Friedrich RE, Scheuer HA, Gröbe A. Anterior lingual mandibular bone depression in an 11-year-old child. In Vivo. 2012; 26:1103-1107
Sisman Y, Etöz OA, Mavili E Anterior Stafne bone defect mimicking a residual cyst: a case report. Dentomaxillofac Radiol. 2010; 39:124-126 https://doi.org/10.1259/dmfr/49320253
Deyhimi P, Darisavi S, Khalesi S. Stafne bone cavity with ectopic salivary gland tissue in the anterior of mandible. Dent Res J (Isfahan). 2016; 13:454-457 https://doi.org/10.4103/1735-3327.192306
Shokri A, Baharvand M, Mortazavi H. Is cone-beam computed tomography diagnostic for anterior Stafne bone cyst: Report of a rare case. Dent Hypotheses. 2015; 6:31-33
Etöz M, Etöz OA, Sahman H An unusual case of multilocular Stafne bone cavity. Dentomaxillofac Radiol. 2012; 41:75-78 https://doi.org/10.1259/dmfr/34731967
Krafft T, Eggert J, Karl M. A Stafne bone defect in the anterior mandible--a diagnostic dilemma. Quintessence Int. 2010; 41:391-393
Watanabe A, Yoshida S, Kato H A rare case of static bone cavity in the anterior mandibular region of a 10-year-old boy. Int J Surg Case Rep. 2021; 83 https://doi.org/10.1016/j.ijscr.2021.106019
Dereci O, Duran S. Intraorally exposed anterior Stafne bone defect: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 113:e1-3 https://doi.org/10.1016/j.tripleo.2011.07.029
Pellatt A, Wooi M, Revington P. Stafne bone cavity: a rare case affecting the anterior mandible. J Oral Dis Markers. 2019; 3:33-35
Öztürk B, Zirek T, Altındağ A, Taşsöker M. Stafne kemik kavitesi: vaka serisi. NEU Dent J. 2023; 8:139-145
Manigandan T, Rakshanaa TVR, Dornadula P. Atypical variant of Stafne bone defect mimicking odontogenic cyst of the jaw. J Oral Maxillofac Pathol. 2023; 27:S91-S94 https://doi.org/10.4103/jomfp.jomfp_255_22
Aydin U, Oguz Y. Stafne bone cavity incidentally ‘Twice’ diagnosed on panoramic radiographs. J Oral Maxillofac Radiol. 2014; 2:26-29
This report presents imaging findings of a rare case of anterior lingual mandibular bone depression in a child. These defects are typically localized at the lingual cortical area of the lower jaw and have been diagnosed casually during routine radiographic examination. We presented very different information about the prognosis and formation hypotheses of the lesion observed in a child than has been presented so far. The purpose of this report is also to introduce a new case of an anterior lingual mandibular bone defect and to focus on clinical features, alternative diagnostic imaging sources differential diagnoses and review the current literature.
CPD/Clinical Relevance: An anterior lingual mandibular bone depression mimicking a Stafne bone defect is described.
Article
Anterior lingual mandibular bone depression (ALMBD) is categorized as the anterior equivalent of the similar posterior mandibular lingual bone depression (or defect) known as Stafne's cavity. The first case of ALMBD was reported by Richard and Ziskind in 1957.1 It is rare to observe this defect in children and most lesions are diagnosed in adults.2
Anterior bone defects (ABDs) are rarely seen compared to posterior ones. Both anterior Stafne bone defects (ASBDs) and ALMBDs are thought to be caused by pressure of the sublingual salivary glands.2,3 The exact mechanism of this bone resorption, however, remains uncertain.2 ASBDs and ALMBDs are pseudocysts of the mandible and have also been referred to as lingual mandible bone cavities, lingual mandible bone depressions, mandibular salivary gland inclusions, and static, latent, or idiopathic bone cysts, cavities, or defects.4 While these are non-neoplastic bony lesions, their radiographic features and clinical manifestations can resemble other intra-bony neoplastic lesions. These defects are most often unilateral and rarely bilateral. Usually, both lesions are randomly identified during radiographic examination. Some additional imaging methods, such as magnetic resonance imaging (MRI), computed tomography (CT; also known as multislice CT), cone beam computed tomography (CBCT), and sialography, can be helpful to confirm the diagnosis of atypical lesions and avoid unnecessary surgical procedures, because these lesions are frequently asymptomatic.5 Dental clinicians should be aware of this entity to prevent unnecessary biopsies. In most cases, clinical and radiographic follow up is the recommended course of action. In this article, we report a rare case of a 12-year-old girl with an asymptomatic, unilocular ALMBD in the left mandibular area that showed an unusual healing pattern with a preliminary diagnosis of ASBD.
