating decisions between extraction, deep marginal elevation, or the possibility of placing an indirect restoration margin.25 Additionally, this enables the examination of the ferrule and improves the visualization of angulation for access of the root canal system, reducing the risk of iatrogenic errors.26
The presence of fractures extending to the root surface reduces the prognosis of the tooth, and treatment options become limited to extraction.27 Clinically, the presence of a single, deep, narrow periodontal pocket around the affected tooth, along with mobility in a post or coronal restoration, may indicate a fracture. Additionally, a ‘J-shaped’ lesion seen radiologically, or the loss of the periodontal ligament space could also suggest a fracture.28 More advanced imaging techniques, such as cone beam computed tomography (CBCT), can predictably demonstrate patterns of bone loss that are indicative of a fracture.29,30
Bony support and root length must also be considered part of this assessment. Extensive crestal bone loss, or the presence of vertical bony defects in the region of the tooth in question would be likely to contraindicate apical surgery. Teeth with already compromised bony support or a decreased crown:root ratio would lose further support following apical surgery and as such, NSRCreT or extraction may be favourable.13 The same concept applies to teeth with shortened roots. Considering the 3 mm lost for apical surgery, if the remaining crown:root ratio would be less than 1:1, endodontic surgery would not be a viable treatment option.
When teeth do not meet the criteria of restorability, consideration of non-surgical root canal re-treatment or surgical endodontics is futile. The most pragmatic option would be extraction, with a discussion with the patient about replacement options, whether fixed or removable.
Other considerations of peri-apical surgery include potentially negative consequences. Any form of surgery requiring the raising of a full-thickness periosteal flap can lead to localized gingival recession. This must be considered when planning surgery in the aesthetic zone, especially around crown margins (Figure 4). Recession in patients with high smile lines can lead to poorer aesthetic outcomes, and in the most aesthetically driven patients, preferential outcomes may be acquired through extraction and prosthetic replacement.
Figure 4.
(a,b) Pre-existing restorations in the upper anterior region. Apical surgery for the previously root canal-treated UL1 successfully resolved the chronic apical abscess. However, following surgery, approximately 2 mm of recession was noted in the region of the flap raised. Images courtesy of Dr Mark Ritchie.
At the level of the patient
A holistic examination of the patient is often overlooked when considering viable options to manage symptomatic root-treated teeth. Patients with unstable dentitions (unrestored caries and unstable periodontal disease) should not be considered for apical surgery until they become dentally stable. In such cases, the most pragmatic treatment option may be to consider extraction and replacement options for teeth with the poorest prognosis.
A further factor to consider is the patient's medical history regarding direct contra-indications for surgery. Surgical procedures can generally be considered for patients with cardiac diseases, diabetic/endocrine pathologies, and controlled metabolic disorders. However, caution is advised for those who smoke or have undergone head and neck radiotherapy, because they may experience increased failure rates and post-operative complications (including osteoradionecrosis). Patients with osteoporosis undergoing bisphosphonate therapy, particularly via intravenous administration, face an elevated risk of MRONJ following surgery.31 Finally, bleeding disorders or anticoagulant/antiplatelet medications are not a direct contra-indication to surgical procedures. However, care must be taken because apical surgery is generally elective, and therefore, procedures carrying a lower risk of bleeding may be attempted in the first instance.
Conclusion
Navigating the decision between NSRCreT and surgical intervention is a critical aspect of endodontic care. By staying informed of the latest advances and considering patient-specific factors, GDPs can provide their patients with all viable treatment options. By understanding each approach's indications, limitations, and outcomes, practitioners can deliver optimal care and achieve successful patient treatment outcomes.