Case report
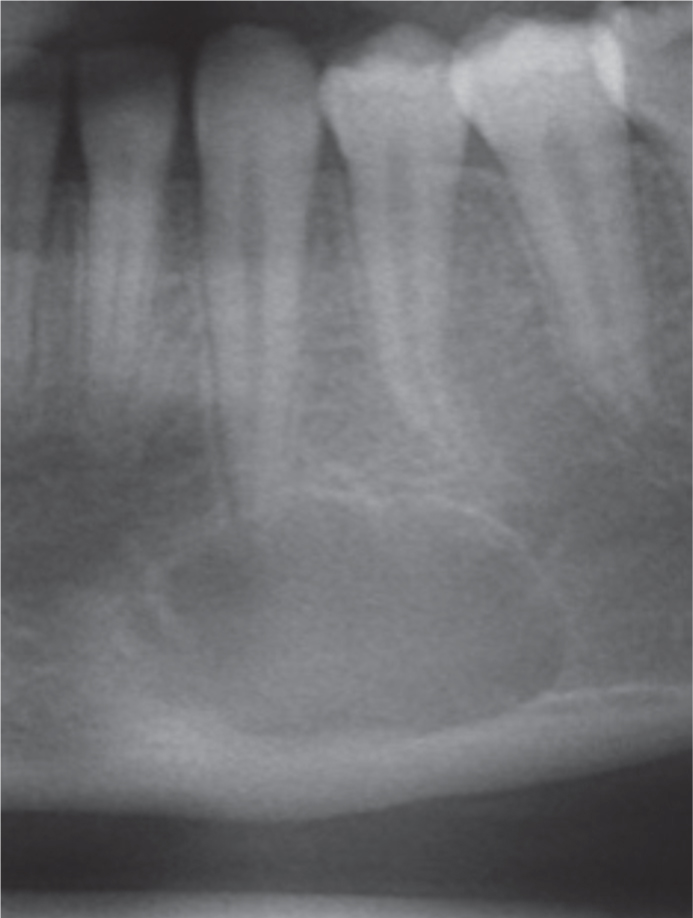
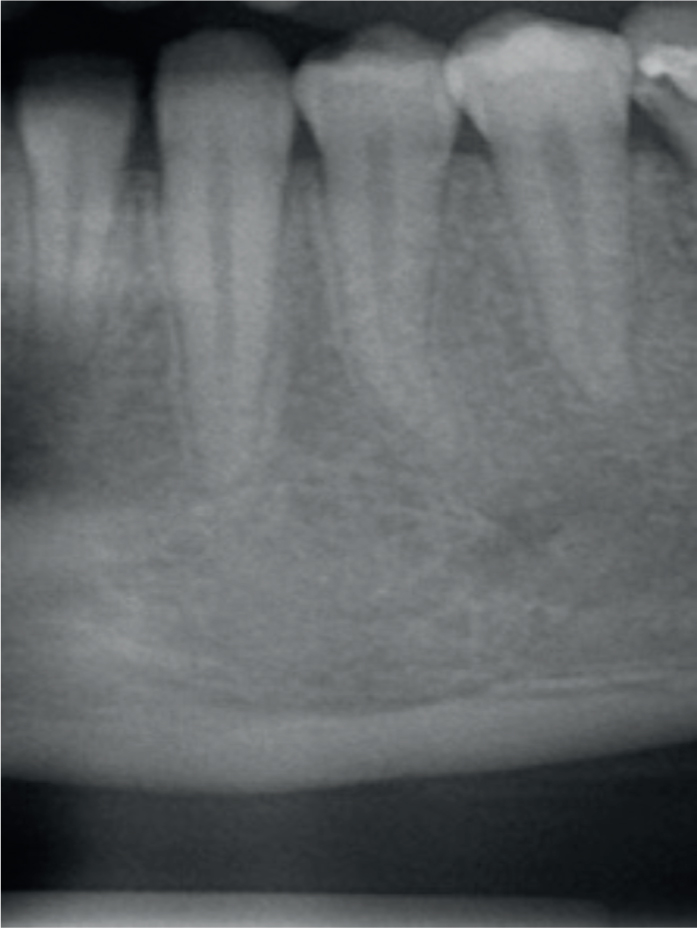
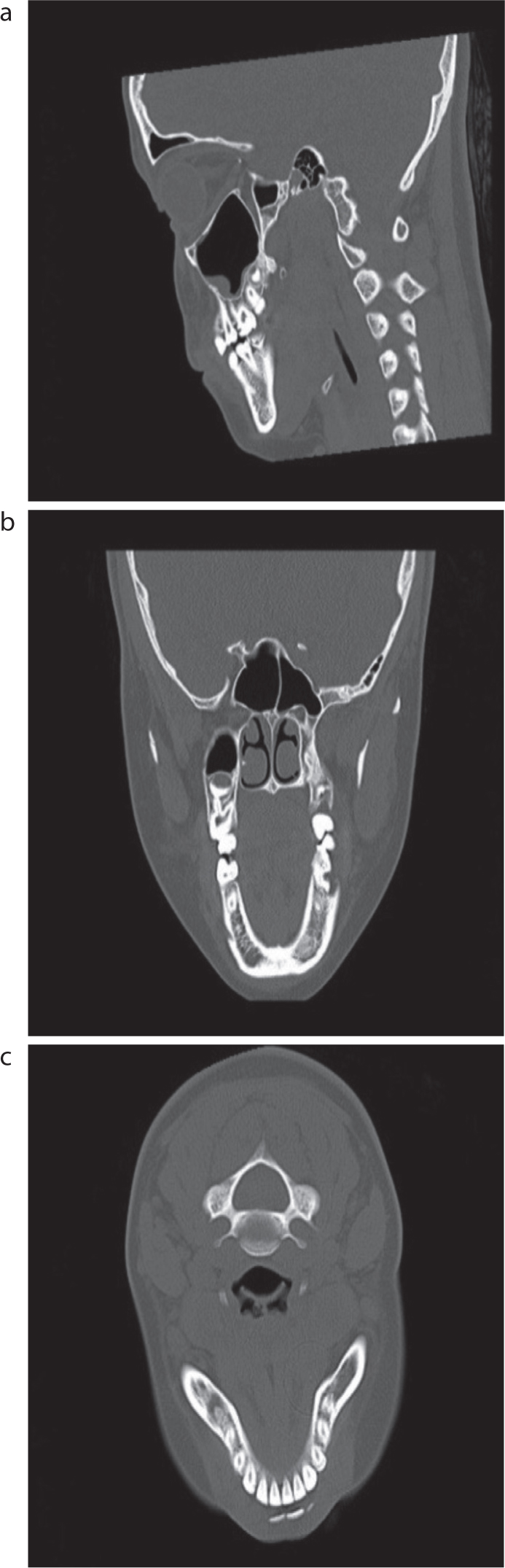
A 12-year-old female patient presented to our clinic for a routine appointment. During routine radiography, an ovoid-shaped, unilocular, well-limited radiolucent lesion with dimensions of 22×15 mm extending from below the apex of the mandibular left canine and first premolar teeth to the mandibular cortex was observed (Figure 1). Clinical examination revealed that the oral mucosa was healthy in the radiolucent area. In the anamnesis taken from the patient, the lesion was determined to be asymptomatic, and there was no history of trauma, genetic disorder, infectious disease, e or any pathology. There was no pain or swelling around the lesion and no abnormality in salivary flow. After an extra-oral examination, no facial asymmetry or lymphadenopathy was seen. All of the associated teeth were vital, and there was no root resorption. Owing to the localization of this lesion, we decided to obtain CT images for differential diagnosis. Consent to take the images was obtained from the patient's parents. It was observed that the lesion examined in the axial, coronal and sagittal sections extended to the lingual cortex. CT imagery revealed a 20×16×15-mm well-defined oval shaped defect on the lingual cortical bone at the apex of the mandibular left canine and first premolar (Figure 2). Based on the shape and size of the present defect, the absence of any clinical symptoms, the exclusion of other pathologies, and the child's age, no surgical treatment was performed. The lesion was thought to be an ALMBD and the patient was informed about the normal variation with follow up recommended. Using routine radiograph and CT images at the 2-year follow-up, it was observed that the lesion was filled with bone. Therefore, the lesion was defined as ALMBD (Figures 3 and 4).
Figure 1. The initial radiograph shows a unilocular peri-apical radiolucency below the apex of the left mandibular canine and first premolar teeth.Figure 2.
(a–c) CT images taken from different sections show the lesion with a well defined border and extends into the mandible cortex.Figure 3. The 2-year radiograph shows changes in the lesion dimension and the boundaries.Figure 4.
(a–c) The 2-year CT images show that the lesion is completely filled with bone.
Discussion and conclusions
ASBDs were first defined by Stafne as well-defined radiolucent lingual bone defects located below the mandibular canal that were usually unilateral and asymptomatic.6 ASBDs are unilocular radiolucencies with well-defined borders and are often detected during routine radiographic inspection owing to their asymptomatic nature.7 Radiographically, ASBDs typically appear as unilocular, circumscribed radiolucencies as in our case, but Etöz reported a multilocular lesion in one case.8 In most cases, a soft tissue invagination into the lingual cortical plate is noted above the level of mylohyoid insertion.6,9 ALMBDs are located in the sublingual gland area (in the incisor–canine–premolar region) and anterior lingual mandibular corpus.10 The presence of ALMBD in childhood is quite rare, and there is little research about this entity. There is only one reported case of ALMBD in paediatric patients to date, recorded by Friedrich et al.2 Previous publications have reported that ASBDs are more common in males than in females.7 Our case is rare in terms of the region of the lesion and the patient's age and gender.
ALMBDs are infrequent subtypes of ASBDs. ALMBDs may be confused with other pathologies such as residual cysts, traumatic bone cysts, giant cell granulomas, bone marrow defects, periapical cemento-osseous dysplasia (PCOD), radicular cysts, lateral periodontal cysts, ameloblastomas or odontogenic keratocysts (OKs).11,12 A residual cyst describes an inflammatory odontogenic lesion in which inadequate curettage of the cyst remains after the removal of the relevant tooth. This may imitate ALMBDs if the defect is in an edentulous region. The absence of a previous non-vital tooth/radicular cyst is the main distinguishing factor when differentiating ALMBD from a residual cyst.
If the bone defect is associated with the root apices, it may imitate an inflammatory cyst. Endodontic treatment may be performed because of this misinterpretation. A pulp vitality test should be applied to prevent unnecessary root canal treatment.12,13 The existence of dental caries and changes in the lamina dura of the teeth adjacent to the defect can also aid the clinical diagnosis. Simple bone cysts may also be included in the differential diagnosis. However, these pseudocysts may seem oval-shaped or scalloped around the roots of the teeth, and aspiration biopsy of the lesions contains blood, which helps with diagnosis. OKs can also be seen as unilocular radiolucent lesions with cortical borders. OKs grow more aggressively than odontogenic lesions and may cause root resorption and cortical thinning. This information can be useful for differential diagnosis. In the early stages of development, immature lesions of cemento-ossifying fibroma and cemento-osseous dysplasia may appear radiolucent and mimic ALMBDs. These lesions will usually turn into radiopaque foci if they are not treated. This ALMBD case could not have been misdiagnosed as PCOD owing to its radiological findings and location below the mandibular canal and the apical region of the affected teeth. The radiographic findings of ameloblastomas can vary from unilocular to multilocular radiolucencies. Ameloblastoma is generally present near the angle of the mandible. However, they can cause root displacement, resorption, and expansion of the jaws. Consequent cut-shaped root resorption of teeth can provide important clues to differentiate these two diseases because ALMBD has no relationship to the teeth.14
The aetiopathogenesis of ALMBDs is under-recognized. Most authors believe it has a congenital origin, others consider it a developmental entity.3 However, some authors have accepted the pressure resorption theory as the main aetiological factor for the majority of cases. According to this theory, owing to a chronic inflammatory process, salivary gland hypertrophy can exert enough pressure to cause bone resorption.15–17 Owing to the relationship between the bone defect and its corresponding sublingual gland, the hypertrophic sublingual gland could be the cause of ALMBD.3,9 However, none of these theories has been proven. Radiographic evaluation of ABDs can be a diagnostic challenge. Positional errors may lead to magnification, and limit dimensional accuracy on panoramic radiographs.18 However, ALMBDs with unusual presentations should be determined by advanced imaging techniques such as CT, CBCT, MRI or sialography.13 To provide an accurate diagnosis of ABDs, 2D plain radiographs can be consolidated by 3D techniques for soft and hard tissue imaging. CT is one of the most effective methods for defining ABDs, determining the boundaries of these defects, and evaluating their relations with the surrounding tissues. CT images may be adequate to exclude the probable diagnosis of other pathologies, provide the final diagnosis, and define the content of the defect.9 Şişman et al showed that there is no difference between multi-slice CT and CBCT in the detection of ABDs. Also, Watanabe et al indicated that the diagnosis of ABDs with CT is useful.3,11
MRI has the advantage of being able to distinguish soft tissues in the region of interest, reveal salivary gland tissue, and avoid X-ray exposure. MRI also has some disadvantages, such as its high cost, claustrophobia, and probable artifacts owing to the presence of dental materials.3,12 Sialography can be difficult in practice and uncomfortable for the patient, and it exposes the patient to ionizing radiation. Contrary to posterior bone defects, conventional sialography of the sublingual gland provides limited value for the diagnosis of ABDs. Its use in ABDs is limited owing to the large number of Rivinus ducts that are smaller in diameter, making it difficult to perform the procedure.12
The late onset of ALMBD is a significant argument for dismissing theories that propose developmental defects during bone formation as the cause of mandibular bone depressions. The present case connects lingual mandibular defects to much earlier stages in life than typically expected. However, we were unable to precisely define the onset of this lesion because the present ALMBD was an incidental finding with no history of any other disease or developmental alteration in the region of interest. ALMBD is an idiopathic bone defect that can occasionally be diagnosed in children. Paediatric dentists should be careful and aware of this new entity.